Pvl imaging
Reading File
Finding Sources
Finding Sources
Searching PubMed
periventricular leukomalacia imaging MRI ultrasound
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
I now have all the information needed for a comprehensive answer. Here it is:
PVL (Periventricular Leukomalacia) - Imaging
PVL is the most common pattern of brain injury in preterm infants, representing white matter injury (WMI) adjacent to the lateral ventricles. It peaks in vulnerability between 23-32 weeks post-conceptional age and results from hypoxia-ischemia at vascular watershed/border zones in the periventricular white matter.
Two Forms of PVL
| Focal PVL (fPVL) | Diffuse PVL (dPVL) | |
|---|---|---|
| Pathology | Necrosis of all cell elements | Selective pre-oligodendrocyte injury + astrocytosis |
| Main lesion | Cystic necrosis (macrocysts/microcysts) | Hypomyelination, microstructural changes, gliosis |
| Outcome | More severe - spastic diplegia/quadriplegia | Cognitive, behavioral, visual impairments |
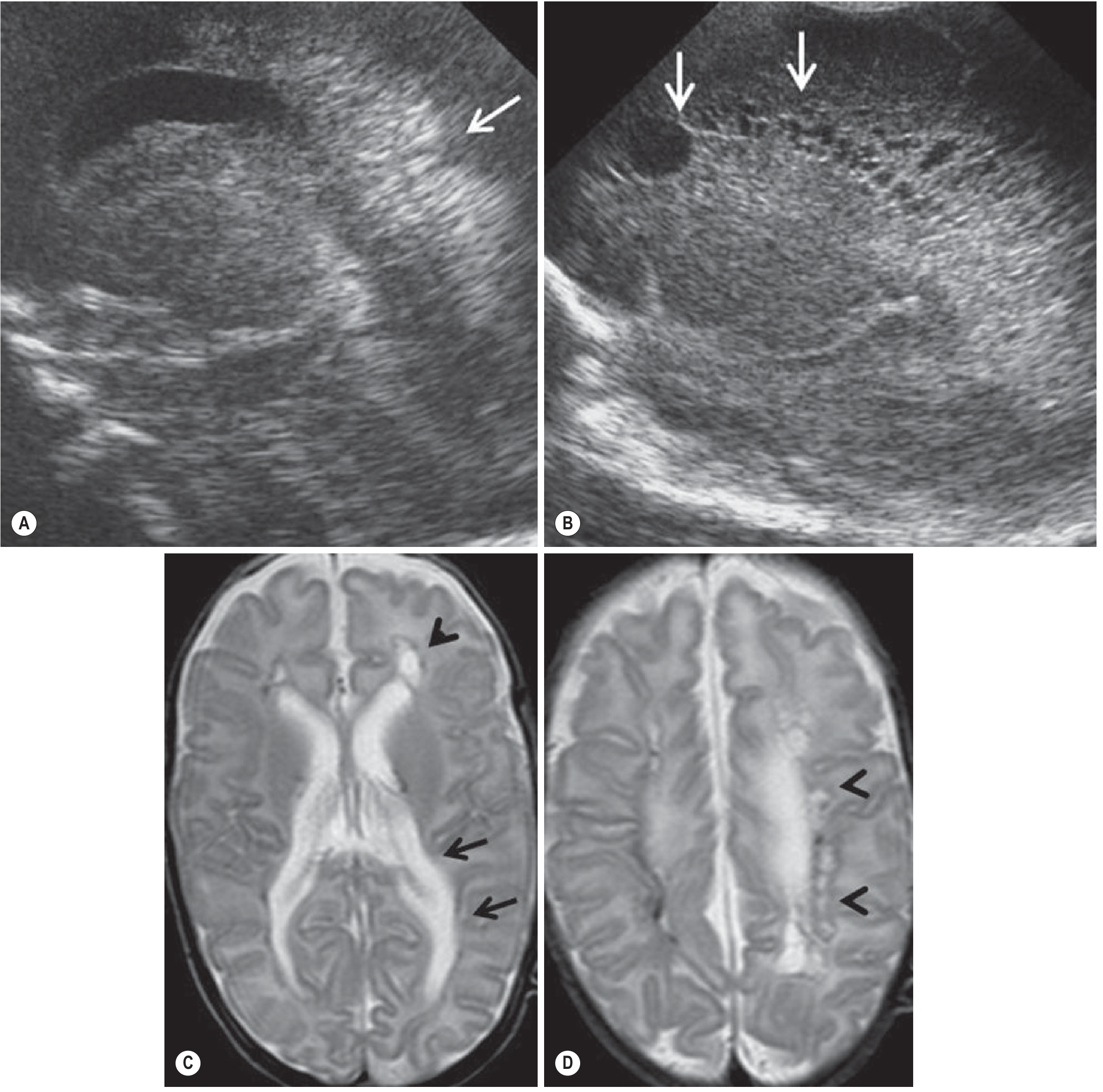
Cranial Ultrasound (US)
The first-line screening tool in neonates - radiation-free and repeatable through the anterior fontanelle.
Focal PVL (fPVL) sequence:
- Days 1-7: Periventricular hyperechogenic "flares" (increased echogenicity of white matter)
- Days 8-25: Flares evolve into coalescent macrocysts or microcysts within the periventricular white matter
Diffuse PVL (dPVL): Brain US is usually normal at initial stages - the main ultrasound limitation.
Important: Ultrasound often fails to identify subtle diffuse white matter injury. The true incidence of PVL is likely underestimated by US alone. MRI is more sensitive.
MRI Findings
MRI is more sensitive than US, especially for dPVL and diffuse/punctate WMI.
Acute/Subacute fPVL
- Restricted diffusion (DWI) within periventricular and deep white matter in the acute phase
- Cystic lesions: T1 low signal, T2 high signal, with central free diffusion (as opposed to restricted)
- Cysts coalesce, then are progressively resorbed over time
Established/Chronic fPVL
- Ventricular enlargement with an irregular outline of the body of lateral ventricles
- Thinning of periventricular white matter
- Focal signal abnormality extending from ventricular margins (especially posteriorly) - reflecting white matter gliosis
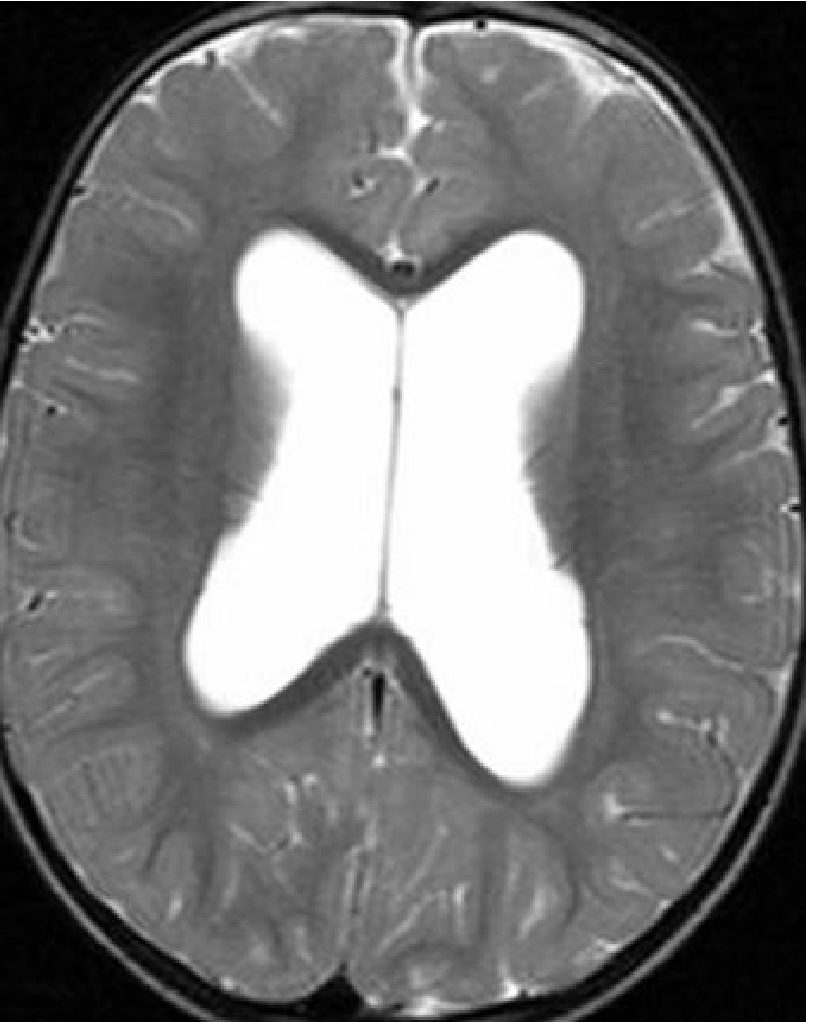
Diffuse PVL (dPVL) on MRI
- Ventriculomegaly with regular (smooth) outlines of the lateral ventricles
- Thinning of periventricular white matter without the irregular/cystic changes of fPVL
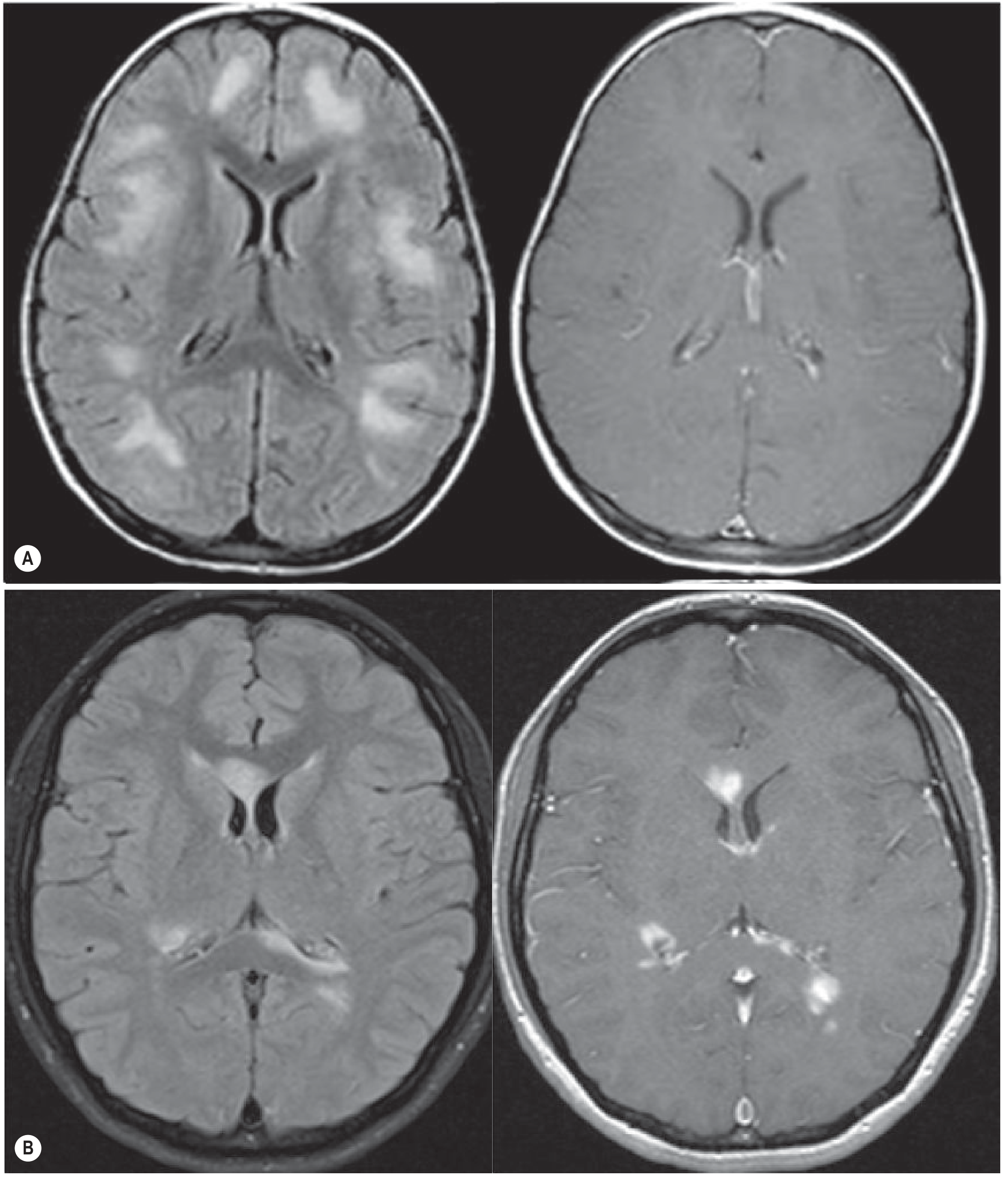
Punctate WMI (current predominant form)
In contemporary preterm cohorts, large cystic PVL is now uncommon. The current predominant lesion is punctate WMI - appearing as areas of signal hyperintensity on T1 (and hypointensity on T2) with a periventricular topology.
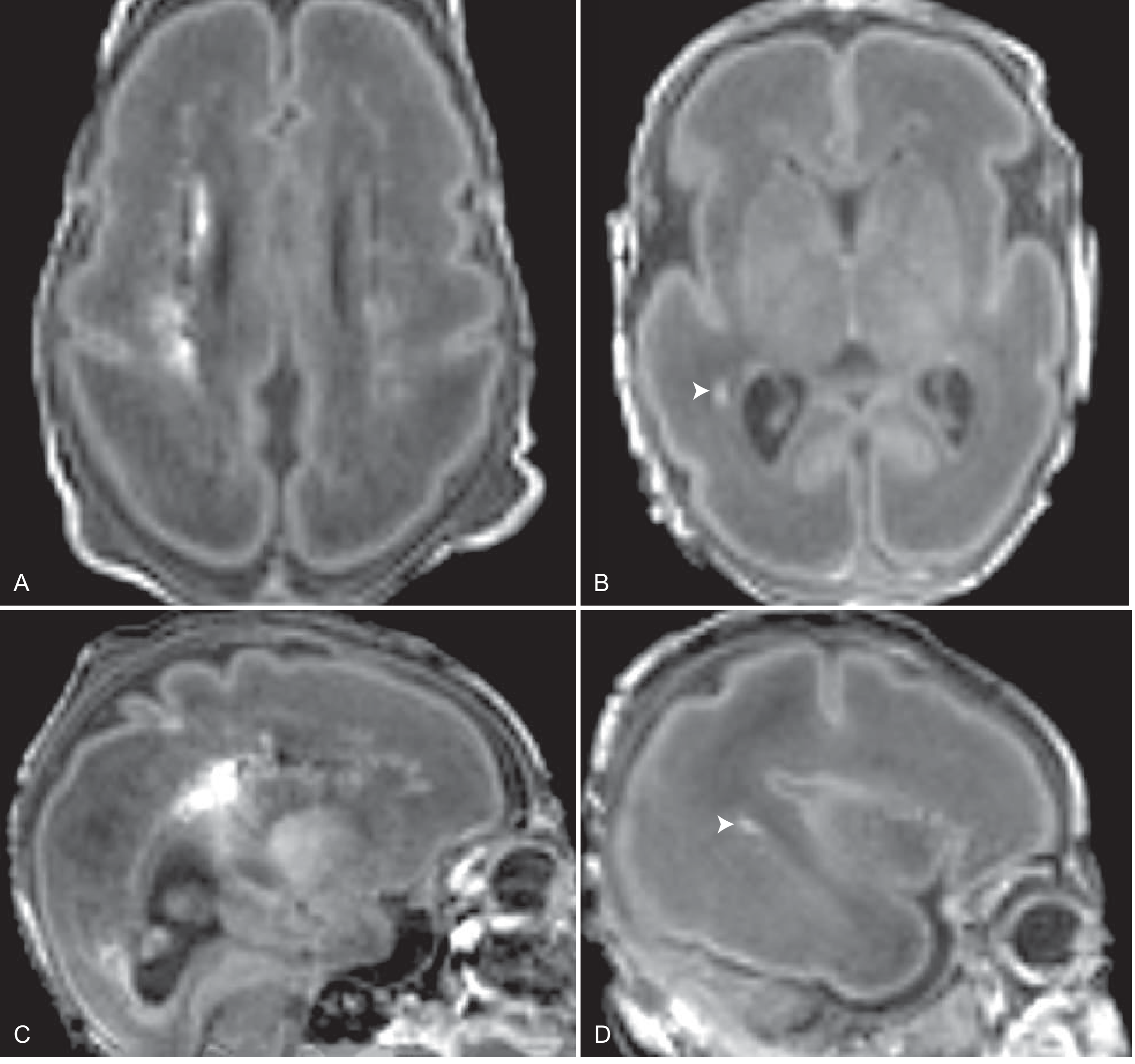
Prognostic MRI Marker
After corrected age of 1 month: abnormal signal intensity (low T1, high T2) in the posterior limb of the internal capsule predicts a poor motor outcome.
Summary: US vs MRI in PVL
| Feature | Cranial US | MRI |
|---|---|---|
| First-line use | Yes (screening, serial) | Reserved for neurological signs |
| fPVL detection | Good (flares → cysts) | Excellent (DWI, T1, T2) |
| dPVL detection | Poor (often normal) | Superior |
| Punctate WMI | Insensitive | Best modality |
| Motor outcome prediction | Insensitive | Better (PLIC signal) |
| Cognitive outcome prediction | Poor | Also poor (limitation of both) |
Clinical Context
- Incidence: Detected by US in 5-15% of very-low-birth-weight infants; true incidence higher
- Risk factors: IVH, cardiopulmonary instability, sepsis, hypocarbia, metabolic acidosis, placental abruption, twin-twin transfusion syndrome
- Sequelae: Spastic diplegia (most common - lower extremity motor fibers traverse periventricular area), or quadriplegia/cognitive/visual/auditory impairment with more severe injury
Sources: Grainger & Allison's Diagnostic Radiology; Creasy & Resnik's Maternal-Fetal Medicine; Bradley and Daroff's Neurology in Clinical Practice
Cerebral abscess imaging
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Here is the full answer:
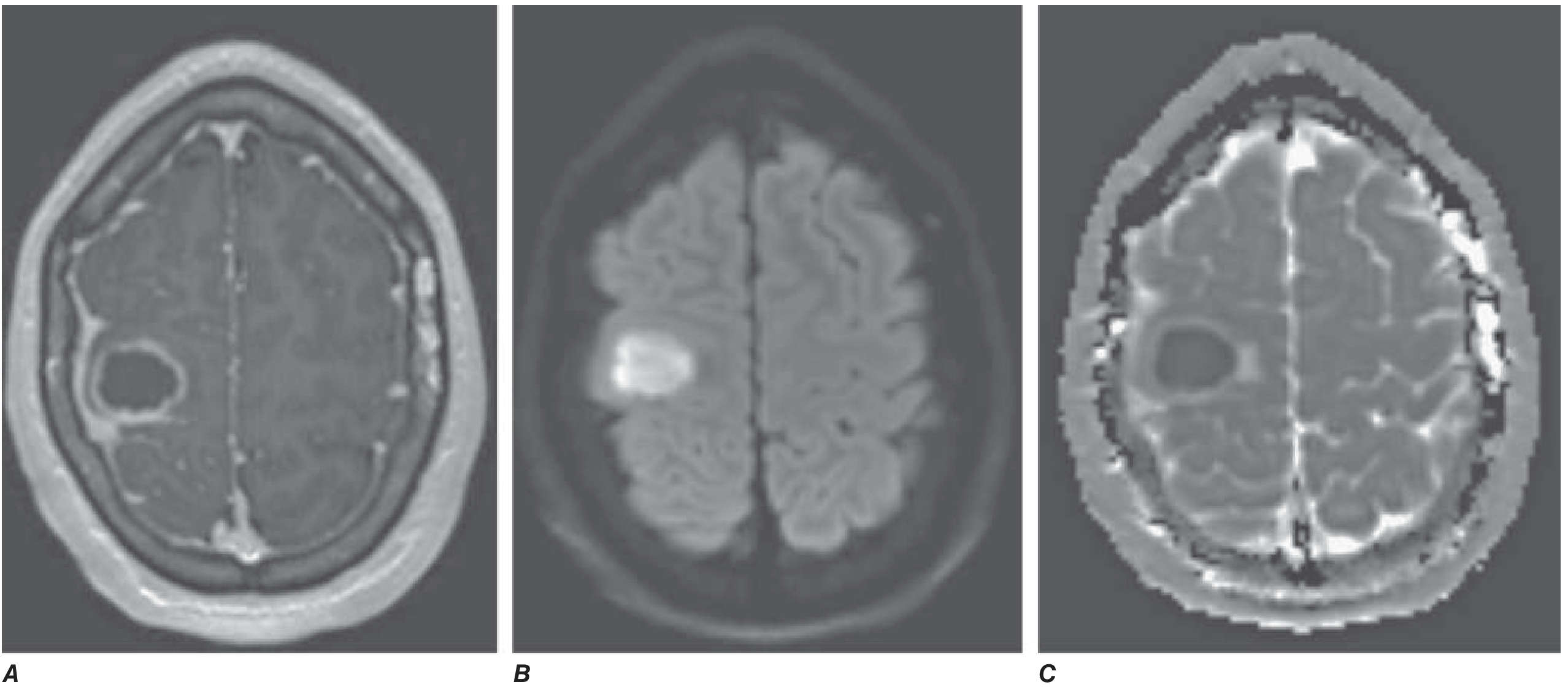
Cerebral Abscess - Imaging
A brain abscess is a focal collection of purulent material within the brain parenchyma, most commonly bacterial. It evolves through four defined stages, each with distinct imaging characteristics.
Stages of Abscess Formation
| Stage | Pathology | CT | MRI |
|---|---|---|---|
| Early cerebritis | Focal inflammation, no capsule | Ill-defined hypodensity; no/minimal enhancement | T1 low signal, irregular peripheral enhancement; T2 high signal |
| Late cerebritis | Coalescing necrosis, early capsule | Irregular peripheral enhancement, may progress centrally on delayed images | As above, more defined |
| Early capsule | Pus collection, capsule forming | Central hypodensity + ring enhancement + surrounding oedema | Ring enhancement, T2 hypointense rim, restricted diffusion in centre |
| Late capsule | Mature wall, fully formed | Smooth thin ring enhancement, medial wall thinner | All features maximally developed |
CT Findings
Cerebritis stage:
- Ill-defined area of low attenuation (hypodensity)
- Enhancement usually absent early; can appear irregular and peripheral in late cerebritis
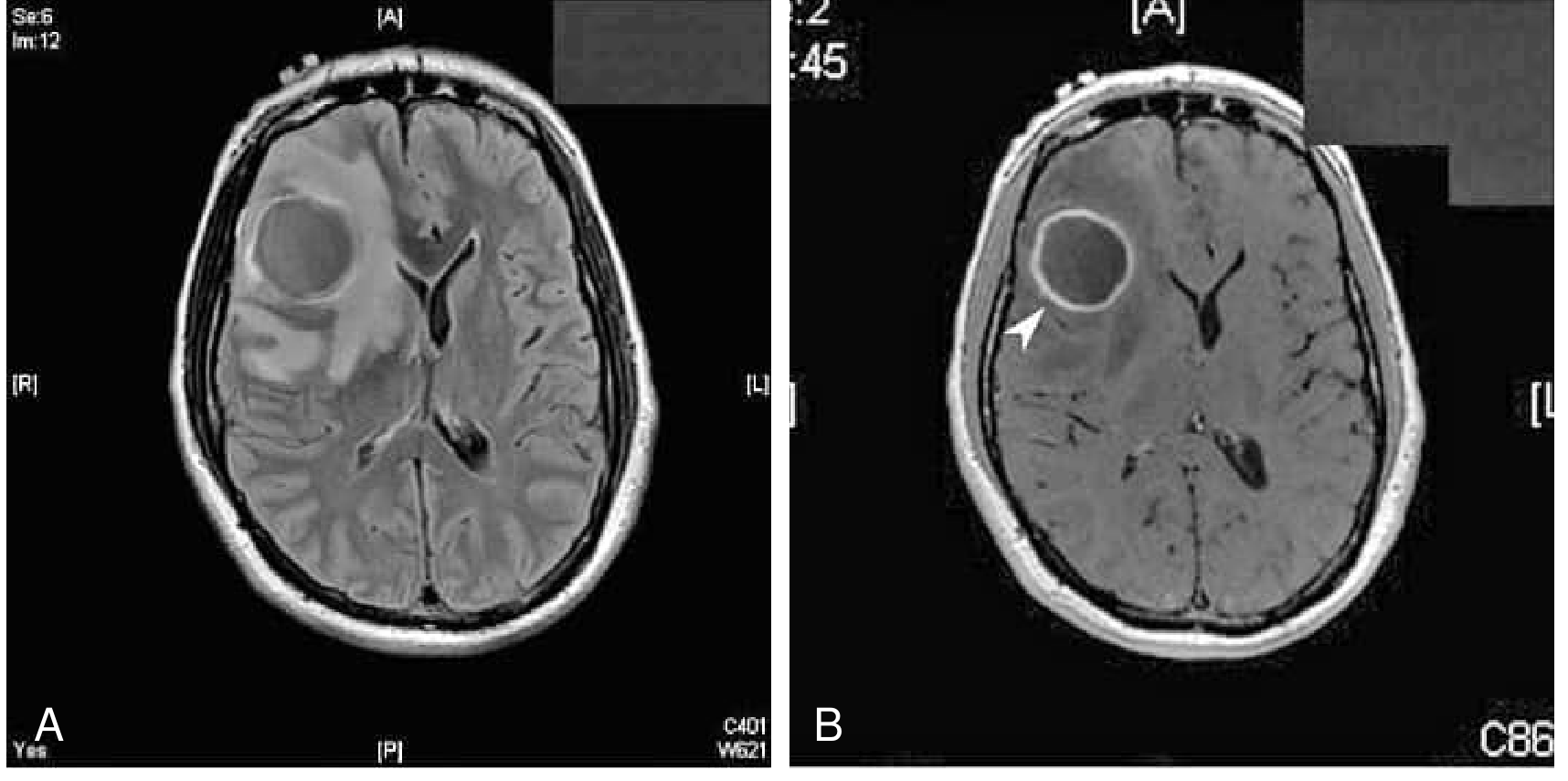
Mature (capsule stage):
- Central hypodensity (pus/necrotic debris)
- Rim of slightly higher attenuation surrounded by hypodense vasogenic oedema
- Ring enhancement after contrast - smooth inner margin, with characteristic thinning of the medial (deep/ventricular) wall
- Centre does NOT enhance on delayed images (unlike cerebritis)
- Gas within the abscess is rare - when present, suggests surgical intervention, sinus communication, or gas-forming organism
MRI Findings (Superior to CT)
MRI is better than CT for:
- Early cerebritis stage (CT often fails to show it)
- Posterior fossa abscesses
- Identifying satellite lesions and adjacent complications
Signal characteristics of mature abscess:
| Sequence | Centre (Pus) | Rim (Capsule) | Surrounding Oedema |
|---|---|---|---|
| T1 | Intermediate (between CSF and white matter) | Slightly hyperintense to white matter | Low signal |
| T2 | Iso- to slightly hyperintense to CSF | Hypointense (key feature) | High signal |
| FLAIR | Ring of low signal | Hypointense rim | High signal |
| T1 + Gad | No central enhancement | Smooth ring enhancement | No enhancement |
| DWI | Bright (high signal) | - | - |
| ADC | Dark (low signal) - restricted diffusion | - | - |
| SWI | - | Markedly hypointense (free radicals from phagocytosis); may show dual rim sign | - |
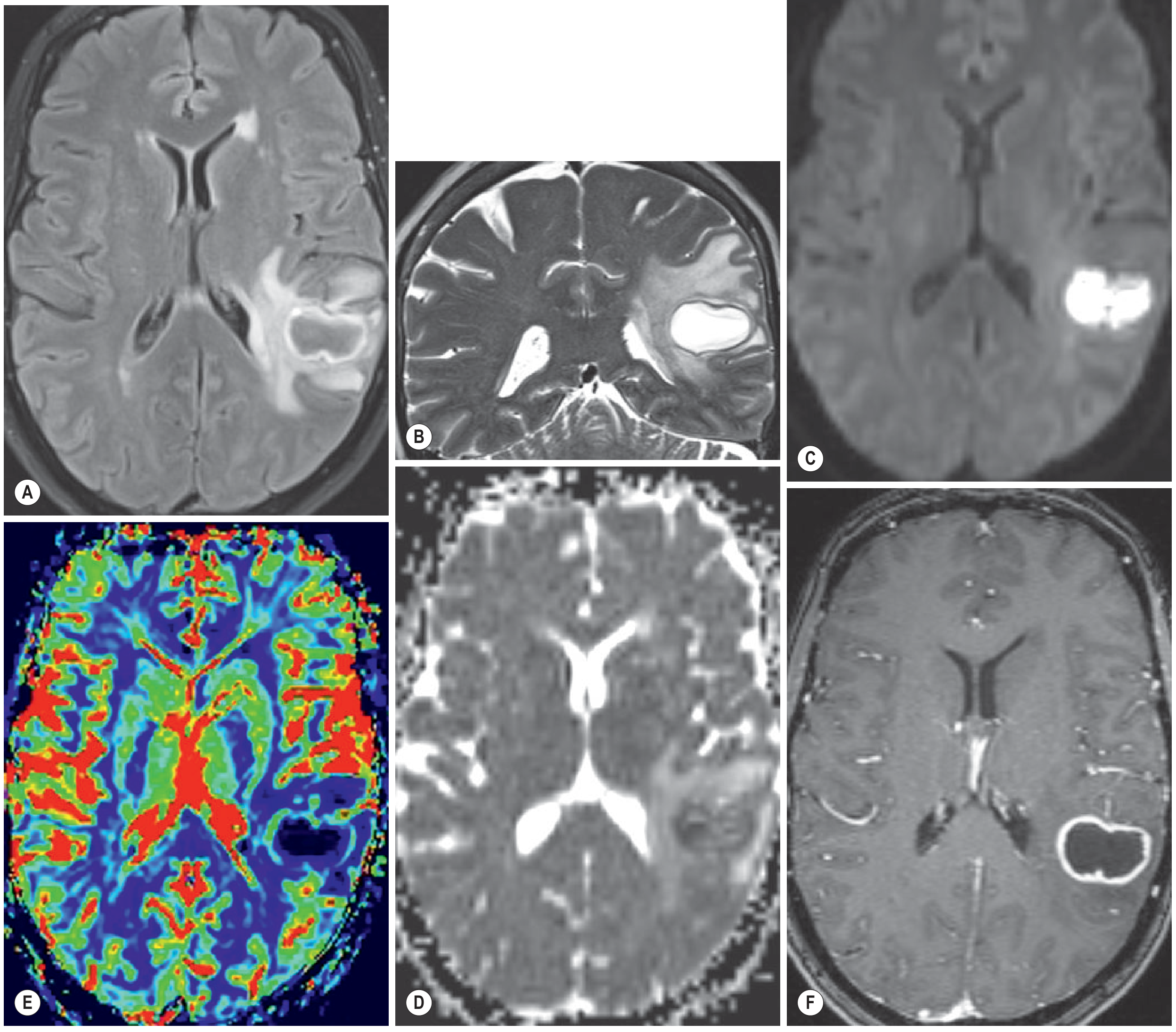
The Key DWI Finding - and Its Limitations
Restricted diffusion (DWI bright, ADC dark) in the abscess cavity is the most useful feature distinguishing abscess from ring-enhancing tumours (glioblastoma, metastasis), which typically show facilitated diffusion (dark on DWI).
- The degree of diffusion restriction is inversely correlated with the viable cell count inside the abscess
- Important caveat: restricted diffusion does NOT always reliably distinguish abscess from tumour - necrotic tumours and other lesions can occasionally show restricted diffusion
Location of Abscesses
Depends on source of infection:
- Frontal sinusitis → frontal lobe (directly beneath involved sinus)
- Mastoiditis/otitis media → temporal lobe or cerebellar hemisphere
- Haematogenous spread → predilection for gray-white matter junction (MCA territory, frontoparietal region); can occur anywhere
- Abscesses are multiple in 10-50% of cases
- Often subcortical or periventricular
- Frequently medial wall thinner than lateral wall (closer to ventricle, lower vascularity)
Differential Diagnosis of Ring-Enhancing Lesion
| Feature | Abscess | Glioblastoma | Metastasis |
|---|---|---|---|
| DWI centre | Bright (restricted) | Usually dark | Usually dark |
| Rim thickness | Thin, smooth, uniform | Thick, irregular | Thin but often nodular |
| Medial wall | Thinner | Irregular | Irregular |
| Satellite lesions | Common (small) | Less common | Multiple primaries |
| T2 rim | Hypointense | Isointense | Variable |
| SWI rim | Markedly hypointense | Variable | Variable |
A thick, irregular rim of enhancement is more suggestive of tumour. Abscess more likely shows small satellite lesions and a smooth inner margin.
Complications on Imaging
- Ventricular rupture: abscess breaks through medial wall into ventricle → ventriculitis (intraventricular debris, ependymal enhancement, FLAIR high signal within ventricles)
- Satellite abscesses: small additional ring lesions nearby
- Subdural empyema: crescentic fluid collection with restricted diffusion along the convexity or interhemispheric fissure
- Epidural abscess: lentiform extra-axial collection, can cross midline (unlike subdural)
Follow-up Imaging
- Recommended at biweekly intervals or when new symptoms arise
- Adequate treatment: resolution of rim enhancement or disappearance of T2 hypointense rim
- DWI superior to conventional MRI for monitoring response: low DWI signal = good response; increasing DWI signal = reaccumulation of pus
Sources: Grainger & Allison's Diagnostic Radiology; Harrison's Principles of Internal Medicine 22E; Bradley and Daroff's Neurology in Clinical Practice; Goldman-Cecil Medicine
Demyelinating cns imaging
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content across MS, NMO, ADEM, and tumefactive MS. Let me compile the full answer.
Demyelinating CNS Disease - Imaging
Demyelinating diseases of the CNS form a spectrum of conditions. MRI is the cornerstone of diagnosis for all of them. The key entities are: Multiple Sclerosis (MS), Neuromyelitis Optica Spectrum Disorder (NMOSD), Acute Disseminated Encephalomyelitis (ADEM), and Tumefactive MS.
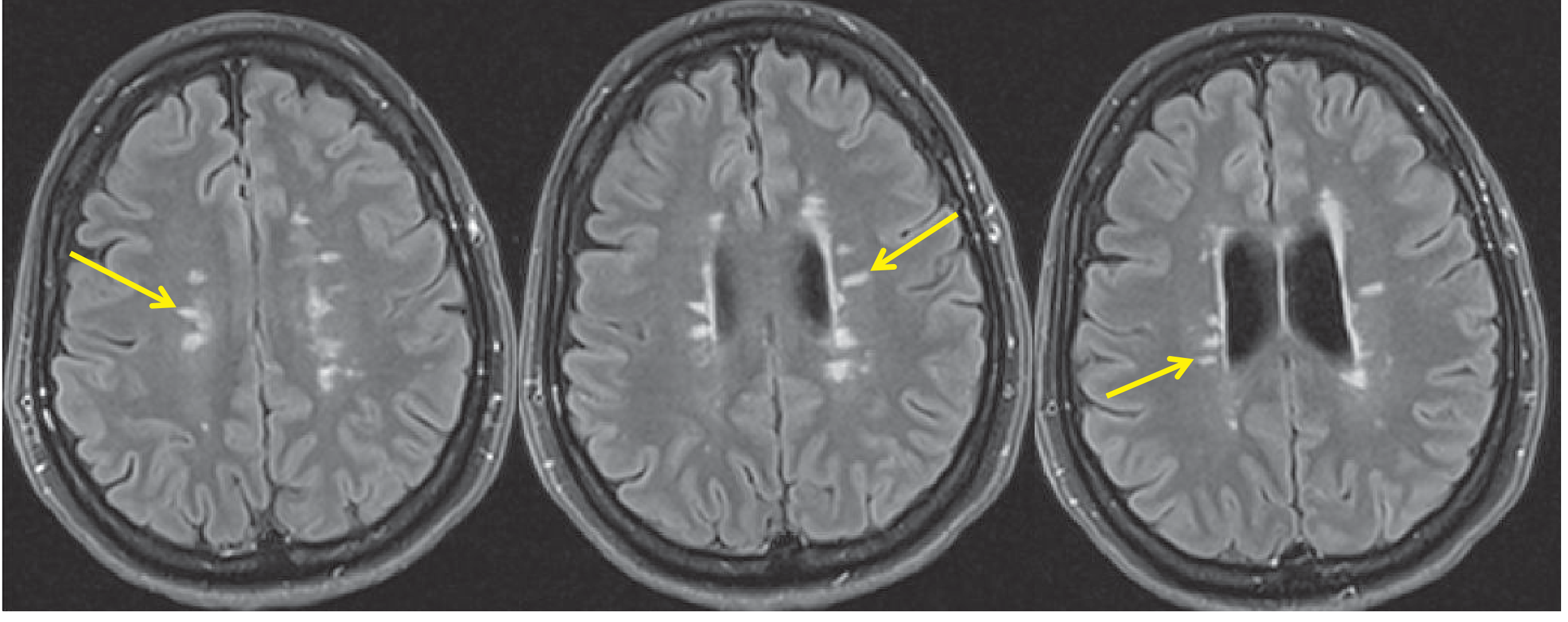
1. Multiple Sclerosis (MS)
MRI Lesion Characteristics
MS lesions are T2/FLAIR hyperintense plaques, seen in 98% of MS patients in the periventricular white matter. They are the backbone of diagnosis using the 2017 McDonald Criteria.
Morphology:
- Round to oval, typically a few mm to >1 cm
- Discrete and focal early; confluent in advanced disease, especially in posterior periventricular white matter
- Centred on medium-sized veins - "Dawson fingers": ovoid periventricular lesions whose major axis is perpendicular to the outer surface of the lateral ventricles (best seen on sagittal FLAIR)
- Central vein sign: visible on SWI - central punctate hypointensity within MS lesions (reflecting the perivenular origin); less frequent in non-MS white matter lesions
Characteristic Locations (McDonald Criteria Regions)
| Region | Specific Site |
|---|---|
| Periventricular | Superolateral to lateral ventricular angles (most common) |
| Juxtacortical | U-fibre involvement at cortex-WM junction |
| Infratentorial | Floor/surface of 4th ventricle, medial longitudinal fasciculus, pons surface, cerebellar peduncles |
| Corpus callosum | Inferior margin (calloso-septal interface) |
| Spinal cord | Cervical > thoracic; short-segment, peripheral, lateral/dorsal columns |
| Optic nerves | Fat-suppressed T1 / STIR hyperintensity; enhancement in acute optic neuritis |
Posterior fossa lesions preferentially affect the floor of the 4th ventricle, pons surface, intrapontine trigeminal tract, and cerebellar peduncles - unlike ischaemic lesions which involve central pontine WM.
Signal Characteristics by Sequence
| Sequence | MS Plaque |
|---|---|
| T2 / FLAIR | Hyperintense (cornerstone sequence) |
| T1 | Intermediate-low (most lesions) |
| T1 "black holes" | Hypointense < grey matter = axonal loss / severe demyelination; present in <40% of lesions (chronic irreversible damage) |
| T1 + Gad | Nodular/homogeneous or ring-like enhancement (active/acute lesions only); open-ring pattern characteristic of MS |
| SWI | Central vein sign (perivenular); hypointense rim in chronic lesions (iron deposition in activated microglia) |
| DWI | Can show restricted diffusion in acute demyelination |
Enhancement Patterns
- Nodular/homogeneous: common, especially small active lesions
- Ring enhancement in larger lesions - the MS ring is characteristically incomplete/open ring with the open margin facing cortical grey matter (unlike tumours and abscess which form complete rings)
- Simultaneous coexistence of enhancing and non-enhancing lesions is the rule in RRMS and is a key diagnostic clue
Spinal Cord MS
- Short-segment lesions: less than 2 vertebral segments (vs NMOSD which is ≥3)
- Less than half the cross-sectional diameter of the cord
- Peripheral location: predominantly lateral and dorsal columns
- Cervical region most commonly affected
- In progressive MS: diffuse subtle T1/PD/STIR abnormality and cord atrophy
2017 McDonald Criteria - MRI Requirements
Dissemination in Space (DIS): ≥1 T2 lesion in ≥2 of: periventricular, juxtacortical/cortical, infratentorial, spinal cord
Dissemination in Time (DIT): simultaneous enhancing + non-enhancing lesions, OR new T2/enhancing lesion on follow-up MRI
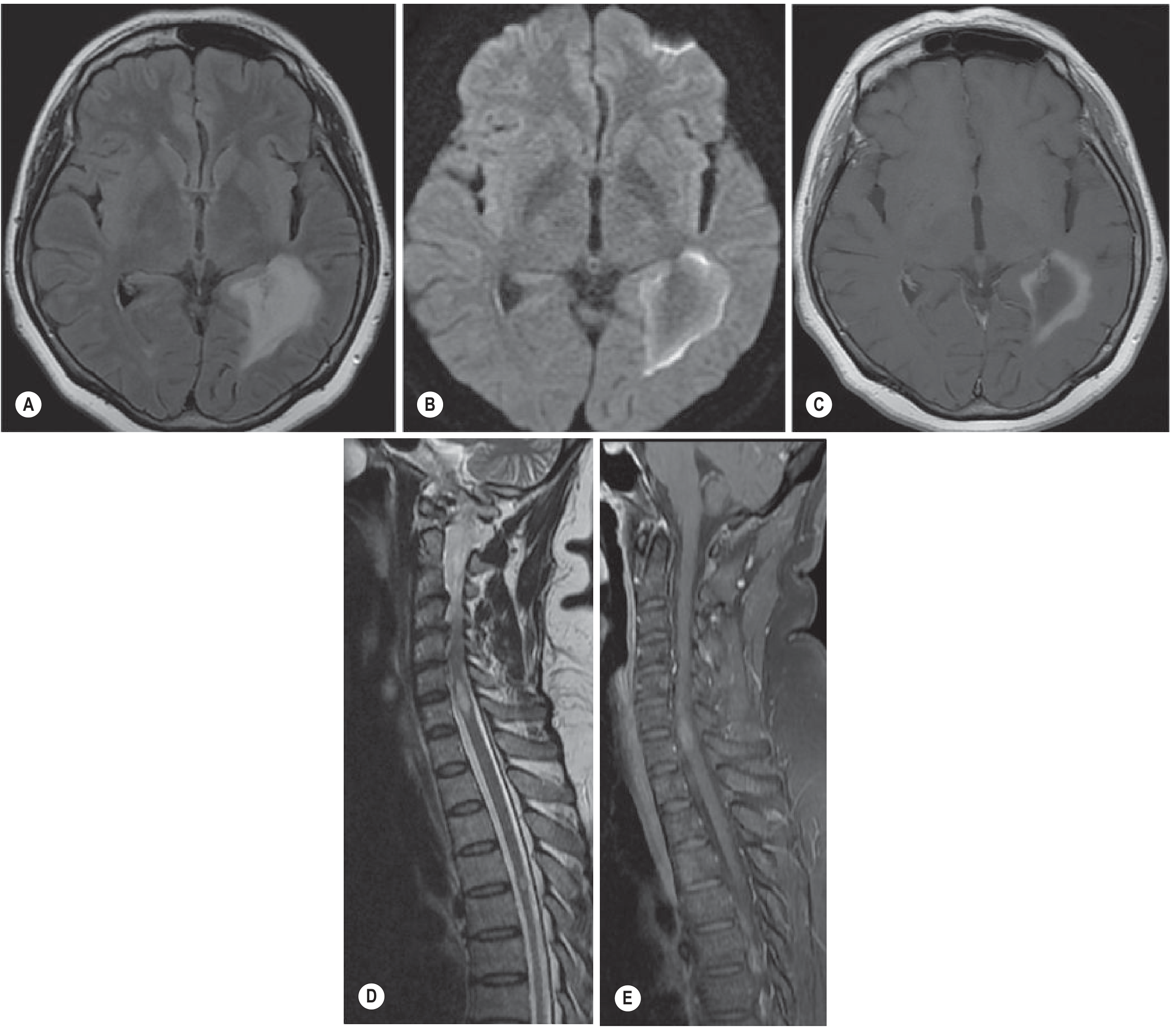
2. Neuromyelitis Optica Spectrum Disorder (NMOSD)
NMOSD (AQP4-IgG positive in most) has characteristic imaging that differs from MS in important ways.
Spinal Cord - Key Features
- Longitudinally extensive transverse myelitis (LETM): T2 hyperintensity extending ≥3 vertebral segments (vs <2 in MS)
- Enhancement in up to 90%; cervical cord: "shaggy ring enhancement" in ~30%
- Axial T2: "bright spotty lesions" = highly specific for NMO (reflects destructive inflammation)
- Progresses to atrophy, necrosis, and syrinx-like cavities on T1
Brain - NMO Features (distinct from MS)
- Lesions at sites of high AQP4 expression (circumventricular organs):
- Periependymal areas around 3rd and lateral ventricles
- Hypothalamus
- Periaqueductal grey
- Dorsal brainstem / area postrema (4th ventricle floor) - explains intractable vomiting/hiccup
- Corpus callosum: ependymal surface, "arch bridge" or marbled oedematous appearance
- Corticospinal tracts (posterior internal capsule → cerebral peduncle → longitudinally extensive)
- Enhancement: "cloud-like" - multiple patches with blurred margins (vs MS nodular/ring)
- No central vein sign on SWI (unlike MS)
- No hypointense rim on SWI (unlike chronic MS)
MS vs NMOSD - Key Imaging Differences
| Feature | MS | NMOSD |
|---|---|---|
| Spinal cord lesion length | Short (<2 segments) | Long (≥3 segments) |
| Cord T2 appearance | Peripheral focal | Bright spotty lesions |
| Cord location | Peripheral (lateral/dorsal) | Central |
| T1 cord signal | Normal | Hypointense (destructive) |
| Brain lesion distribution | Periventricular, corpus callosum inferior | AQP4 sites: area postrema, hypothalamus, 3rd/4th ventricle |
| Corpus callosum | Inferior/calloso-septal | Ependymal surface, "arch bridge" |
| Enhancement type | Nodular/open ring | Cloud-like |
| Central vein sign (SWI) | Yes | No |
| SWI hypointense rim | Chronic lesions | No |
| Optic nerve | Short segment | Entire length, chiasm involvement |
3. Acute Disseminated Encephalomyelitis (ADEM)
Predominantly a paediatric condition (peak age 5-8 years), following viral infection or vaccination.
Brain MRI
- Large, patchy, poorly marginated lesions (vs MS: small, well-defined)
- Predominant subcortical location with asymmetric hemispheric white matter involvement
- Often bilateral thalamic and basal ganglia involvement (helps distinguish from MS)
- Diffuse pontine involvement common
- Monophasic: no new lesions after 3 months on follow-up MRI (in contrast to MS)
- Complete MRI resolution within 6 months → favours ADEM diagnosis
- Persistence/new lesions after 3 months → suggests subsequent MS diagnosis
Enhancement in ADEM
- Gadolinium enhancement is uncommon (14-30%) overall
- When present, all lesions typically enhance simultaneously (unlike MS where enhancing and non-enhancing lesions coexist)
- Patterns: complete/incomplete ring, nodular, gyral, or spotty
- A normal brain MRI within the first few days does not exclude ADEM
Spinal Cord in ADEM
- Affected in one-third of patients, predominantly thoracic
- LETM: large, multi-segment lesions with cord swelling (like NMOSD, unlike MS)
- Variable enhancement; may affect grey matter, white matter, or both
4. Tumefactive MS
A large (>2 cm) demyelinating MS plaque that mimics a brain tumour on imaging.
- FLAIR: large hyperintense lesion, relatively well-defined, little mass effect for its size
- DWI: peripheral restricted diffusion (rim of restriction at the active demyelinating edge) - distinct from abscess (central restriction) and glioblastoma (variable)
- Post-contrast T1: open/incomplete ring enhancement with the open border facing cortical grey matter - the defining feature separating it from glioblastoma and metastasis (which show complete rings)
- Other MS lesions typically present elsewhere in the brain (key diagnostic clue)
Summary Comparison Table
| Feature | MS | NMOSD | ADEM | Tumefactive MS |
|---|---|---|---|---|
| Age | 20-40s | Any (F predominant) | Children (peak 5-8y) | Any |
| Brain lesions | Small, periventricular | AQP4 sites | Large, subcortical, poorly marginated | Single large lesion |
| DWI | Variable | Variable | Variable | Peripheral restriction |
| Enhancement | Open ring / nodular | Cloud-like | All lesions simultaneously | Open ring |
| Spinal cord | Short segment, peripheral | LETM, central, destructive | LETM with swelling | Short segment |
| Central vein (SWI) | Yes | No | No | No |
| Course | Relapsing/progressive | Relapsing, severe | Monophasic | Monophasic (often) |
| New lesions >3 months | Yes | Yes | No | Depends |
Sources: Grainger & Allison's Diagnostic Radiology; Harrison's Principles of Internal Medicine 22E; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.