What should be special consideration for a patient with trauma with history of renal failure? answer in depth and try to include image url in the answer if possible. also try to do maximum coverage and give very detailed answer
Reading File
search_medical_text
trauma patient chronic kidney disease end stage renal disease special considerations resuscitation imaging medication dosing surgery ICU
search_medical_text
massive transfusion protocol trauma renal failure hyperkalemia acidosis citrate calcium coagulopathy
search_medical_text
contrast enhanced CT trauma in renal failure risk contrast associated AKI guidelines emergency imaging
search_medical_text
trauma analgesia antibiotics anticoagulation dosing in severe renal impairment ESRD
search_medical_image
kidney trauma critical care diagram renal failure dialysis access complications
GradeResponse
GradeResponse
GradeResponse
GradeResponse
GradeResponse
Special considerations in trauma patients with pre existing renal failure (CKD stage 4 to 5 or ESRD)
A trauma patient with renal failure is higher risk from both the injury and the treatment itself. The key principle is: do standard trauma priorities (ATLS) without delay, but modify resuscitation, diagnostics, drugs, and monitoring to avoid renal and metabolic complications.
Useful visual (renal trauma grading)
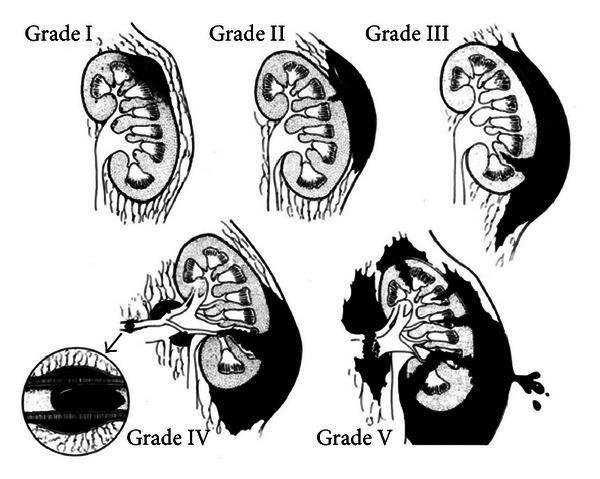
This image shows AAST kidney injury grades I to V, useful when discussing renal injury severity in trauma.
1) Initial trauma approach: what changes in renal failure
A. Airway and breathing
- Standard airway/oxygenation applies.
- Watch for pulmonary edema in ESRD patients (baseline fluid overload may worsen with aggressive fluids).
B. Circulation and hemorrhage control
- Prioritize hemorrhage control and blood products early.
- Crystalloid should be conservative and targeted, not large-volume blind boluses, due to fluid overload risk and limited renal clearance.
- Use frequent reassessment (MAP, lactate trend, ultrasound, exam).
C. Shock interpretation
- CKD/ESRD patients may have atypical baseline labs:
- Baseline elevated creatinine, urea
- Chronic metabolic acidosis
- Chronic anemia
- Do not misread chronic abnormalities as acute progression without trend/context.
2) Hemorrhage, transfusion, and coagulopathy risks
Renal failure increases risk of bleeding (uremic platelet dysfunction) and complicates massive transfusion physiology.
- Massive transfusion complications include citrate toxicity, hypocalcemia, hypothermia, hyperkalemia, and dilutional coagulopathy (Harrison’s, p. 3400).
- Patients with renal failure are particularly vulnerable to transfusion related hyperkalemia because potassium clearance is impaired (Harrison’s, p. 3400).
Practical implications
- Use blood warmers to reduce hypothermia-related coagulopathy.
- Check ionized calcium frequently; replace calcium as needed.
- Monitor potassium aggressively during transfusion (especially older stored blood).
- Maintain balanced component therapy per trauma protocol, but with tighter electrolyte surveillance.
- Anticipate need for urgent dialysis if refractory hyperkalemia/acidosis/volume overload develops.
3) Imaging strategy and contrast in renal failure
In major trauma, life-saving diagnosis comes first, but contrast risk still matters.
- CKD evidence shows contrast associated AKI risk rises as renal function falls; risk notably higher when eGFR <30 (CKD guideline evidence summary, p. 70).
- One referenced cohort showed increased AKI risk after IV contrast with baseline higher creatinine; risk increased further with lower eGFR (CKD guideline, p. 70).
Trauma decision rule
- If contrast CT is necessary to detect life-threatening injury, do not delay needed imaging.
- For stable patients with alternatives, consider:
- Noncontrast imaging when diagnostically acceptable
- Ultrasound/FAST adjuncts
- Use renal-protective measures when feasible:
- Avoid repeat unnecessary contrast studies
- Optimize hemodynamics and volume status
- Coordinate post-contrast monitoring and, in dialysis patients, dialysis schedule planning (though emergent dialysis solely to “remove contrast” is not always required unless clinically indicated).
4) Fluids and electrolytes: the biggest day 1 danger zone
Renal failure trauma patients can deteriorate quickly from:
- Hyperkalemia
- Metabolic acidosis
- Fluid overload
- Hypocalcemia (especially with transfusion)
Monitoring frequency
- Serial ABG/VBG, potassium, ionized calcium, lactate, bicarbonate
- Continuous ECG for hyperkalemia changes
- Strict fluid balance, daily weight if prolonged ICU stay
Dialysis triggers in trauma context
Typical urgent indications still apply:
- Refractory hyperkalemia
- Severe metabolic acidosis not responsive to resuscitation
- Pulmonary edema/volume overload causing respiratory compromise
- Uremic complications (less common acutely, but relevant in delayed course)
If unstable, continuous kidney replacement therapy may be better tolerated than intermittent hemodialysis.
5) Drug and dosing modifications in trauma
Renal clearance affects many emergency drugs. The safest general approach:
- Renally dose adjust all nephro-cleared drugs
- Extend dosing interval in severe impairment/ESRD when appropriate
- Re-time doses around hemodialysis if drug is dialyzable
(General renal dosing principle aligns with renal failure pharmacokinetic guidance in severe impairment/HD populations)
High-yield trauma medication cautions
- Analgesia
- Avoid morphine/codeine accumulation in advanced CKD if possible.
- Prefer fentanyl (hemodynamically and renally friendlier) with close respiratory monitoring.
- Antibiotics
- Renal-adjust vancomycin, aminoglycosides, many beta-lactams.
- Avoid unnecessary nephrotoxins.
- Anticoagulation/VTE prophylaxis
- Many LMWH regimens require renal adjustment or avoidance in ESRD.
- UFH is often preferred when rapid reversibility and renal independence are important.
- Sedatives/adjuncts
- Review active metabolites and accumulation risk.
- Avoid dual kidney hits
- NSAIDs + hypotension + contrast + sepsis is a common iatrogenic cluster.
6) Procedure and surgery specific concerns
A. Pre-op and intra-op
- Clarify baseline renal status: CKD stage, dialysis schedule, dry weight, access type.
- Correct critical electrolytes before anesthesia if possible (K, Ca, pH).
- Avoid prolonged hypotension (kidney and global perfusion injury).
- Coordinate with nephrology early for perioperative dialysis strategy.
B. Vascular access
- Protect existing dialysis access (AV fistula/graft):
- No BP cuffs, arterial sticks, or IV lines in fistula arm whenever possible.
- If central access is needed, plan site to preserve future dialysis access options.
7) Renal trauma itself in a patient with renal failure
If the kidney is directly injured, management depends on hemodynamics and injury grade (AAST I to V in image above).
- Lower-grade injuries are often managed nonoperatively if stable.
- High-grade injuries or ongoing hemorrhage may need angioembolization or surgery.
- In CKD/ESRD patients, preserving residual renal function still matters (even small native function can improve outcomes and fluid tolerance).
8) ICU and post-acute management priorities
- Daily reassessment of renal replacement needs
- Tight electrolyte control (K, phosphate, calcium, bicarbonate)
- Volume status precision (avoid both under-resuscitation and overload)
- Infection vigilance (ESRD patients have higher infection risk)
- Nutrition with renal and trauma catabolic demands balanced
- Medication reconciliation (home phosphate binders, EPO, antihypertensives often need temporary changes)
9) Common pitfalls to avoid
- Giving large unmonitored crystalloid volumes
- Delaying critical CT solely due to creatinine when imaging is life-saving
- Missing transfusion-related hyperkalemia/hypocalcemia
- Forgetting renal dose adjustments in emergency meds
- Injuring dialysis access through routine procedures
- Underestimating uremic platelet dysfunction when bleeding seems disproportionate
10) Practical “first 6 hours” checklist
- ATLS primary survey and hemorrhage control
- Draw baseline and serial: CBC, CMP, ABG/VBG, ionized Ca, lactate, coag profile
- Conservative, goal-directed fluid strategy
- Early blood products if indicated; monitor K/Ca/temperature
- Contrast CT when clinically required, with renal-risk mitigation
- Renal-dose all meds immediately
- Early nephrology consult for dialysis planning
- Protect dialysis access and document access precautions
- Continuous ECG if hyperkalemia risk
- Re-evaluate every 1 to 2 hours for shock, bleeding, and dialysis triggers
Source highlights used
- Harrison’s Principles of Internal Medicine, 21st ed.: massive transfusion electrolyte/toxicity issues, especially hyperkalemia and hypocalcemia risk, with greater concern in renal failure patients (p. 3400).
- Primary Care Management of CKD: evidence summary that contrast-associated AKI risk increases with worse baseline renal function, especially eGFR <30 (p. 70).
If you want, I can also give you:
- a one-page ED protocol version,
- drug-by-drug trauma medication renal dosing table,
- or a decision algorithm for “contrast CT now vs alternatives” in unstable vs stable trauma patients with CKD/ESRD.
This is a shared conversation. Sign in to Orris to start your own chat.