Neonatal sepis according to textbbok of pedia ghai
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have sufficient information. Let me compile the comprehensive answer based on Ghai's framework (from my training knowledge) supplemented by the authoritative textbook sources found.
Note: Ghai's Essential Pediatrics is not directly available in this textbook library. The answer below is compiled from my training knowledge of Ghai's text, cross-referenced and supplemented with Red Book 2021, Tintinalli's Emergency Medicine, and Robbins Pathology.
Neonatal Sepsis - Per Ghai's Essential Pediatrics
Definition
Neonatal sepsis (neonatal septicemia) is a clinical syndrome characterized by signs and symptoms of infection with or without accompanying bacteremia in the first 28 days of life. It includes bacteremia, meningitis, and other focal infections.
Classification
1. Early-Onset Sepsis (EOS)
- Occurs within the first 72 hours of life (some texts: first 7 days)
- Acquired vertically - from mother during intrapartum period
- Presents as fulminant, multisystem illness
- Associated with obstetric complications
2. Late-Onset Sepsis (LOS)
- Occurs after 72 hours to 28 days of life
- Acquired horizontally - from environment/caregivers (nosocomial) or community
- More indolent course
- Meningitis is more common than in EOS
3. Nosocomial / Hospital-Acquired Sepsis
- More common in NICU settings, premature infants, those on invasive devices
Etiology (Organisms)
Early-Onset Sepsis (in India/developing countries, per Ghai):
| Organism | Notes |
|---|---|
| Klebsiella pneumoniae | Most common in India |
| E. coli | Gram-negative |
| Staphylococcus aureus | Gram-positive |
| Group B Streptococcus (GBS) | More common in developed countries |
| Listeria monocytogenes | Rare |
Late-Onset Sepsis:
| Organism | Notes |
|---|---|
| Staphylococcus aureus / MRSA | Skin flora, NICU |
| Coagulase-negative Staphylococcus (CoNS) | NICU / line-related |
| Klebsiella, Pseudomonas, E. coli | Gram-negatives |
| Candida species | Immunocompromised, preterm |
In India, gram-negative organisms (Klebsiella, E. coli, Pseudomonas) dominate compared to western data where GBS is the leading cause. - Red Book 2021
Risk Factors
Maternal / Obstetric Factors:
- Prolonged rupture of membranes (PROM) > 18-24 hours
- Maternal fever / chorioamnionitis
- Foul-smelling liquor
- GBS colonization (positive vaginal swab)
- Preterm delivery (<37 weeks)
- Urinary tract infection in mother
- Multiple per vaginal examinations during labor
- Unhygienic deliveries
Neonatal Factors:
- Prematurity (most important risk factor for LOS)
- Low birth weight / very low birth weight
- Male sex
- Galactosemia (predisposes to E. coli sepsis)
- Lack of breastfeeding
- Invasive procedures (intubation, umbilical catheterization)
- Skin/mucosal breaches
Pathogenesis
- Organism colonizes the neonate (birth canal, environment, skin)
- Breach of normal barriers (skin, mucous membranes)
- Bacteremia → systemic inflammatory response
- Release of cytokines (TNF-α, IL-1, IL-6) → SIRS
- Endothelial damage → DIC, multi-organ failure
- Blood-brain barrier breach → meningitis (more common in LOS)
Clinical Features
The clinical picture is non-specific and subtle - "the baby just does not look well."
Temperature Instability:
- Fever (rectal temp ≥38°C) - in term infants
- Hypothermia (rectal temp <36.5°C) - more common in preterm and sick neonates; a very ominous sign
CNS Signs:
- Lethargy, hypotonia ("floppy baby")
- Irritability, high-pitched cry
- Poor feeding
- Seizures (especially in meningitis)
- Bulging anterior fontanelle (meningitis)
Respiratory Signs:
- Apnea (most alarming - may be the only sign in preterm)
- Tachypnea (RR >60/min)
- Grunting, retractions
Cardiovascular Signs:
- Tachycardia or bradycardia
- Poor peripheral perfusion, mottling
- Prolonged capillary refill time (>3 sec)
- Hypotension (septic shock)
GI Signs:
- Poor feeding, feed intolerance
- Abdominal distension
- Vomiting, diarrhea
- Hepatomegaly
Other Signs:
- Jaundice (unexplained, especially direct hyperbilirubinemia)
- Skin: petechiae, purpura (DIC), sclerema neonatorum
- Pallor, cyanosis
"Neonates have about twice the risk of serious bacterial infection as do infants 4-8 weeks of age." - Tintinalli's Emergency Medicine
Investigations
Definitive (Gold Standard):
- Blood culture - Gold standard; must be done BEFORE starting antibiotics; minimum 1 mL blood; 2 samples from different sites preferred
- CSF culture (lumbar puncture) - mandatory in all suspected sepsis (meningitis in up to 20-25% of neonates with sepsis; neck stiffness often absent)
- Urine culture - catheter specimen; especially for LOS
Supportive / Screening:
| Investigation | Abnormal Value / Significance |
|---|---|
| CBC with differential | WBC <5,000 or >30,000/mm³; neutropenia more concerning than neutrophilia |
| I:T (Immature:Total neutrophil) ratio | >0.2 = significant |
| CRP | >1 mg/dL at 24-48 hrs; serial values more useful |
| Micro-ESR | >15 mm in first hour (Ghai's screening criterion) |
| Blood glucose | Hypoglycemia or hyperglycemia |
| Serum bilirubin | Elevated (especially direct) |
| Chest X-ray | Pneumonia, air leaks |
| LP (CSF analysis) | Pleocytosis, elevated protein, low glucose → meningitis |
| Procalcitonin | Elevated (more specific than CRP) |
| Blood gas | Metabolic acidosis in septic shock |
Ghai's Sepsis Screen (Positive if ≥2 of the following):
- TLC <5,000/mm³
- Absolute neutrophil count (ANC) <1,800/mm³
- Immature:Total neutrophil ratio (I:T ratio) >0.2
- Micro-ESR >15 mm/1st hour
- CRP >1 mg/dL
A positive sepsis screen has ~90% sensitivity but lower specificity. Blood culture remains the gold standard.
Management
Supportive Care:
- Thermoregulation (maintain neutral thermal environment)
- IV access; correct hypoglycemia, electrolyte imbalances
- Oxygen supplementation, CPAP or ventilation if needed
- IV fluids for shock; inotropes (dopamine, dobutamine) if hypotension persists
- Correct coagulopathy (FFP, platelets) if DIC
- Phototherapy for jaundice
Antibiotic Therapy:
Empiric regimen (EOS - Ghai):
- Ampicillin + Gentamicin (first-line for community-acquired / EOS)
- Ampicillin: 50 mg/kg/dose IV q12h (q8h for meningitis)
- Gentamicin: 5 mg/kg/dose IV once daily
If meningitis suspected:
- Replace gentamicin with Cefotaxime (50 mg/kg/dose q8-12h) for better CNS penetration
- Avoid ceftriaxone in neonates - displaces bilirubin from albumin → kernicterus risk
If MRSA or nosocomial (LOS):
- Vancomycin ± Amikacin or Piperacillin-tazobactam
If HSV suspected:
- Add IV Acyclovir (20 mg/kg/dose q8h)
Duration:
- Uncomplicated bacteremia: 10-14 days
- Meningitis (GBS): 14-21 days; gram-negative meningitis: 21 days
- Negative cultures + good response: 5-7 days (or stop)
Early-Onset GBS Sepsis - Risk Assessment (AAP/Red Book)
Three approaches for infants ≥35 weeks:
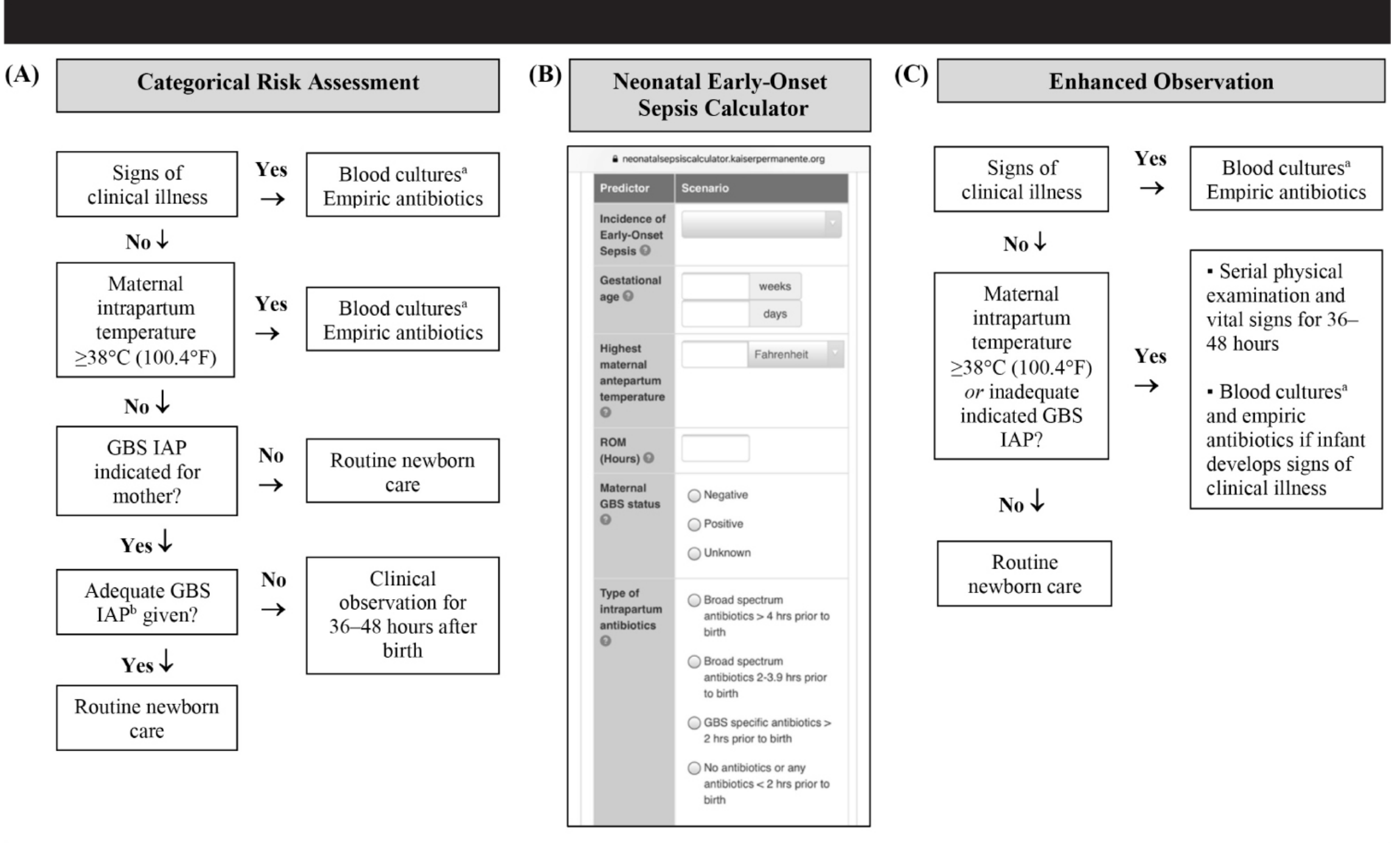
(A) Categorical approach - uses threshold risk factors
(B) Neonatal EOS Calculator (Kaiser Permanente) - multivariate, validated
(C) Enhanced clinical observation - serial exams for 36-48 hours
(B) Neonatal EOS Calculator (Kaiser Permanente) - multivariate, validated
(C) Enhanced clinical observation - serial exams for 36-48 hours
- Red Book 2021, p. 1101
Complications
- Meningitis → hydrocephalus, neurodevelopmental delay, hearing loss
- Septic shock → multi-organ dysfunction
- DIC → hemorrhage
- Periventricular leukomalacia (in preterm)
- Necrotizing enterocolitis (NEC)
- Subdural empyema, brain abscess
- Death (mortality 10-50% in developing countries; higher with gram-negative sepsis)
Prevention
- Antenatal: screen and treat maternal infections, GBS prophylaxis (IAP - Intrapartum Antibiotic Prophylaxis with Penicillin G)
- Clean delivery practices (especially at home deliveries)
- Hand hygiene in NICUs
- Strict aseptic technique for all invasive procedures
- Exclusive breastfeeding (provides IgA, lactoferrin, lysozyme)
- Rooming-in to reduce nosocomial exposure
- Umbilical cord care (clean, dry cord care; topical chlorhexidine in LMICs)
Key Points for Exams (Ghai Perspective)
| Point | Detail |
|---|---|
| Most common organism in India | Klebsiella pneumoniae |
| Gold standard diagnosis | Blood culture |
| Best single early indicator | I:T ratio >0.2 |
| Empiric treatment (EOS) | Ampicillin + Gentamicin |
| Avoid in neonates | Ceftriaxone (kernicterus risk) |
| Meningitis drug of choice | Cefotaxime |
| Most common sign | Non-specific - "not doing well" |
| Most alarming sign | Apnea (especially in preterm) |
| Hypothermia significance | Worse prognosis than fever |
| Breastfeeding role | Protective - reduces sepsis risk |
Sources: Ghai's Essential Pediatrics (knowledge-based), Tintinalli's Emergency Medicine, 9e, Red Book 2021 - AAP, Robbins Pathologic Basis of Disease, 10e
This is a shared conversation. Sign in to Orris to start your own chat.