How to read ecg
how to read ECG electrocardiogram interpretation systematic approach
ECG electrocardiogram waveform components PQRST intervals
How to Read an ECG
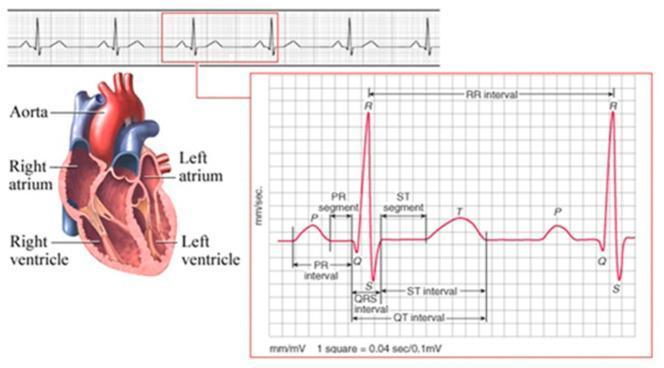
The ECG Waveform
| Wave/Segment | What it represents |
|---|---|
| P wave | Atrial depolarization |
| PR interval | Conduction from atria → ventricles (AV node) |
| QRS complex | Ventricular depolarization |
| ST segment | Early ventricular repolarization |
| T wave | Ventricular repolarization |
| QT interval | Total ventricular electrical activity |
| U wave | Repolarization of Purkinje fibers (sometimes visible) |
The 14-Step Systematic Approach (Harrison's, p. 6812)
Step 1 — Calibration & Technical Quality
- Standard calibration: 1 mV = 10 mm (2 large squares tall)
- Paper speed: 25 mm/s (each small square = 0.04 s; each large square = 0.2 s)
- Check for artifact, poor lead contact, and correct lead placement
Step 2 — Rhythm
- Is it regular or irregular?
- Is there a P wave before every QRS? A QRS after every P?
- Sinus rhythm: P waves upright in leads I, II, aVF
Step 3 — Heart Rate
- Regular rhythm: 300 ÷ number of large squares between R-R intervals
- 1 box = 300 bpm, 2 = 150, 3 = 100, 4 = 75, 5 = 60, 6 = 50
- Irregular rhythm: Count QRS complexes in a 10-second strip × 6
Step 4 — PR Interval (AV Conduction)
- Normal: 0.12–0.20 s (3–5 small squares)
- Short PR: pre-excitation (WPW), accelerated AV conduction
- Long PR: 1st-degree AV block
- Progressively lengthening → dropped beat: Mobitz I (Wenckebach)
- Fixed PR with dropped beats: Mobitz II
Step 5 — QRS Duration
- Normal: < 0.12 s (< 3 small squares)
- Widened QRS (≥ 0.12 s): bundle branch block, ventricular rhythm, hyperkalemia, drug toxicity
Step 6 — QT/QTc Interval
- Normal QTc: < 440 ms (men), < 460 ms (women)
- Correct for rate using Bazett's formula: QTc = QT ÷ √RR
- Prolonged QTc: risk of Torsades de Pointes (electrolyte abnormalities, drugs, congenital syndromes)
Step 7 — Mean QRS Axis
- Normal axis: −30° to +90°
- Quick method: if QRS is upright in leads I and aVF → normal axis
- Left axis deviation (< −30°): LBBB, inferior MI, left anterior fascicular block
- Right axis deviation (> +90°): RVH, RBBB, left posterior fascicular block, PE
Step 8 — P Waves
- Normal: upright in I, II; inverted in aVR; duration < 0.12 s; amplitude < 2.5 mm
- Peaked P in II (P pulmonale): right atrial enlargement
- Bifid P in II / biphasic P in V1 (P mitrale): left atrial enlargement
- Absent P waves: atrial fibrillation, sinoatrial block
Step 9 — QRS Voltages
- Low voltage (< 5 mm in all limb leads): pericardial effusion, emphysema, obesity, hypothyroidism
- Left ventricular hypertrophy (LVH): S in V1 + R in V5/V6 > 35 mm (Sokolow-Lyon)
- Right ventricular hypertrophy (RVH): dominant R in V1
Step 10 — Precordial R-Wave Progression
- R wave should grow from V1 → V5/V6
- Poor R-wave progression (dominant S beyond V3): anterior MI, LBBB, RVH
Step 11 — Abnormal Q Waves
- Pathologic Q wave: > 0.04 s wide OR > 25% of the R wave height in that lead
- Indicate prior MI (age and territory depend on which leads are affected)
| Leads with Q waves | Territory |
|---|---|
| II, III, aVF | Inferior (RCA) |
| V1–V4 | Anterior (LAD) |
| I, aVL, V5–V6 | Lateral (LCx) |
Step 12 — ST Segments
- Normal: isoelectric (flat, at baseline)
- ST elevation: STEMI, pericarditis (saddle-shaped, diffuse), Brugada, early repolarization
- ST depression: NSTEMI/UA, posterior MI (V1–V2), digitalis effect, strain pattern
Step 13 — T Waves
- Normal: upright in I, II, V3–V6; inverted in aVR
- T-wave inversions: ischemia, RVH/LVH strain, RBBB/LBBB, CNS events
- Peaked T waves: hyperkalemia, early ischemia ("hyperacute T waves")
Step 14 — U Waves
- Small positive deflection after T wave (best seen in V2–V3)
- Prominent U waves: hypokalemia, bradycardia, antiarrhythmics
- Inverted U waves: may indicate ischemia or LVH
Quick Reference: Common ECG Patterns
| Condition | Key finding |
|---|---|
| STEMI | ST elevation ≥ 1 mm in ≥ 2 contiguous leads |
| NSTEMI/UA | ST depression or T-wave inversions |
| LBBB | Wide QRS, notched R in V5/V6, QS in V1 |
| RBBB | Wide QRS, RSR' ("rabbit ears") in V1, wide S in V6 |
| AFib | Irregularly irregular rhythm, no P waves |
| VT | Wide-complex tachycardia, AV dissociation |
| Hyperkalemia | Peaked T → wide QRS → sine wave pattern |
| Hypokalemia | Flat T, prominent U waves |
| Long QT | QTc > 440 ms (men) / 460 ms (women) |
Key principle (Harrison's, p. 6812): Always compare with prior ECGs — subtle changes are often more significant than absolute values. Errors in ECG interpretation most commonly result from skipping steps.
18yr old female with severe iron deficiency anemia with usg whole abdomen showing spleenomegaly with prominent portal vein. Menstrual history is normal at present with past history of delayed menstrual cycle 5 months back for 4 months. Upeer gi endoscopy is normal. Rest of the routine investigations are normal
splenomegaly prominent portal vein iron deficiency anemia young patient portal hypertension
non-cirrhotic portal hypertension extrahepatic portal vein obstruction causes diagnosis young
splenomegaly portal hypertension ultrasound prominent portal vein
non-cirrhotic portal fibrosis idiopathic portal hypertension splenomegaly hypersplenism workup
iron deficiency anemia splenomegaly hypersplenism menstrual irregularity differential diagnosis
Clinical Assessment
Synthesizing the Clinical Picture
- Splenomegaly
- Prominent/dilated portal vein (USG)
- Iron deficiency anemia (likely from hypersplenism + sequestration)
- Normal upper GI endoscopy (no varices / no oesophageal varices bleed yet)
- Normal liver function tests
- Normal menstrual history currently (prior 4-month amenorrhea likely from anemia-related hypothalamic suppression)
Bailey & Love's (p. 1243): "Non-cirrhotic portal fibrosis, common in tropical countries, is associated with massive splenomegaly and pancytopenia without stigmata of liver dysfunction."
Differential Diagnosis
| Diagnosis | For | Against |
|---|---|---|
| EHPVO | Young age, splenomegaly, prominent portal vein, preserved liver function, normal endoscopy (pre-variceal stage) | Need Doppler to confirm PV thrombosis/cavernoma |
| NCPF / Idiopathic Portal Hypertension | Young female, tropical setting, massive splenomegaly, normal LFTs, hypersplenism | Diagnosis of exclusion |
| Cirrhotic portal HTN | Portal vein dilation, splenomegaly | Normal LFTs, no stigmata of CLD, normal endoscopy |
| Hemolytic anemia with congestive splenomegaly | Anemia + splenomegaly | Iron deficiency pattern (not hemolytic); reticulocyte/hemolysis work up needed |
| Thalassemia trait | Iron deficiency-like picture + splenomegaly | Would show microcytic hypochromic with raised HbA2; iron indices differ |
| Sinistral (left-sided) portal HTN | Splenomegaly + normal liver | Isolated splenic vein thrombosis; pancreatitis history needed |
| Lymphoma / Infiltrative disease | Splenomegaly | No lymphadenopathy mentioned; systemic features absent |
| Connective tissue disease (SLE, etc.) | Young female | No other features mentioned |
Most Likely Diagnosis: EHPVO or NCPF
"The clinical hallmarks of EHPVO are hemorrhage from gastric/esophageal varices and hypersplenism with splenic enlargement, thrombocytopenia, and less commonly ascites. Liver function is always preserved unless EHPVO occurs with a coexistent primary liver disorder."
USG Doppler Findings (What to Look For)
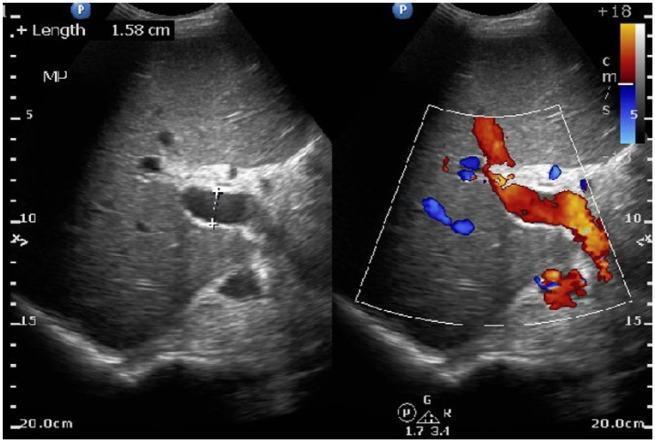
- Portal vein diameter (>13 mm = dilated — here already noted as prominent)
- Flow direction (hepatopetal vs. hepatofugal)
- Evidence of cavernous transformation of portal vein (EHPVO)
- Splenic vein diameter
- Hepatic echotexture (to rule out cirrhosis/fibrosis)
- Hepatic veins (to rule out Budd-Chiari)
Investigations Required
| Investigation | Purpose |
|---|---|
| USG Doppler of portal system | Confirm portal vein patency, flow direction, rule out cavernoma (EHPVO) |
| CBC with differential | Assess for pancytopenia (hypersplenism) — thrombocytopenia, leukopenia |
| Peripheral smear | Rule out hemolytic anemia, thalassemia, blast cells |
| Iron studies (serum iron, ferritin, TIBC) | Confirm iron deficiency, rule out anemia of chronic disease |
| HbA2 / Hb electrophoresis | Rule out thalassemia trait |
| Reticulocyte count | Assess bone marrow response; elevated in hemolysis |
| LFT, coagulation profile | Baseline liver function; PT/INR may be deranged in advanced disease |
| Thrombophilia screen | In EHPVO: Factor V Leiden, Protein C/S, antithrombin III, JAK2 mutation, antiphospholipid antibodies |
| ANA, anti-dsDNA | Rule out SLE (young female) |
| Urine routine | Rule out hematuria in SLE/vasculitis |
| Serology (HBsAg, anti-HCV) | Rule out viral hepatitis-related portal hypertension |
| Upper GI endoscopy with retroflexion | Already done — but repeat if Doppler suggests significant portal HTN to look for fundal varices |
| Liver biopsy (if needed) | Only if NCPF vs. early cirrhosis is uncertain |
Key Points About the Anemia
- Hypersplenism — splenic sequestration of RBCs → shortened RBC survival → compensatory increased iron utilization
- Menstrual loss — prior episodes of delayed/prolonged cycles may have contributed (though now normal)
Management Outline (After Confirmation)
- Iron supplementation — oral (ferrous sulfate) or IV iron if severe/malabsorption
- Doppler-guided diagnosis — definitive imaging before any intervention
- If EHPVO confirmed: Thrombophilia workup → anticoagulation if acute/subacute thrombosis → surgical evaluation (Meso-Rex bypass preferred; portosystemic shunt if bypass not feasible)
- If NCPF: Conservative + endoscopic surveillance; beta-blockers for portal HTN if varices develop
- Monitor CBC — particularly platelets (hypersplenism marker)
- GI surveillance endoscopy — at regular intervals even if currently normal, as varices can develop
Summary
This 18-year-old female most likely has Non-Cirrhotic Portal Hypertension (EHPVO or NCPF) presenting with hypersplenism-related iron deficiency anemia and splenomegaly with portal vein prominence, in the absence of liver disease or variceal bleeding. The prior 4-month amenorrhea is best explained by anemia-induced functional hypothalamic suppression. The next critical step is a Doppler ultrasound of the portal venous system and CBC with peripheral smear to characterize the anemia and confirm hypersplenism.