Why thiamene is given at alcoholic pt
Reading File
Finding Sources
Searching the Web
thiamine given alcoholic patients Wernicke encephalopathy mechanism deficiency
Reading File
Here is a complete explanation:
Why Thiamine (Vitamin B1) is Given to Alcoholic Patients
The Core Problem: Thiamine Deficiency
Chronic alcohol use causes thiamine deficiency through two mechanisms:
- Reduced dietary intake - alcoholics often eat poorly and are malnourished
- Reduced absorption - alcohol directly impairs thiamine absorption from the gut, and also reduces its activation in the liver
Main Reason: Prevention and Treatment of Wernicke's Encephalopathy
Wernicke's encephalopathy is an acute, life-threatening neurological emergency caused directly by thiamine deficiency. The classic triad includes:
- Ophthalmoplegia (eye movement disorder / nystagmus)
- Ataxia (unsteady gait)
- Confusion / altered mental status
However, the full triad is only present in a minority of patients, so the condition is frequently underdiagnosed. Any alcoholic patient undergoing detoxification who shows any one of these features should receive thiamine immediately.
If untreated, Wernicke's encephalopathy can progress to Korsakoff syndrome - an irreversible amnestic disorder with:
- Severe memory loss (anterograde > retrograde)
- Confabulation (making up stories to fill memory gaps)
- This combined condition is called Wernicke-Korsakoff syndrome
Critical Warning: Glucose Before Thiamine Can Be Deadly
Thiamine is required for glucose metabolism (it is an essential cofactor in pyruvate dehydrogenase and alpha-ketoglutarate dehydrogenase reactions in the Krebs cycle). If a thiamine-deficient patient is given IV glucose before thiamine, the glucose load depletes the already low thiamine stores further and can precipitate acute Wernicke's encephalopathy. This is why the rule is:
Always give thiamine BEFORE glucose in alcoholic or malnourished patients.
Who Gets Thiamine and How?
| Patient Type | Route | Dose |
|---|---|---|
| Low-risk drinkers, adequate diet | Oral | 300 mg/day during withdrawal |
| Harmful/dependent drinkers with malnutrition | Parenteral (IV/IM) | High-dose IV (e.g. Pabrinex) followed by oral maintenance |
| Suspected Wernicke's encephalopathy | IV immediately | High-dose until symptoms resolve |
Per NICE guidelines, prophylactic parenteral thiamine is recommended for all harmful or dependent drinkers who are malnourished or at risk of malnourishment.
Risk Factors for Wernicke's in Alcoholics
- Acute withdrawal
- Malnutrition / recent weight loss
- Decompensated liver disease
- Homelessness
- Peripheral neuropathy
- Previous history of Wernicke's encephalopathy
- Vomiting or diarrhoea
(Maudsley Prescribing Guidelines in Psychiatry, 15ed)
In short: Thiamine is given to alcoholics because chronic alcohol use causes thiamine deficiency, which leads to Wernicke's encephalopathy - a preventable but potentially fatal and irreversible brain condition. Since thiamine is safe, cheap, and the condition is commonly underdiagnosed, it is given prophylactically to essentially all patients with significant alcohol use disorder.
Myelin sheeth of neuron is made of ?
Finding Sources
Searching the Web
myelin sheath composition lipids proteins oligodendrocyte Schwann cell
Reading File
Reading File
Loading Image
Loading Image
Myelin Sheath - Complete Composition
What is the Myelin Sheath?
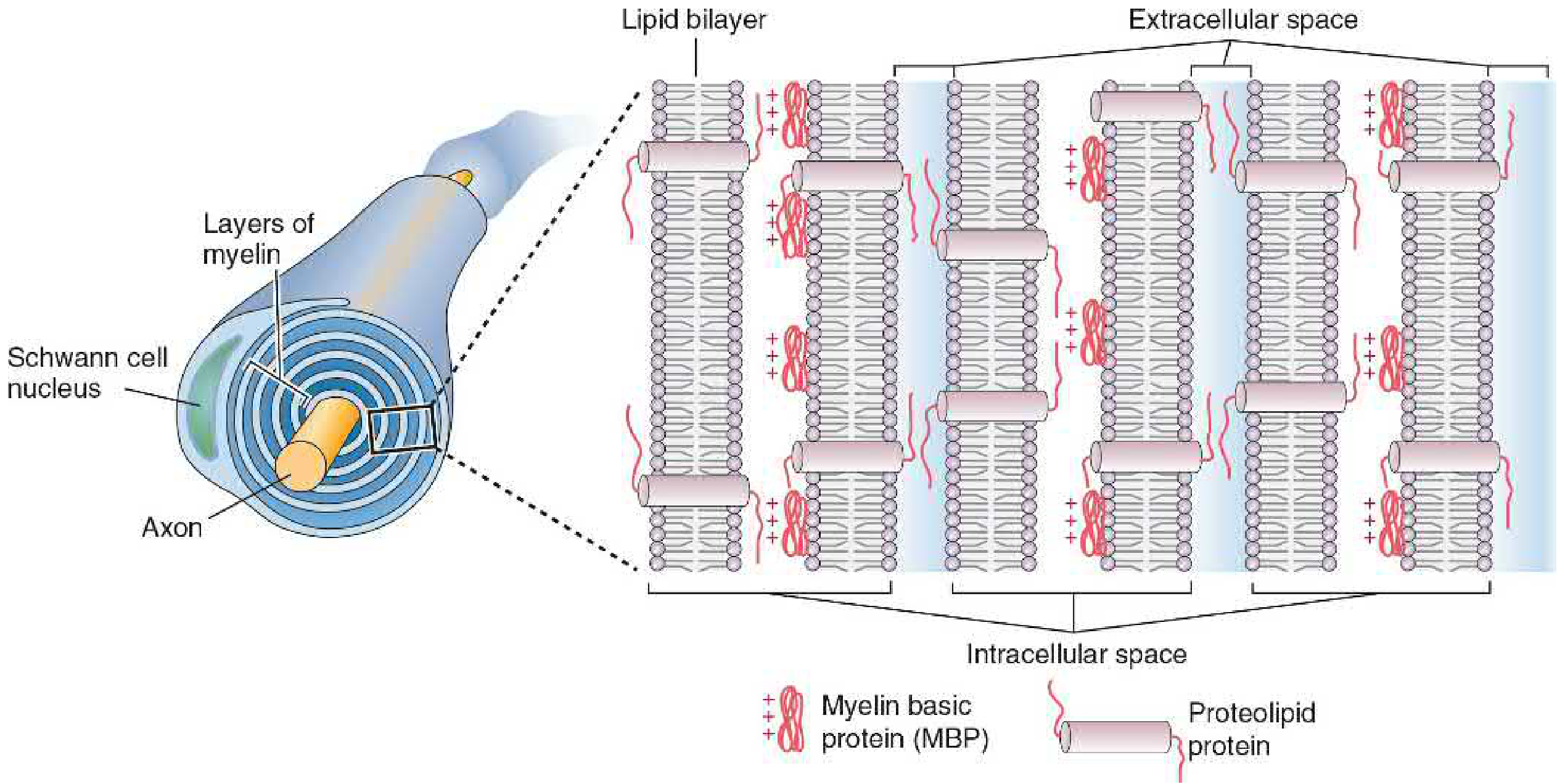
The myelin sheath is a lipid-protein covering that wraps around the axon of a neuron in multiple concentric layers. It is formed from the plasma membrane of supporting glial cells - specifically Schwann cells (PNS) and oligodendrocytes (CNS).
Composition of Myelin Sheath
| Component | % of Dry Weight | Notes |
|---|---|---|
| Total Lipid | ~70% | Much higher than regular cell membranes |
| Total Protein | ~30% | Much lower than regular cell membranes |
Lipid breakdown:
| Lipid | % of Myelin Lipid |
|---|---|
| Cholesterol | ~27.7% |
| Cerebroside (galactosylcerebroside) | ~22.7% - marker lipid of myelin |
| Ethanolamine phosphatides | ~15.6% |
| Phosphatidylcholine | ~11.2% |
| Sphingomyelin | ~7.9% |
| Sulfatide | ~3.8% |
Cerebrosides (especially galactosylcerebroside) are almost exclusively found in myelin - making them a biochemical marker for myelin.
(Basic Medical Biochemistry, 6e - Table 46.2)
Key Myelin Proteins
In the CNS (Oligodendrocytes):
- Proteolipid Protein (PLP) - most abundant; protrudes into extracellular space; aids compaction of membrane layers through hydrophobic interactions
- Myelin Basic Protein (MBP) - small, positively charged; stabilizes the structure from within the membrane (intracellular side)
In the PNS (Schwann cells):
- P0 protein - replaces PLP in the PNS; serves a similar compaction role
- MBP - present in both
How is it Formed?
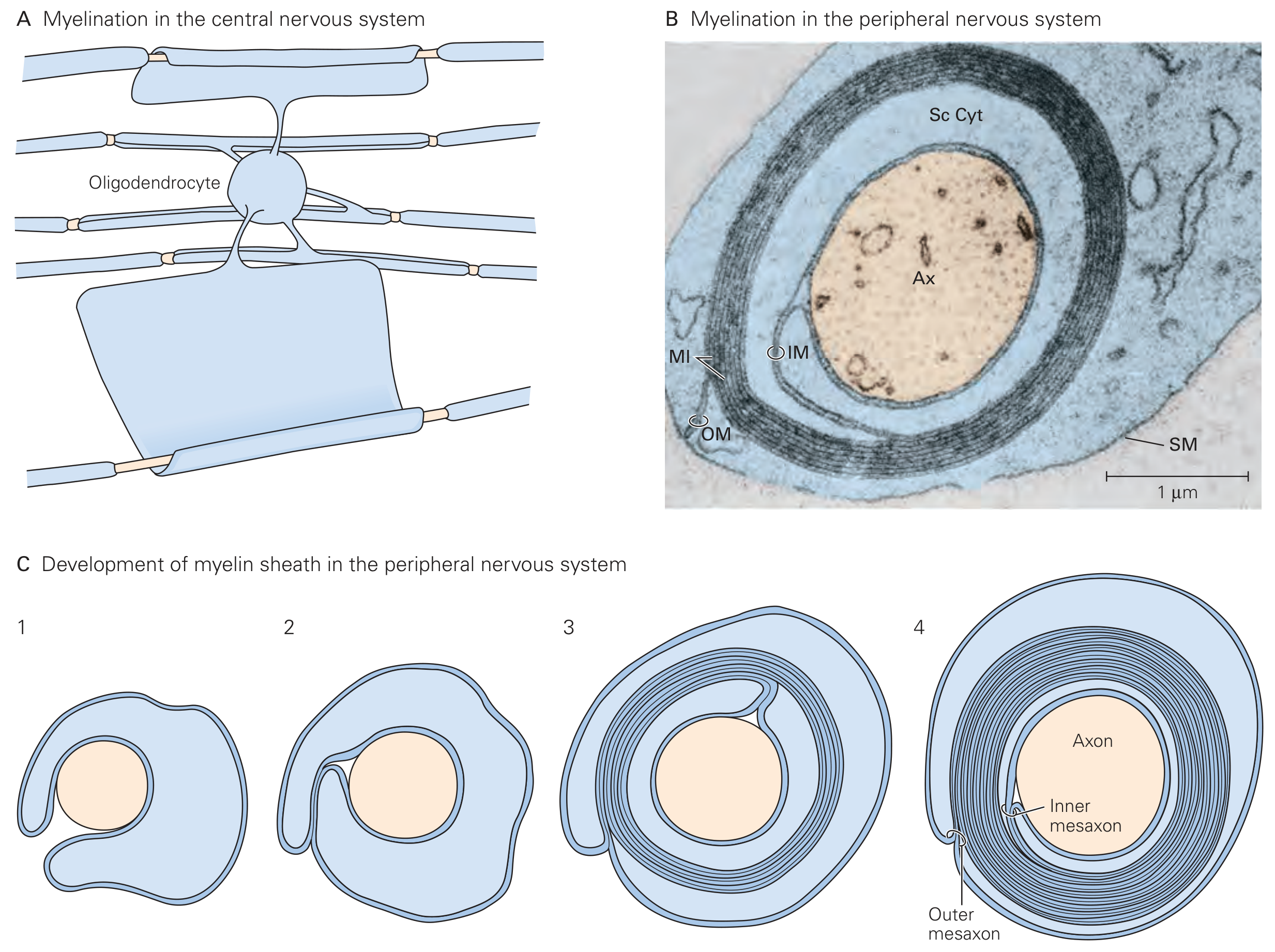
- PNS: A Schwann cell wraps itself around a single axon. Its external membrane spirals in concentric layers; cytoplasm is squeezed out, forming a compact lamellar structure.
- CNS: A single oligodendrocyte can myelinate multiple axons simultaneously by sending out sheet-like processes.
- The gaps between myelin segments are called Nodes of Ranvier, where the axon is exposed - this allows saltatory conduction (nerve impulse "jumps" from node to node), greatly increasing conduction speed.
(Eric Kandel - Principles of Neural Science, 6e)
Function of the Myelin Sheath
- Electrical insulation - prevents leakage of ionic currents
- Saltatory conduction - dramatically increases nerve impulse speed
- Metabolic support - provides trophic support to the axon
Clinical Relevance
Demyelinating diseases (destruction of myelin) include:
- Multiple Sclerosis (MS) - autoimmune destruction of CNS myelin (oligodendrocytes targeted)
- Guillain-Barre Syndrome - autoimmune attack on PNS myelin (Schwann cells targeted)
- Leukodystrophies - genetic disorders affecting myelin synthesis
Do methycibalamin helps to maintain myelin sheet
Finding Sources
Searching the Web
methylcobalamin myelin sheath maintenance mechanism vitamin B12 deficiency demyelination
Reading File
Finding Sources
Reading File
Yes - Methylcobalamin Maintains the Myelin Sheath
Methylcobalamin is the neurologically active form of Vitamin B12 and is directly required for myelin maintenance. Here is a complete breakdown:
What is Methylcobalamin?
Vitamin B12 (cobalamin) exists in two active coenzyme forms in the body:
- Methylcobalamin - active in the cytoplasm, required for nerve function
- Adenosylcobalamin - active in mitochondria, required for energy metabolism
Methylcobalamin is the form that directly protects and maintains the myelin sheath.
Two Key Biochemical Mechanisms
1. Methionine Synthesis (Primary mechanism for myelin)
Methylcobalamin is an essential cofactor for the enzyme methionine synthase, which converts:
Homocysteine + Methyl group → Methionine
Methionine is then converted to S-adenosylmethionine (SAM), the universal methyl donor in the body. SAM is required for:
- Methylation of myelin basic protein (MBP)
- Phospholipid synthesis (phosphatidylcholine) needed for the lipid bilayer of myelin
- Gene expression needed for oligodendrocyte and Schwann cell function
When methylcobalamin is deficient, methionine and SAM levels fall, and myelin cannot be properly synthesized or maintained.
(Adams and Victor's Principles of Neurology, 12e)
2. Methylmalonyl-CoA Pathway (Secondary mechanism)
Adenosylcobalamin (another B12 form) is needed for the reaction:
Methylmalonyl-CoA → Succinyl-CoA (via methylmalonyl-CoA mutase)
In B12 deficiency, this reaction is blocked, causing accumulation of propionyl-CoA, which then gets abnormally incorporated into myelin lipids as odd-chain fatty acids in place of normal even-chain fatty acids. This structurally disrupts the myelin sheath.
(Adams and Victor's Principles of Neurology, 12e)
What Happens When Methylcobalamin is Deficient?
Subacute Combined Degeneration (SCD) of the spinal cord - the classic neurological consequence of B12 deficiency:
- Myelin swells and vacuolates, then axons degenerate
- Affects posterior columns (vibration, position sense) and lateral corticospinal tracts
- Presents with:
- Bilateral numbness and tingling (hands and feet)
- Loss of vibration and proprioception
- Ataxia (unsteady gait, positive Romberg sign)
- Spastic weakness, hyperreflexia, Babinski sign
- If untreated: paraplegia
(Robbins & Kumar Pathologic Basis of Disease; Goldman-Cecil Medicine)
Methylcobalamin vs Other B12 Forms
| Feature | Methylcobalamin | Cyanocobalamin |
|---|---|---|
| Form | Active, ready-to-use | Must be converted in body |
| Primary role | Nerve/myelin protection | General B12 functions |
| Route | Oral / IM | Oral / IM |
| Best for | Neuropathy, nerve repair | General supplementation |
Clinical Summary
| Situation | Role of Methylcobalamin |
|---|---|
| Normal | Maintains myelin via SAM-mediated methylation |
| Deficiency | Demyelination → Subacute Combined Degeneration |
| Supplementation | Halts progression; may partially reverse early demyelination |
| Advanced deficiency (paraplegia) | Recovery is poor even with treatment |
Bottom line: Methylcobalamin is essential for myelin maintenance through two pathways - methionine/SAM-mediated methylation reactions, and proper fatty acid incorporation into myelin lipids. Its deficiency causes a well-recognized demyelinating disease of the spinal cord. This is why methylcobalamin is commonly prescribed in neuropathy, diabetic nerve damage, and B12 deficiency states.
This is a shared conversation. Sign in to Orris to start your own chat.