Bartons fracture etiology mechanism of injury associated injury signs and symptoms and investigations and evaluation treatment explain in detail with appropriate illustrative diagrams and images
Barton's fracture etiology mechanism injury signs symptoms treatment orthopedics
https://www.ncbi.nlm.nih.gov/books/NBK499906
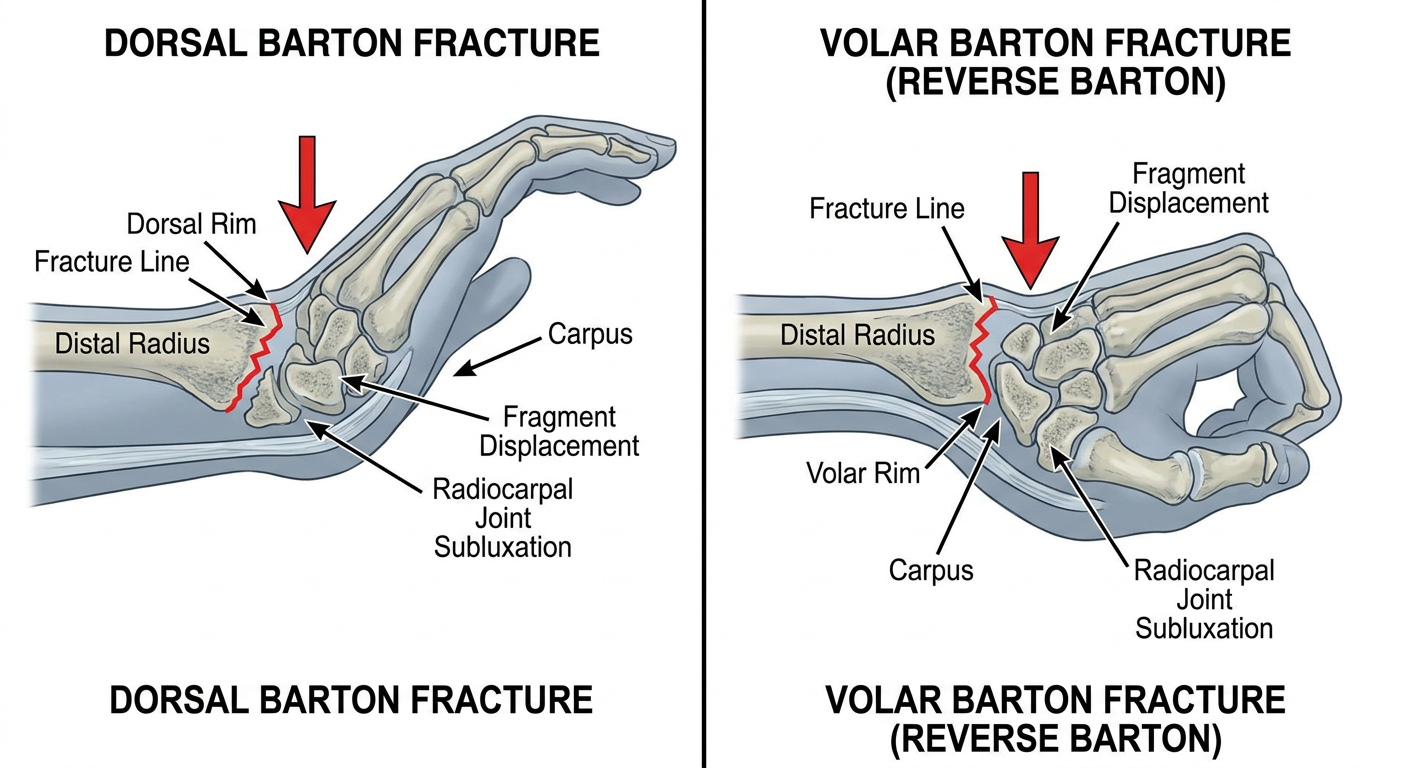
Medical diagram showing Barton's fracture of the distal radius wrist. Split panel illustration: Left panel shows dorsal Barton fracture with the dorsal rim of the distal radius sheared off and the carpus displaced dorsally, mechanism arrow showing fall on dorsiflexed pronated wrist. Right panel shows volar Barton fracture (reverse Barton) with volar rim fracture and carpus displaced volarly, mechanism arrow showing fall on flexed wrist. Labels include: distal radius, carpus, fracture line, fragment displacement direction, radiocarpal joint subluxation. Clean anatomical cross-section lateral view style with clear labels, medical textbook illustration style.
Medical diagram comparing Barton fracture vs Colles fracture vs Smith fracture of the wrist distal radius. Three side-by-side lateral view illustrations labeled clearly. Barton fracture shows intra-articular rim fracture with carpal subluxation. Colles shows extra-articular dorsal displacement dinner fork deformity. Smith shows extra-articular volar displacement garden spade deformity. Each with labeled arrows indicating fracture location and displacement direction. Clean anatomical medical education illustration style with color coding per fracture type.
Barton's Fracture - Complete Clinical Guide
1. Definition and Historical Background
2. Types of Barton's Fracture
| Feature | Dorsal Barton (Classic) | Volar Barton (Reverse Barton) |
|---|---|---|
| Fracture site | Dorsal/posterior rim of distal radius | Volar/anterior rim of distal radius |
| Carpal displacement | Dorsal | Volar (palmar) |
| Mechanism | Dorsiflexion + pronation | Volar flexion / fall on flexed wrist in supination |
| Frequency | Less common | More common |
3. Comparison with Other Distal Radius Fractures
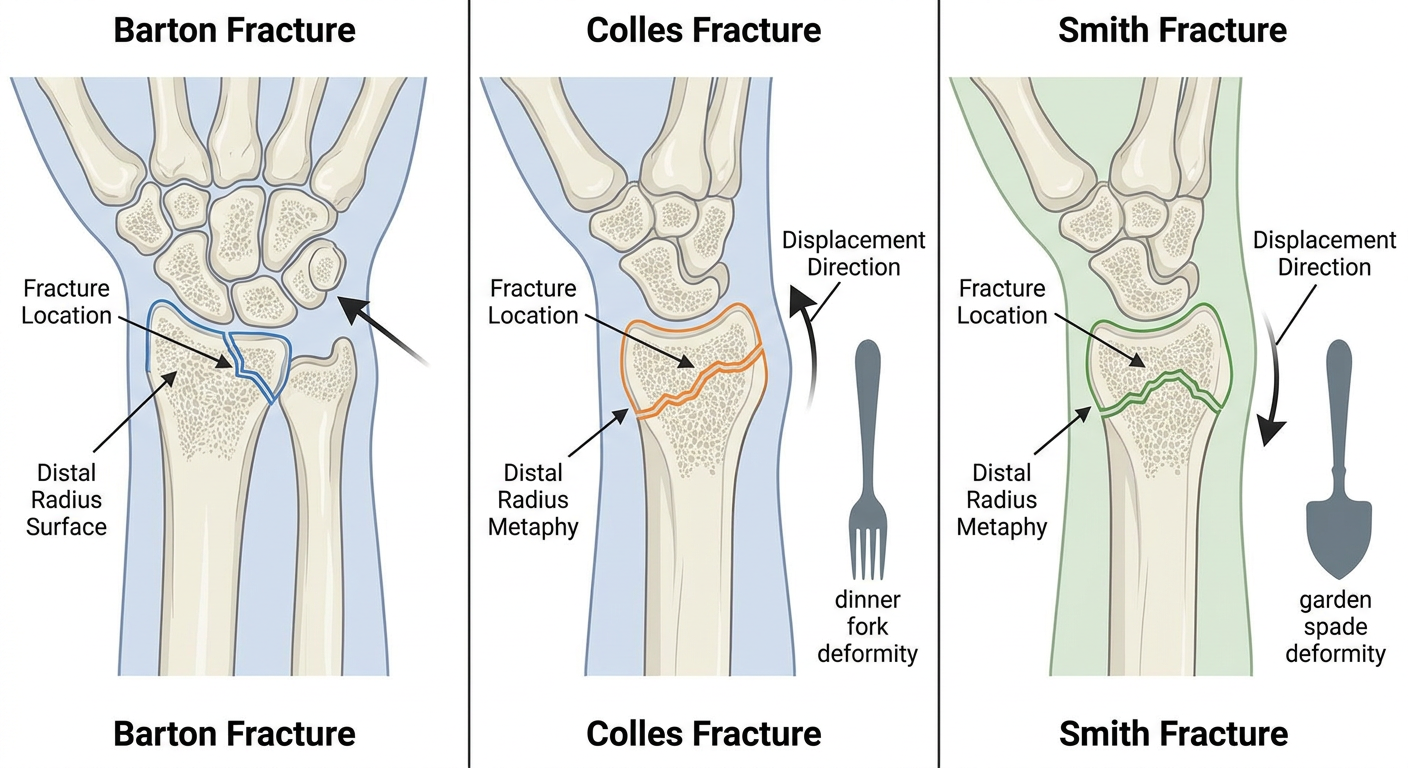
- Barton: Intra-articular, rim fracture, radiocarpal subluxation - no classic deformity name
- Colles: Extra-articular, dorsally angulated - "dinner fork deformity"
- Smith (reverse Colles): Extra-articular, volarly angulated - "garden spade deformity"
4. Etiology
Patient Population
- Young adults / males: sporting injuries, motorcycle accidents, high-energy trauma - young male workers/motorcycle riders account for approximately 70% of Barton fracture cases
- Elderly / women: low-energy falls from standing height; osteoporosis reduces the force threshold required
- High-energy mechanisms: motor vehicle accidents, falls from height, direct trauma
Pathomechanics
- Extrinsic radiocarpal ligaments
- Joint capsule
- Scaphoid and lunate fossae of the radius
5. Mechanism of Injury
Dorsal Barton Fracture (Classic)
- Fall on an outstretched, pronated wrist in dorsiflexion
- Axial compressive force transmitted through the carpus strikes the dorsal rim of the articular surface
- The dorsal rim is sheared off; the carpus subluxates dorsally
Volar Barton Fracture (Reverse Barton) - more common
- Fall on a flexed wrist (volar flexion) or fall on outstretched hand in supination
- Compressive shear force directed at the volar rim of the articular surface
- The volar rim fractures; the carpus subluxates volarly/palmarly
- Described in Tintinalli's EM: "less common volar rim fracture is produced by a fall on the outstretched hand in supination"
Force Transmission Pathway
Impact (ground) → Metacarpals → Carpus → Radiocarpal articular surface →
Shearing at the rim → Triangular rim fragment separates → Carpus displaced with fragment
6. Associated Injuries
| Associated Injury | Notes |
|---|---|
| TFCC tear (Triangular Fibrocartilage Complex) | Most common associated soft tissue injury |
| Distal Radioulnar Joint (DRUJ) disruption | Risk increased with coronal shift, >6 mm prereduction ulnar variance |
| Scapholunate ligament injury | Creates radiocarpal instability; may not be apparent acutely |
| Volar Intercalated Segment Instability (VISI) | Can result from ligamentous disruption |
| Ulnar styloid fracture | Common concomitant fracture |
| Median nerve compression | Acute carpal tunnel syndrome |
| Compartment syndrome | Forearm; must be excluded at initial presentation |
| Scaphoid fracture | Check with dedicated imaging if clinically suspected |
7. Signs and Symptoms
History
- Acute onset wrist pain following trauma
- Description of mechanism: fall on outstretched hand, sports injury, MVA
- Young patients: high-energy mechanism; elderly patients: low-energy fall
Physical Examination
- Wrist swelling and edema
- Deformity of the wrist (less pronounced than Colles fracture but visible)
- Ecchymosis (bruising) - may be delayed 24-48 hours
- Skin integrity assessment (open fracture?)
- Dorsal or volar wrist tenderness directly over the distal radius rim
- Point tenderness at the radiocarpal joint
- Bony crepitus may be palpable
- Median nerve: check sensation in the thumb, index, middle, and radial half of ring finger; thenar muscle strength
- Radial nerve: dorsal web space sensation
- Radial artery: capillary refill, radial pulse
- Restricted range of motion of the wrist (flexion, extension, pronation, supination)
- Grip strength reduced
8. Investigations and Evaluation
Imaging
Plain Radiographs (First-Line)
- May show a comminuted fracture of the distal radial metaphysis
- Fracture line at the articular margin
- Radial styloid fracture may coexist
- Carpal shift visible
- Shows the oblique intra-articular fracture of the volar or dorsal rim of the radius
- Demonstrates the degree of articular surface involvement
- Confirms the direction and magnitude of carpal subluxation/dislocation
- Radial height: 11 mm
- Radial inclination: 22 degrees
- Volar tilt: 11 degrees
- Radial shortening < 3 mm
- Dorsal tilt < 10 degrees
- Intra-articular step-off < 2 mm



CT Scan
- Indicated when X-rays are inconclusive or show complex comminution
- Best for assessing articular step-off, fragment size, and surgical planning
- Evaluates intra-articular involvement in 3D
- Useful to identify die-punch fragments or occult associated carpal fractures
MRI
- Reserved for assessment of soft tissue injuries
- Evaluates TFCC integrity
- Identifies scapholunate ligament tears
- Useful when carpal instability is suspected clinically but not confirmed radiographically
- Not a first-line investigation in the acute setting
Other Studies
- DRUJ assessment under fluoroscopy: pronation-supination stress test if DRUJ injury suspected
- EMG/nerve conduction: if median nerve injury is present and persistent (not acute)
- Bone density (DEXA): in elderly patients as part of osteoporosis workup (fragility fracture)
- Doppler ultrasound: rarely needed; if vascular injury suspected
9. Treatment
A. Emergency Department Management (Immediate)
- Analgesia: NSAIDs (ibuprofen), acetaminophen/paracetamol; IV/IM analgesia if severe
- Neurovascular documentation: before and after any manipulation
- Splinting: Sugar-tong splint or volar slab for temporary immobilization
- Emergent orthopedic consultation: required for all Barton fractures (unstable by nature)
B. Conservative (Non-Operative) Treatment
- Minimally displaced fractures
- Fragments involving < 50% of the radial articular surface
- No associated carpal subluxation
- Closed reduction under fluoroscopy (attempted under sedation/haematoma block)
- Sugar-tong splint immobilization
- Followed by cast application once swelling subsides
- Urgent orthopedic follow-up within 2-3 days
C. Operative Treatment
- Fracture involving > 50% of the radial articular surface
- Accompanying carpal subluxation
- Failed closed reduction
- Irreducible fracture
- Open fracture
- Associated neurovascular compromise
Open Reduction and Internal Fixation (ORIF) - Standard of Care
- Most Barton fractures require ORIF
- Volar Barton: volar plating approach (Henry approach to volar surface of distal radius)
- Dorsal Barton: dorsal plating (direct visualization of articular surface)
- Open reduction - direct visualization of articular surface
- Reduction and anatomic alignment of the rim fragment
- Internal fixation - typically a volar locking plate (for volar Barton) or dorsal buttress plate
- Intraoperative fluoroscopy to confirm reduction
- Address associated ligamentous injuries (TFCC, scapholunate) if needed
Percutaneous Pinning
- An option when closed reduction under fluoroscopy is successful but fracture is at risk of re-displacement
- K-wires used to hold reduction
- Less commonly used than plate fixation
External Fixation
- Used in highly comminuted fractures or when soft tissue condition precludes plating
- Can be used as a bridging procedure
D. Post-operative Rehabilitation
- Early range-of-motion exercises for wrist and fingers started as soon as possible to prevent stiffness
- Progressive strengthening at 6-8 weeks
- Full return to activity at 3-6 months depending on fracture type and fixation
10. Complications
| Complication | Timing | Notes |
|---|---|---|
| Post-traumatic arthritis (radiocarpal OA) | Late | Most common long-term complication; related to quality of articular reduction |
| Carpal instability | Delayed | From ligamentous injury; may not be apparent acutely |
| Median nerve dysfunction | Early or late | Most common nerve complication; acute CTS needs emergent release |
| TFCC tear | Early | May require arthroscopic repair if DRUJ unstable |
| Complex Regional Pain Syndrome (CRPS) | Late (weeks-months) | Vitamin C 500 mg/day x 50 days prescribed postoperatively to reduce risk |
| EPL tendon rupture | Late | After ORIF due to long screws, or attritional wear at Lister's tubercle |
| FPL rupture | Late | Most common flexor injury after volar plating (watershed line issue) |
| Compartment syndrome | Early | Must be excluded at initial presentation |
| Malunion / loss of reduction | Early | Particularly with conservative management |
| Infection / hardware failure | Post-op | Standard surgical risks |
11. Prognosis
- Outcomes are most favorable when anatomic reduction of the articular surface is achieved and maintained
- The overall goal is sufficient pain-free motion to allow return to usual activities while minimizing early-onset osteoarthritis
- Young patients with high-energy injuries have higher complication rates due to concomitant soft tissue disruption
- Elderly patients with osteoporotic bone may have poorer fixation quality
Quick Reference Summary
BARTON'S FRACTURE AT A GLANCE
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Definition: Intra-articular rim fracture of distal radius
+ radiocarpal fracture-dislocation
Types: Dorsal (classic) | Volar (reverse, more common)
Mechanism: Dorsal = fall on dorsiflexed pronated wrist
Volar = fall on flexed/supinated wrist
Key feature: Carpus displaced WITH the fragment
Investigation: X-ray (PA + lateral) → CT if complex
Lateral view is MOST diagnostic
Treatment: Emergent ortho consult
Minimally displaced → splint + urgent f/u
Displaced/unstable → ORIF (standard of care)
Complications: Post-traumatic arthritis, TFCC tear, CTS,
CRPS, carpal instability
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
- ROSEN's Emergency Medicine: Concepts and Clinical Practice (9th ed.)
- Tintinalli's Emergency Medicine: A Comprehensive Study (8th ed.)
- Rockwood and Green's Fractures in Adults (10th ed., 2025)
- Miller's Review of Orthopaedics (9th ed.)
- Campbell's Operative Orthopaedics (15th ed., 2026)
- StatPearls - Barton Fracture (NCBI Bookshelf)