Menstrual cycle mbbs physiology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
I now have comprehensive information from Ganong's, Guyton & Hall, Costanzo, and Berek & Novak's Gynecology. Let me compile the full answer.
The Menstrual Cycle - MBBS Physiology
Overview
The menstrual cycle is the periodic, cyclical preparation of the female reproductive system for fertilization and pregnancy. The average duration is 28 days (range: 21-35 days), counted from the first day of one menstrual bleed to the first day of the next. The cycle is orchestrated by the hypothalamo-pituitary-ovarian (HPO) axis and is divided into concurrent ovarian and uterine phases.
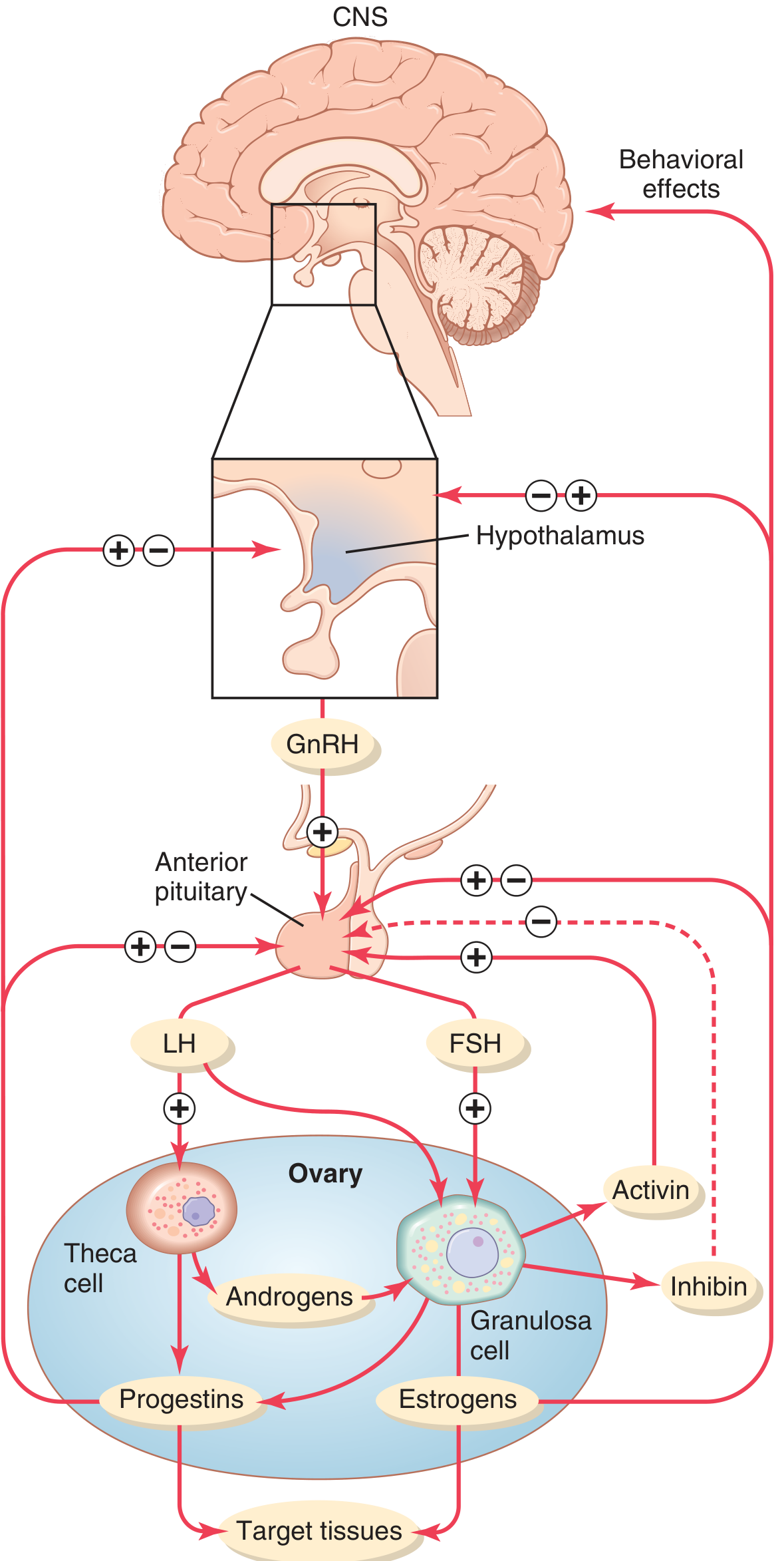
I. The HPO Axis - The Control System
The hypothalamus secretes GnRH (Gonadotropin-Releasing Hormone) in a pulsatile fashion (key - continuous GnRH suppresses the axis). GnRH stimulates the anterior pituitary to release FSH (follicle-stimulating hormone) and LH (luteinizing hormone), which act on the ovary.
KNDy neurons in the arcuate nucleus of the hypothalamus are the GnRH pulse generator. They co-express:
- Kisspeptin - stimulates GnRH neurons
- Neurokinin B - stimulates kisspeptin release
- Dynorphin - inhibits kisspeptin release (terminates each pulse)
II. The Two-Cell, Two-Gonadotropin Theory (High-Yield!)
This is the fundamental mechanism of estrogen synthesis in the follicle:
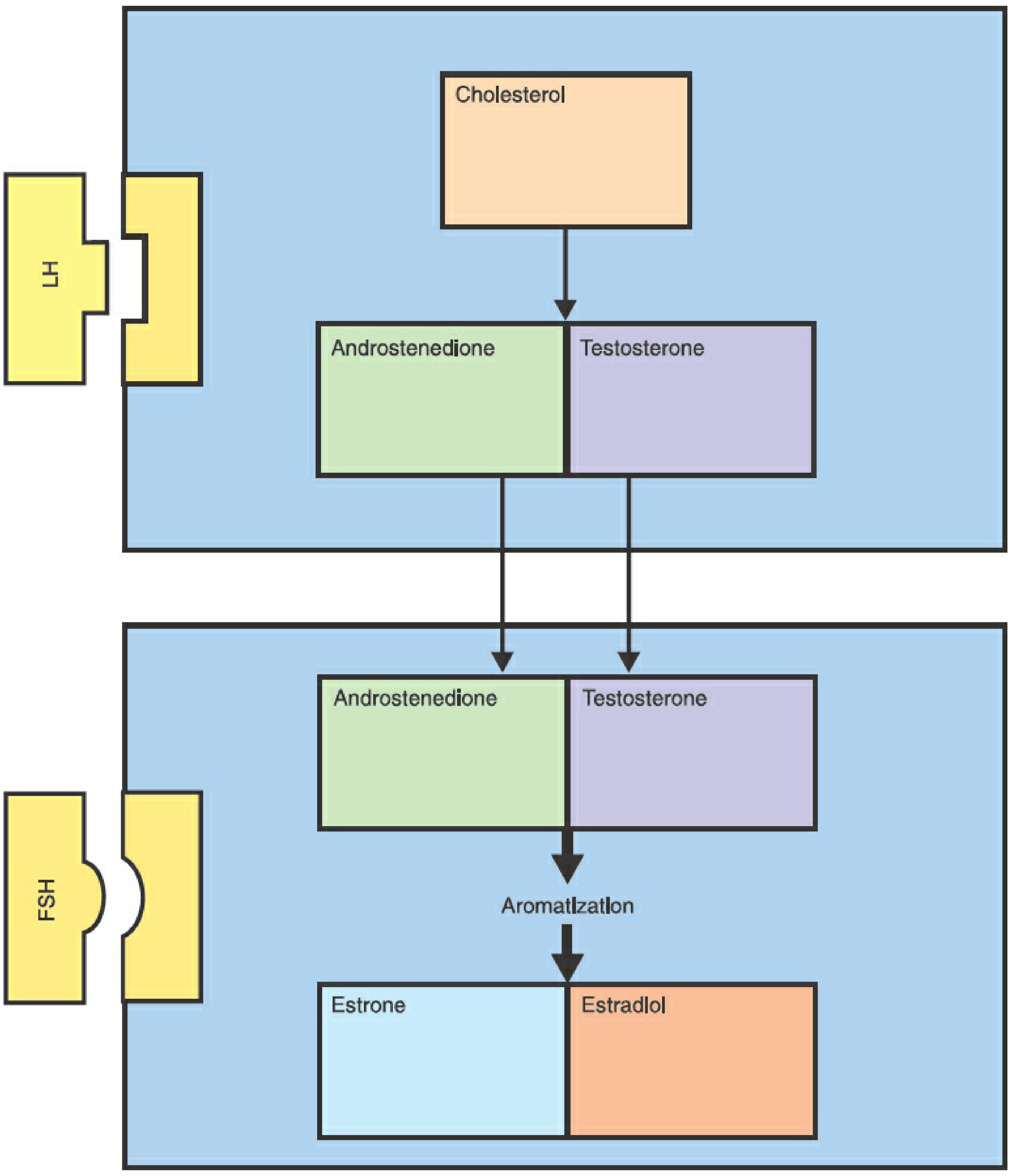
| Cell | Gonadotropin | Product |
|---|---|---|
| Theca interna cells | LH | Androgens (androstenedione, testosterone) from cholesterol |
| Granulosa cells | FSH | Aromatize androgens → Estrone and Estradiol |
- Theca cells lack aromatase; granulosa cells lack 17α-hydroxylase early on - hence the obligatory two-cell cooperation.
- Rising estrogen from granulosa cells negatively feeds back to reduce FSH, creating a selection pressure that only the dominant follicle (with the most FSH receptors) can survive. All others undergo atresia. - Berek & Novak's Gynecology, p. 289
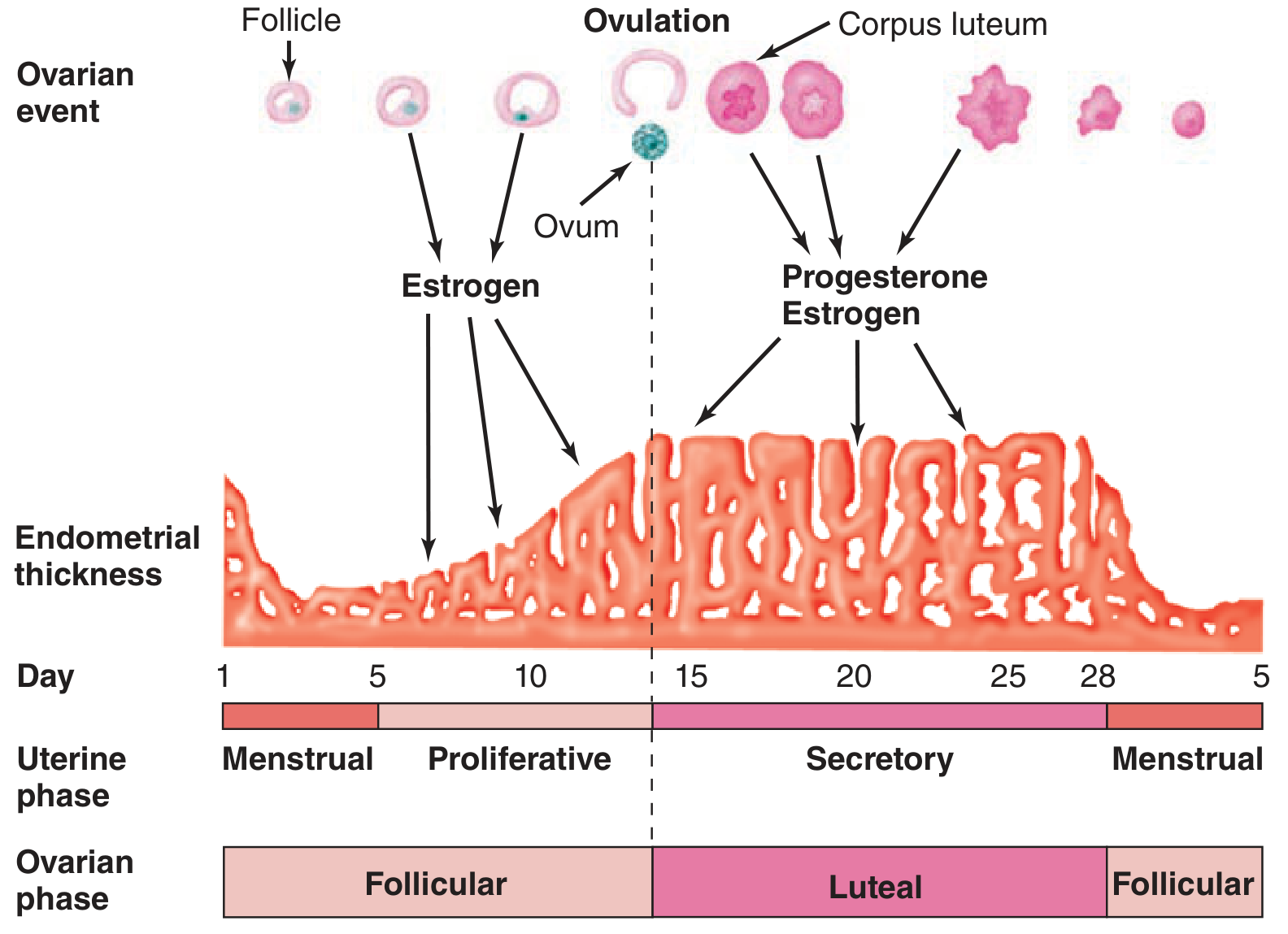
III. Ovarian Phases
Phase 1: Follicular Phase (Day 1-14)
- At birth, the ovaries contain ~2 million primordial follicles. By puberty, <300,000 remain. Only ~500 reach maturity in a lifetime.
- At the start of each cycle, FSH (rising because the previous corpus luteum has degenerated) stimulates a cohort of primordial follicles to develop.
- By day 6, one dominant (Graafian) follicle is selected based on its superior FSH receptor count and estrogenic microenvironment. Others undergo atresia via apoptosis.
- The Graafian follicle fills with follicular fluid (antrum formation). The primary oocyte is arrested in prophase I of meiosis and completes the 1st meiotic division just before ovulation, ejecting the first polar body.
- Granulosa cells secrete increasing amounts of estradiol (17β-estradiol), which:
- Proliferates the endometrium (stimulates gland and stromal growth, elongates spiral arteries)
- Makes cervical mucus thin, watery, elastic, alkaline ("spinnbarkeit" - can be stretched into a thread), and shows "ferning" pattern on a glass slide (channels form to allow sperm transit)
- Exerts negative feedback on FSH/LH (keeps levels modest through most of the follicular phase)
Ovulation (Day ~14)
When estradiol remains high for 2-3 days and exceeds a critical threshold, it switches its pituitary effect from negative to positive feedback, triggering the LH surge (LH rises 6-8 fold) and a smaller FSH surge. This is the preovulatory surge. It occurs 24-48 hours before ovulation.
- Progesterone secretion by granulosa cells just before ovulation also contributes to the FSH midcycle surge.
- The LH surge triggers:
- Completion of meiosis I in the oocyte → secondary oocyte (arrested in metaphase II)
- Rupture of the Graafian follicle → ovum released into peritoneal cavity, picked up by fimbriae
- Luteinization of the follicle remnant
- Brief lower abdominal pain from peritoneal irritation by follicular fluid = Mittelschmerz - Ganong's Review of Medical Physiology, p. 404-405
Phase 2: Luteal Phase (Day 14-28)
- The ruptured follicle fills with blood (corpus hemorrhagicum), then granulosa and theca cells proliferate under LH stimulation to form the corpus luteum (yellowish, lipid-rich luteal cells).
- VEGF is essential for corpus luteum vascularization.
- The corpus luteum secretes large amounts of progesterone + estrogen + inhibin.
- Duration is a remarkably constant 14 days.
- If no fertilization: Corpus luteum degenerates at ~day 24 → corpus albicans (scar tissue). Progesterone/estrogen fall → menstruation.
- If fertilization occurs: hCG (from trophoblast) rescues the corpus luteum, which persists through the first trimester.
IV. Uterine Phases
Phase 1: Menstrual Phase (Day 1-4/5)
- Corpus luteum regression → progesterone and estrogen withdrawal → endometrial ischemia (spasm of spiral arteries, mediated by PGF2α) → necrosis and shedding of the stratum functionale.
- The stratum basale (supplied by straight basilar arteries) is NOT shed and regenerates the endometrium.
- Normal menstrual flow: duration 3-5 days (range 1-8 days), volume 30 mL average (normal up to 80 mL).
- Menstrual blood is predominantly arterial (75% arterial, 25% venous).
- Contains fibrinolysin from endometrial tissue → prevents clotting (clots in menstrual blood indicate excessive flow).
- Contains prostaglandins → responsible for dysmenorrhea (uterine cramps). - Ganong's Review of Medical Physiology, p. 405-406
Phase 2: Proliferative (Follicular) Phase (Day 5-14)
- Driven by estrogen from the growing follicle.
- Endometrium increases rapidly in thickness (days 5-14).
- Glands elongate but do not secrete; stroma grows.
- Spiral arteries elongate.
Phase 3: Secretory (Luteal) Phase (Day 14-28)
- Driven by progesterone (+ estrogen) from the corpus luteum.
- Glands become tortuous and coiled, accumulate glycogen in vacuoles, and secrete mucus.
- Stroma becomes edematous.
- Spiral arteries become more coiled and elongated.
- Progesterone causes cervical mucus to become thick, viscous, cellular - no ferning, no spinnbarkeit (blocks sperm - fertilization window has passed).
- Progesterone has a mild thermogenic effect → basal body temperature rises ~0.5°C in the luteal phase. This is the basis of the "rhythm method" of contraception.
- The secretory phase is always 14 days regardless of cycle length. Variability in cycle length is due to variability in the proliferative phase. - Costanzo Physiology 7th Edition, p. 479
V. Hormonal Summary Table
| Hormone | Follicular Phase | Around Ovulation | Luteal Phase |
|---|---|---|---|
| FSH | Rises early, then falls | Midcycle surge (smaller) | Low |
| LH | Low-moderate | Large midcycle surge (6-8×) | Low |
| Estradiol (E2) | Gradually rises to peak | High (triggers LH surge) | Secondary smaller peak, then falls |
| Progesterone | Very low | Slight rise just before ovulation | High (dominant hormone) |
| Inhibin B | Rises with follicular development | - | - |
| Inhibin A | Low | - | High from corpus luteum |
VI. Feedback Mechanisms (High-Yield)
| Situation | Feedback | Effect |
|---|---|---|
| Low estrogen (early follicular) | Negative on pituitary/hypothalamus | Suppresses FSH/LH but allows gradual rise |
| High sustained estrogen (preovulatory) | Positive on pituitary | Triggers LH surge → ovulation |
| Progesterone + estrogen (luteal) | Negative | Suppresses FSH/LH (prevents new cycle) |
| Inhibin (from granulosa/corpus luteum) | Negative | Specifically suppresses FSH |
| Activin (from granulosa) | Positive | Stimulates FSH secretion |
VII. Clinically Important Derivatives
| Concept | Clinical Relevance |
|---|---|
| Anovulatory cycles | Common first 12-18 months post-menarche and pre-menopause; no corpus luteum → no progesterone; cycle may shorten |
| No progesterone effect | Endometrium stays proliferative → irregular, variable bleeding |
| LH surge detection | Basis of ovulation predictor kits (urine LH) |
| Progesterone thermogenic effect | Basis of basal body temperature (BBT) charting |
| Ferning of cervical mucus | Indicates estrogen dominance = near ovulation |
| PCOS | Androgen excess → chronic anovulation (suppresses FSH, no dominant follicle) |
| hCG cross-reacts with LH receptor | Rescues corpus luteum in early pregnancy |
| Constant 14-day luteal phase | Forensic date calculation in obstetrics (Naegele's rule) |
VIII. Normal Menstruation - Key Numbers
| Parameter | Normal Value |
|---|---|
| Cycle length | 21-35 days (average 28) |
| Duration of flow | 1-8 days (average 3-5 days) |
| Volume of blood loss | Up to 80 mL (average 30 mL) |
| Arterial vs venous | 75% arterial, 25% venous |
| Luteal phase length | Always ~14 days (constant) |
| Follicle count at puberty | <300,000 |
| Follicles that ovulate in lifetime | ~500 |
Sources: Ganong's Review of Medical Physiology 26th Ed, p. 403-406 | Guyton & Hall Textbook of Medical Physiology, p. 1025-1026 | Costanzo Physiology 7th Ed, p. 479 | Berek & Novak's Gynecology, p. 289-291
This is a shared conversation. Sign in to Orris to start your own chat.