Left anterior fascicular block note
Reading File
Finding Sources
Finding Sources
Searching the Web
left anterior fascicular block ECG criteria diagnosis clinical significance
Reading File
Reading File
Reading File
Searching Images
left anterior fascicular block ECG 12-lead axis deviation
Loading Image
Loading Image
I have comprehensive content from the textbooks and ECG images. Here is the complete clinical note on Left Anterior Fascicular Block (LAFB).
Left Anterior Fascicular Block (LAFB)
Anatomy & Mechanism
The left bundle branch divides into two fascicles:
- Anterior fascicle — thin, long; supplies the anterolateral LV wall; relatively vulnerable to ischemia
- Posterior fascicle — thick, short, dual blood supply; more resistant to isolated block
In LAFB, impulses reaching the left ventricle travel exclusively via the posterior fascicle, which inserts inferoseptally. Depolarization therefore proceeds from inferior → superior and right → left, causing marked left axis deviation without significant QRS prolongation. — Goldman-Cecil Medicine, p. 565
ECG Criteria
| Feature | Finding |
|---|---|
| Frontal axis | −45° to −90° (left axis deviation) |
| QRS duration | Normal or minimally prolonged (<120 ms) |
| Lead I / aVL | qR pattern (small q, tall R) |
| Leads II, III, aVF | rS pattern (small r, deep S) |
| Precordial leads | May show delayed R-wave progression (late transition) |
| R-wave peak time in aVL | Prolonged (≥45 ms) |
LAFB is the most common cause of marked left axis deviation in adults and does not substantially prolong the QRS. — Harrison's Principles of Internal Medicine 22E, p. 1391
Representative ECG (isolated LAFB):
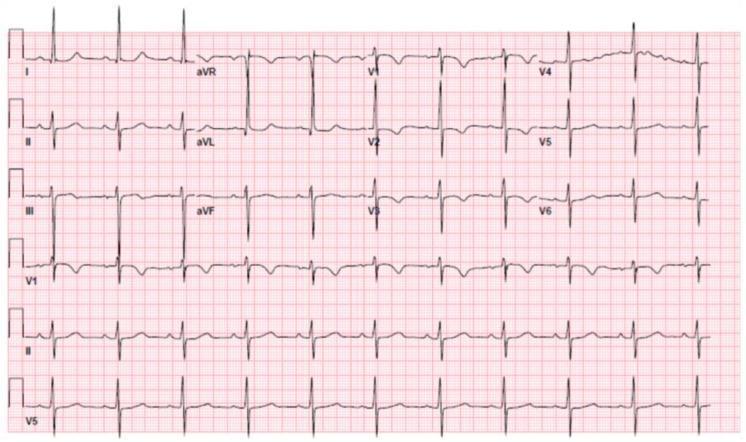
Key ECG Pattern: qR vs rS
- Leads I and aVL: Initial septal depolarization travels toward II/III/aVF (away from I/aVL) → small q wave; then the main LV vector swings up-and-left → tall R wave → qR
- Leads II, III, aVF: Initial vector moves toward them → small r; then main vector moves away → deep S → rS
Epidemiology
- Found in ~1% of otherwise healthy adults
- Prevalence of any bundle branch block rises from ~1% at age 50 to ~17% by age 80
- Most common isolated fascicular block — Goldman-Cecil Medicine, p. 565
Etiology / Associated Conditions
| Category | Examples |
|---|---|
| Degenerative | Fibrosis of the conduction system (Lev's/Lenègre's disease) |
| Ischemic | Coronary artery disease; LAD territory infarction |
| Structural | Hypertensive heart disease, aortic valve disease (including post-TAVR), cardiomyopathy |
| Infiltrative/Inflammatory | Sarcoidosis, Chagas disease, amyloidosis |
| Congenital | Congenital heart disease |
Clinical Significance
- Isolated LAFB: Generally benign in the absence of structural heart disease. No treatment required.
- Bifascicular block (LAFB + RBBB): The most common form of bifascicular block. Risk of progression to complete heart block is present but relatively low in asymptomatic patients.
- Trifascicular block (LAFB + RBBB + 1° AV block, or alternating BBB): Higher risk of complete AV block; pacemaker consideration warranted in symptomatic patients.
- New LAFB in acute MI: Particularly in the setting of anterior STEMI, suggests proximal LAD occlusion with septal involvement.
- VT morphology: RBBB/LAFB pattern (right precordial rSR' + LAD) is the signature of fascicular VT arising from the left posterior fascicle (Belhassen VT), which is responsive to verapamil. — Harrison's Principles of Internal Medicine 22E
Pacing Indications (LAFB context)
Retrospective studies suggest permanent pacing may reduce long-term risk of syncope in patients with bilateral bundle branch block (e.g., RBBB + LAFB). Isolated LAFB alone is not an indication for pacing. — Harrison's Principles of Internal Medicine 22E, p. 1456–1457
Differential Diagnosis of Left Axis Deviation (−45° to −90°)
| Cause | Distinguishing features |
|---|---|
| LAFB | qR in I/aVL; rS in II/III/aVF; normal QRS width |
| LVH | Voltage criteria met; broader QRS; strain pattern |
| Inferior MI | Pathologic Q waves in II/III/aVF |
| LBBB | Wide QRS (≥120 ms); broad notched R in I/aVL; no septal q in I |
| WPW (right-sided pathway) | Short PR, delta wave |
| Hyperkalemia | Wide, bizarre QRS; peaked T waves |
| Emphysema/RVH | Clinical context; right axis more typical |
Summary
LAFB is a partial left bundle branch system block causing isolated left axis deviation (−45° to −90°) with normal QRS duration, a qR pattern in I/aVL, and rS in II/III/aVF. It is the most common fascicular block, often incidental, but gains clinical importance as part of bifascicular/trifascicular block or in the context of acute ischemia.
This is a shared conversation. Sign in to Orris to start your own chat.