Prisms in Ophthalmology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a thorough answer. Let me compile the full response.
Prisms in Ophthalmology
1. Definition and Basic Optics
A prism is a transparent optical element with a triangular cross-section. It deviates (refracts) light toward its base, while the image appears displaced toward the apex. The critical relationship is:
1 prism dioptre (Δ) = the power required to deviate a ray of light by 1 cm at a distance of 1 metre
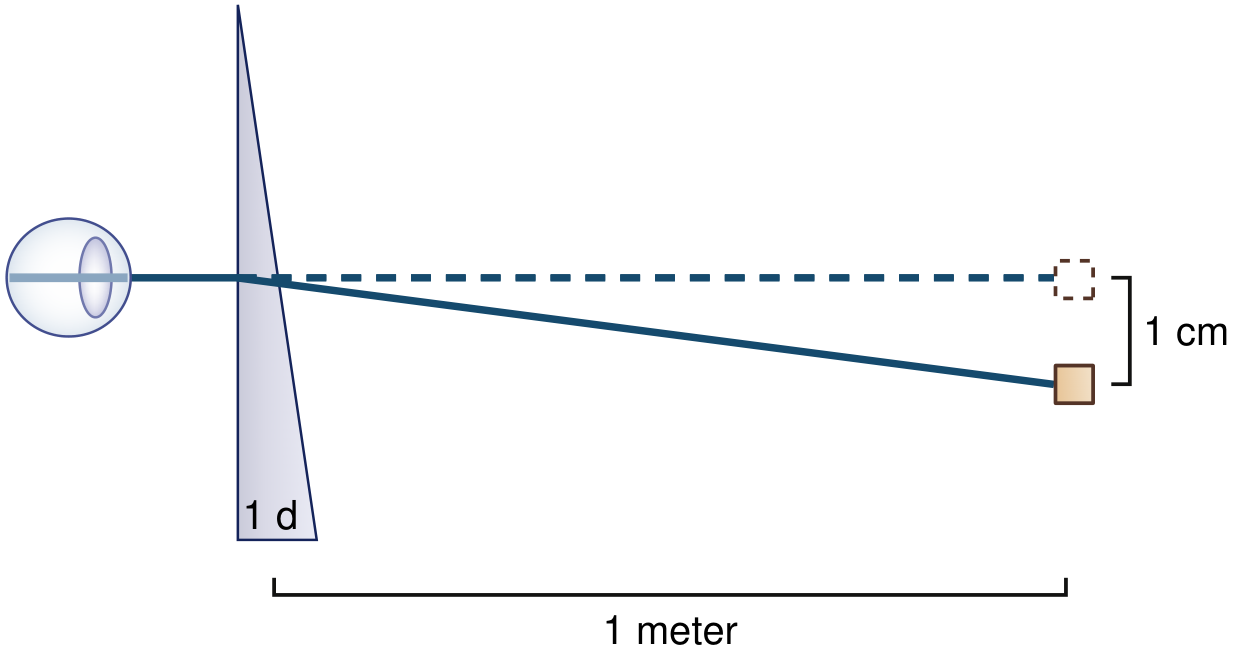
Fig. 18.19 - Bradley and Daroff's Neurology in Clinical Practice
Other useful equivalencies:
- 1 mm of corneal light reflex displacement ≈ 7° of ocular deviation (Hirschberg estimate)
- 1° of ocular deviation ≈ 2 prism dioptres (Δ)
The prism dioptre symbol is Δ. Prism powers used clinically range from 1Δ (diagnostic tests) up to 40Δ or more for correction of large deviations.
2. Types of Prisms Used Clinically
| Type | Description | Use |
|---|---|---|
| Glass/plastic trial prisms | Individual prisms of set powers | Diagnostic testing |
| Prism bar | A column of prisms of increasing progressive strength (e.g. 1-45Δ) | Prism cover test, fusional amplitudes |
| Fresnel prism | Thin press-on plastic prism stuck to spectacle lens | Temporary/trial correction of diplopia or deviation; large powers without weight |
| Permanent spectacle prism | Ground into spectacle lens | Chronic, stable small deviations |
3. Prism Orientation Rules
- Light is bent toward the base of the prism
- The image is displaced toward the apex
- The eye must rotate toward the base to re-fixate - so the eye moves in the direction of the base
- Convention: prism orientation is named by its base position:
- Base-out (BO) - base is temporal; induces convergence
- Base-in (BI) - base is nasal; induces divergence
- Base-up (BU) / Base-down (BD) - for vertical deviations
- To correct a deviation: place the prism with its base in the direction of the deviation (apex toward fixation)
- Right esotropia → base-out prism before the right eye
- Right hypertropia → base-down prism before the right eye
4. Diagnostic Uses
4a. Hirschberg Test (Corneal Reflex Estimation)
A penlight is held ~30 cm from the patient. The position of the corneal light reflex is noted:
- Each 1 mm of decentration ≈ 7° ≈ 14Δ
- Reflex at pupil margin (~2 mm from centre) ≈ ~15°
- Reflex at limbus ≈ ~45°
This is a quick, objective estimate - useful in children or uncooperative patients.
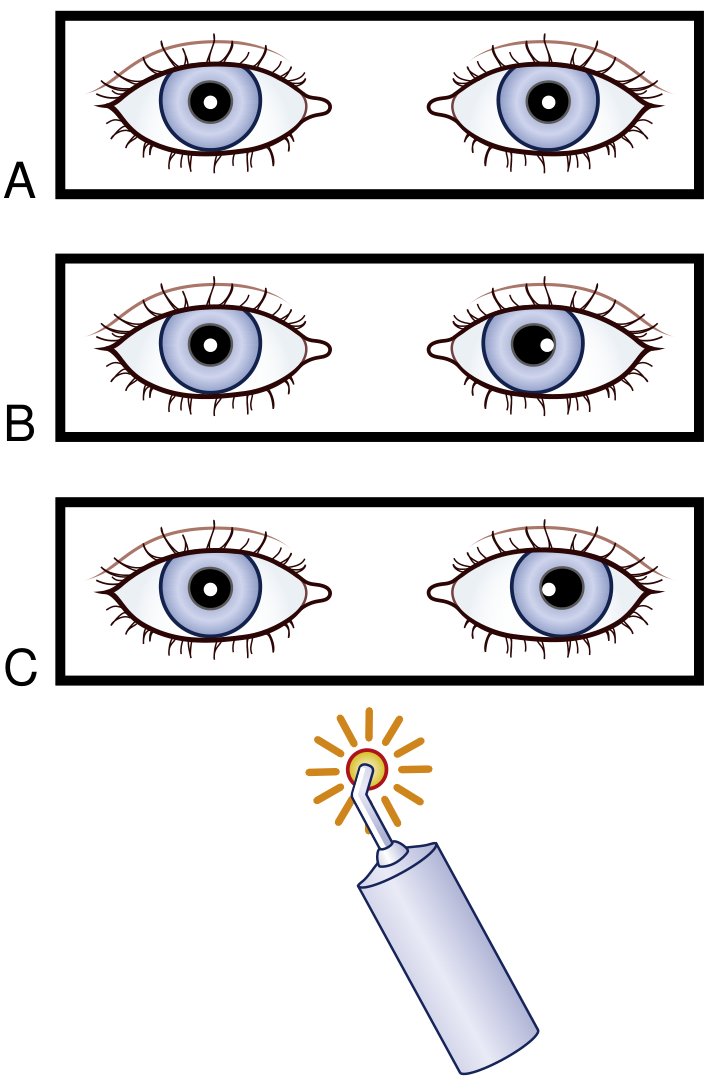
Fig. 18.18 - Bradley and Daroff's Neurology in Clinical Practice
4b. Krimsky Test
Prisms are placed in front of the fixating eye and increased until the corneal light reflections become symmetrical. This reduces parallax error and is preferred over the prism reflection test (where prisms are placed in front of the deviating eye).
4c. Prism Cover Test (Gold Standard for Measuring Deviation)
This is the most accurate clinical method for measuring the angle of strabismus. Procedure:
- The alternate cover test is first performed to establish direction and approximate extent of deviation
- Prisms of increasing strength are placed in front of one eye with the base opposite the direction of deviation (e.g. base-out for esotropia, base-down for right hypertropia)
- The alternate cover test is performed continuously as stronger prisms are introduced (typically via a prism bar)
- The re-fixation movement gradually decreases as prism power approaches the deviation magnitude
- End-point: no movement is seen; the prism strength at which movement reverses and then neutralizes gives the angle of deviation
Performed in: primary position (distance and near), the eight diagnostic positions of gaze, and - for intermittent exotropia - far distance fixation.
4d. 20Δ Base-Out Prism Test (Fusion Test in Infants)
Used to detect fusion in infants without manifest squint:
- A 20Δ base-out prism is placed in front of one eye (say, the right eye)
- This displaces the retinal image temporally, causing diplopia
- The right eye adducts (to re-fixate), and by Hering's law, the left eye abducts
- The left eye then makes a fusional re-adduction convergence movement
- On removing the prism, both eyes re-fixate correctly
Most children with good binocular single vision (BSV) can overcome a 20Δ prism from age 6 months. Weaker prisms (12Δ, 16Δ) may be tried if needed, though the response is harder to interpret.
4e. 4Δ Base-Out Prism Test (Microtropia / Central Suppression Scotoma)
This test distinguishes bifoveal fixation from foveal suppression (central suppression scotoma - CSS) in microtropia:
With bifoveal fixation:
- The 4Δ prism placed base-out causes both eyes to shift away from prism base, then the fellow eye makes a fusional re-fixation movement
In left microtropia (with CSS):
- When placed over the microtropic left eye: the image falls within the CSS - no movement of either eye is observed
- When placed over the right (fixing) eye: the right eye adducts; the left eye moves by Hering's law, but the second image again falls within the CSS - no re-fixation saccade is seen
This absence of the fusional re-fixation saccade is the diagnostic positive result.
4f. Prism and Alternate Cover Test (PACT) - Wills Eye Manual
From the Wills Eye Manual: With a prism bar, slowly increase the amount of base-out prism in front of one eye until the patient notes double vision (the break point) and then slowly reduce until a single image is restored (the recovery point). This measures fusional vergence amplitudes.
4g. Fusional Amplitude Measurement
Prism bars or the synoptophore are used to measure fusional amplitudes:
- An increasingly strong prism is placed before one eye
- The eye abducts (base-in prism) or adducts (base-out prism) to maintain bifoveal fixation
- When the prism exceeds the fusional amplitude, diplopia is reported or one eye drifts - this marks the limit of vergence ability
Normal fusional vergence values:
| Type | Normal Range |
|---|---|
| Convergence (base-out) | ~15-25Δ at distance; larger at near |
| Divergence (base-in) | ~6-10Δ at distance |
| Vertical fusion | ~2-4Δ |
5. Therapeutic / Corrective Uses
5a. Prismatic Correction in Spectacles (Permanent Prisms)
- Used for small, stable residual deviations after strabismus surgery (or as an alternative to surgery)
- Ground into spectacle lenses - suitable for deviations up to approximately 10-15Δ (larger prisms are heavy and produce visual distortion)
- Used especially in lateral rectus palsy: mild residual deviation may be treated with a prism incorporated into spectacles
- Also in skew deviation: prismatic correction in spectacles, along with botulinum injections and vertical muscle surgery in persistent cases
5b. Fresnel Press-On Prisms
- Thin, lightweight Fresnel prisms can be pressed onto existing spectacle lenses
- Allow much larger prism powers without the weight/thickness of ground-in prisms
- Used for temporary correction while awaiting surgery or spontaneous recovery (e.g. in microvascular CN VI palsy)
- Also useful to assess tolerance before committing to permanent spectacle prisms
- From Kanski's: "Observation with monocular occlusion or prismatic (e.g. temporary Fresnel stick-on) correction of diplopia is appropriate in idiopathic and presumed microvascular lesions"
5c. Postoperative Diplopia Test (Pre-surgical Screening)
This test is mandatory before strabismus surgery in all non-binocular patients over 7-8 years of age:
- Corrective prisms are placed in front of one eye (usually the deviating eye)
- The patient fixates a straight-ahead target with both eyes open
- Prisms are slowly increased to significantly overcorrect the angle
- The patient reports whether diplopia occurs at any point
- If suppression persists throughout: little risk of postoperative diplopia
- If diplopia occurs (e.g. from 30Δ in a consecutive exotropia of 35Δ): indicates high risk; botulinum toxin test should be considered
6. Prisms in Vergence / AC:A Ratio Assessment
The AC:A (accommodative convergence to accommodation) ratio is expressed in prism dioptres per dioptre:
- Normal: 3-5Δ per dioptre
- Abnormalities of the AC:A ratio are central to the aetiology of several types of strabismus (e.g. high AC:A esotropia)
7. Summary Table: Prism Tests and Their Purposes
| Test | Prism Used | Purpose |
|---|---|---|
| Hirschberg | None (estimate from reflex position) | Screen/estimate angle of deviation |
| Krimsky | Prism over fixating eye | Objective measurement of deviation |
| Prism Cover Test | Prism bar, alternate cover | Gold-standard angle measurement |
| 20Δ base-out test | 20Δ base-out | Fusion detection in infants |
| 4Δ base-out test | 4Δ base-out | Diagnose microtropia/CSS |
| Fusional amplitude | Prism bar, increasing | Measure convergence/divergence reserves |
| Postop diplopia test | Corrective prism | Pre-surgical diplopia risk assessment |
| Prism in spectacles | Fresnel/ground-in | Correct residual deviation/diplopia |
8. Clinical Pearls
- "Base opposite the direction of deviation": to measure esotropia use base-out, for exotropia use base-in, for right hypertropia use base-down before the right eye
- Prism bar vs. loose prisms: prism bars are preferred for the prism cover test because they allow rapid sequential changes; loose prisms are used in trial frames
- Large deviations: ground-in prisms are impractical above ~15Δ due to weight and optical distortion; Fresnel prisms or surgery are preferred
- Botulinum toxin + prismatic correction: botulinum to ipsilateral medial rectus can sometimes facilitate prismatic correction in large deviations (e.g. VI nerve palsy) by temporarily reducing the angle
- Prism dioptres vs degrees: remember 1° ≈ 2Δ; the Hirschberg reflex estimate gives 1 mm ≈ 7° ≈ 14Δ
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed.; The Wills Eye Manual; Bradley and Daroff's Neurology in Clinical Practice
Give as EXAM ANSWER
Prisms in Ophthalmology
Definition
A prism is a transparent optical element with a triangular cross-section that refracts light toward its base, while the perceived image is displaced toward the apex.
Prism Dioptre (Δ) — Unit of Prism Power
1 prism dioptre (Δ) = power that deviates a ray of light 1 cm at 1 metre distance
Key conversions:
- 1 mm corneal reflex displacement = 7° of deviation
- 1° = 2 prism dioptres (Δ)
- 1 mm = ~14Δ
Fundamental Rule
| What moves toward BASE | What moves toward APEX |
|---|---|
| Light ray | Perceived image |
| Eye (to re-fixate) | — |
To correct a deviation: place the base in the direction of the deviation
- Esotropia → Base-out (BO)
- Exotropia → Base-in (BI)
- Right hypertropia → Base-down before right eye
Types of Prisms
| Type | Feature | Use |
|---|---|---|
| Glass/plastic trial prism | Fixed powers | Diagnostic testing |
| Prism bar | Column of prisms in increasing steps | Prism cover test, fusional amplitudes |
| Fresnel (press-on) prism | Thin, lightweight, large powers possible | Temporary correction; trial before surgery |
| Ground-in spectacle prism | Incorporated into lens (up to ~15Δ practical) | Permanent small deviation correction |
Diagnostic Uses
1. Hirschberg Test
- Penlight held 30 cm from patient; corneal reflex position is estimated
- 1 mm decentration = 7° = ~14Δ
- Reflex at pupil margin (~2 mm) = ~15°
- Reflex at limbus = ~45°
- Quick, objective; useful in children/uncooperative patients
- No prism is used — this is estimation only
2. Krimsky Test
- Prisms placed in front of the fixating eye until corneal light reflexes are symmetrical in both eyes
- More accurate than the prism reflection test (prism over deviating eye)
- Reduces parallax error
- Used when cover test is not possible (poor cooperation)
3. Prism Cover Test (Gold Standard)
Purpose: Measures the full angle of deviation (manifest + latent)
Procedure:
- Perform the alternate cover test first — establishes direction and approximate angle
- Place prism of increasing strength in front of one eye with base opposite to direction of deviation
- Continue alternate cover testing while increasing prism strength (using a prism bar)
- Re-fixation movement gradually diminishes as prism approaches the true angle
- End-point = no movement; can increase further until reversal occurs, then reduce to neutral
Performed in: primary position (distance + near), all 8 diagnostic positions, and far-distance (for intermittent exotropia)
4. 20Δ Base-Out Prism Test (Fusion test in infants)
Purpose: Detect binocular fusion in infants without manifest squint
Procedure:
- 20Δ base-out placed before one eye
- Displaces image temporally → diplopia stimulus
- Expected response (fusion present):
- Both eyes shift away from prism base (Hering's law)
- Fellow eye makes fusional re-adduction convergence movement
Normal: Children with good BSV overcome 20Δ from age 6 months
5. 4Δ Base-Out Prism Test (Microtropia / Central Suppression Scotoma)
Purpose: Distinguish bifoveal fixation from a central suppression scotoma (CSS)
| Condition | Result |
|---|---|
| Bifoveal fixation (normal) | Eyes shift, then fusional re-fixation saccade occurs |
| Microtropia with CSS | Prism over the microtropic eye → image falls in CSS → no movement |
| Prism moved to fixing eye | Eye adducts, fellow eye moves by Hering's law, but image again falls in CSS → no re-fixation saccade |
The absence of the re-fixation saccade = positive test for CSS
6. Fusional Amplitude Measurement
Purpose: Measure the efficacy (range) of vergence movements
Method: Progressively increasing prism before one eye; eye abducts/adducts to maintain bifoveal fixation; diplopia or drift = limit of fusion (break point)
| Vergence | Normal Range |
|---|---|
| Convergence (base-out) | ~15–25Δ at distance; larger at near |
| Divergence (base-in) | ~6–10Δ at distance |
| Vertical fusion | ~2–4Δ |
7. Postoperative Diplopia Test (Pre-surgical screening)
Mandatory before strabismus surgery in all non-binocular patients >7–8 years
Procedure:
- Corrective prisms placed before deviating eye
- Angle is progressively overcorrected
- Patient reports if diplopia occurs
| Finding | Significance |
|---|---|
| Suppression throughout | Little risk of postoperative diplopia — surgery safe |
| Diplopia occurs | High risk — consider botulinum toxin test first |
Therapeutic Uses
1. Fresnel Press-On Prisms
- Pressed onto existing spectacle lens
- Allow large powers without lens weight/thickness
- Used for temporary correction while awaiting surgery or spontaneous recovery (e.g. microvascular VI nerve palsy, thyroid eye disease)
- Also used to assess tolerance before permanent prism prescription
2. Permanent Prism in Spectacles
- Ground into spectacle lenses
- Practical for deviations up to ~10–15Δ (beyond this: heavy, distorting)
- Indicated for small, stable residual deviations after surgery
- Also used in: lateral rectus palsy (residual deviation), skew deviation, decompensated phorias
3. Prism + Botulinum Toxin (in CN VI Palsy)
- Botulinum injected into ipsilateral medial rectus to reduce the angle
- Facilitates prismatic correction of large deviation while awaiting recovery
AC:A Ratio and Prisms
Accommodative Convergence to Accommodation (AC:A) ratio:
- Expressed as prism dioptres per dioptre (Δ/D)
- Normal: 3–5Δ/D
- High AC:A → convergence excess esotropia
- Low AC:A → convergence insufficiency
Summary: Prism Tests at a Glance
| Test | Prism | Key Purpose |
|---|---|---|
| Hirschberg | None (reflex estimation) | Screen/estimate angle |
| Krimsky | Over fixating eye | Objective angle in uncooperative patients |
| Prism Cover Test | Prism bar + alternate cover | Gold standard angle measurement |
| 20Δ base-out | 20Δ base-out | Fusion detection — infants |
| 4Δ base-out | 4Δ base-out | Diagnose microtropia / CSS |
| Fusional amplitude | Prism bar, increasing | Convergence/divergence reserves |
| Postop diplopia test | Corrective prism (overcorrect) | Pre-surgical diplopia risk |
| Fresnel / spectacle prism | Fresnel or ground-in | Treat residual deviation / diplopia |
High-Yield Points for Exams
- Prism dioptre = 1 cm deviation at 1 m
- Image moves to apex; eye moves to base
- Base opposite to deviation to correct or measure
- Prism cover test = gold standard for measuring strabismus angle
- 4Δ test — no re-fixation saccade = CSS = microtropia
- 20Δ test — absent fusional response before 6 months = abnormal fusion
- Fresnel prisms = temporary, large deviation; ground-in = permanent, small deviation
- Postop diplopia test is mandatory before strabismus surgery in patients >7–8 years
- 1° = 2Δ; 1 mm Hirschberg = 7° = ~14Δ
- Normal AC:A ratio = 3–5Δ/D
This is a shared conversation. Sign in to Orris to start your own chat.