Diabetic keto acidosis
Reading File
Finding Sources
Searching PubMed
"diabetic ketoacidosis"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive information to write a thorough DKA summary. Let me compile it:
Diabetic Ketoacidosis (DKA)
Definition & Diagnostic Triad
The three fundamental biochemical features of DKA are:
- Hyperglycemia (blood glucose typically >250 mg/dL, though may be lower in euglycemic DKA)
- Ketonemia/ketonuria (urinary ketones 2+ or more, or serum β-hydroxybutyrate ≥3.0 mmol/L)
- Acidosis (arterial/venous pH <7.3, serum bicarbonate <18 mmol/L)
DKA occurs predominantly in Type 1 diabetes (~25% of episodes represent new-onset diabetes), but can occur in Type 2 under significant physiologic stress.
Pathophysiology
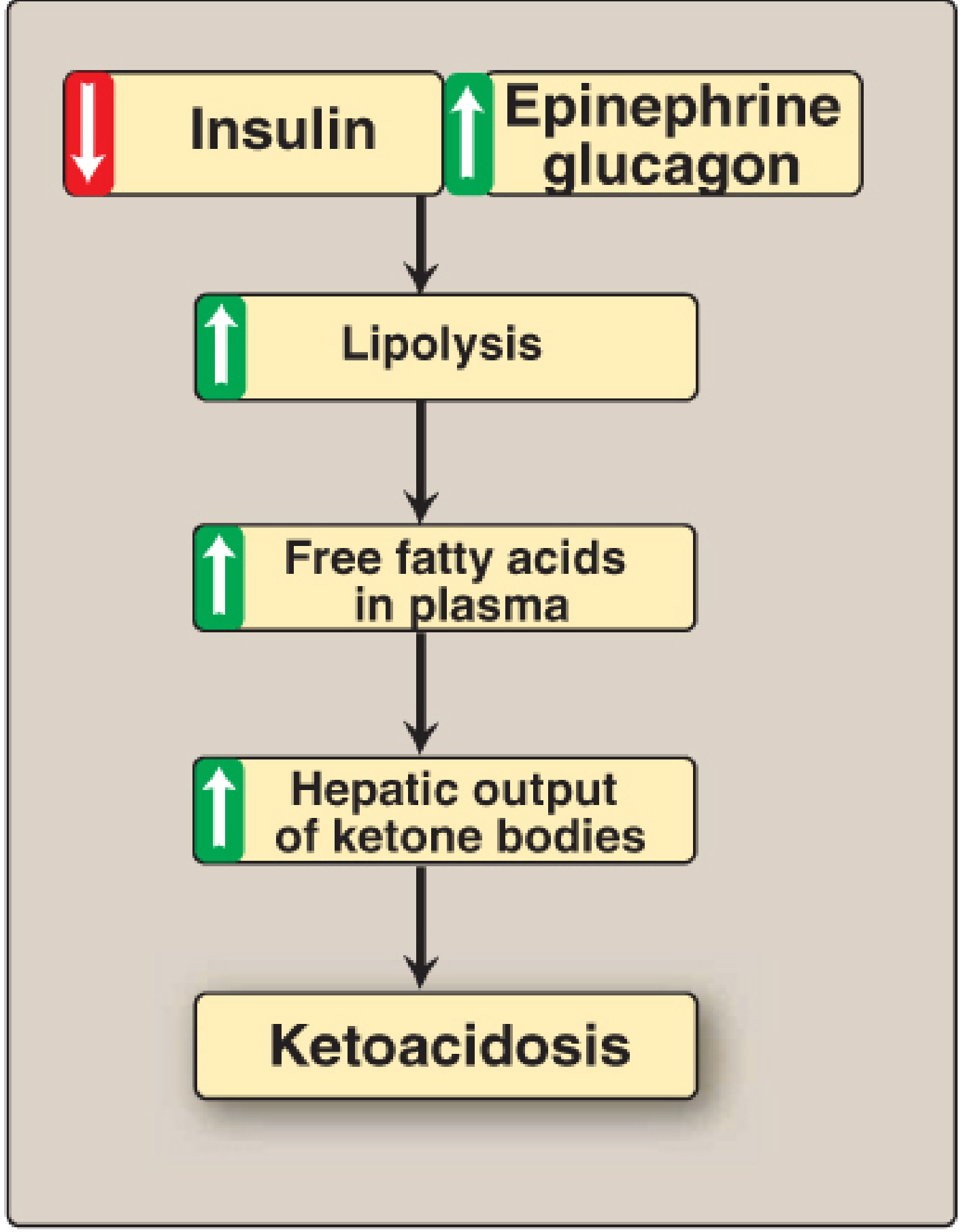
The central defect is combined insulin deficiency + counter-regulatory hormone excess (glucagon, epinephrine, cortisol, GH):
| Process | Mechanism |
|---|---|
| Hyperglycemia | Decreased glucose uptake + increased hepatic gluconeogenesis (from amino acids, lactate, pyruvate) |
| Lipolysis | Hormone-sensitive lipase activated → ↑ free fatty acids (FFAs) in plasma |
| Ketogenesis | FFAs oxidized in liver → acetoacetate + β-hydroxybutyrate + acetone |
| Osmotic diuresis | Glucose exceeds renal threshold → draws water, Na⁺, K⁺, Mg²⁺, Ca²⁺, phosphate into urine |
| Acidosis | Ketone accumulation consumes bicarbonate; anion gap rises |
| Kussmaul breathing | Respiratory compensation to excrete CO₂ and reduce acidosis |
In 95% of patients, total-body sodium is normal or low, yet serum K⁺ may be falsely elevated due to acidosis-driven shift out of cells — masking profound total-body K⁺ depletion.
Precipitants
Most Common:
- Infections (pneumonia, UTI, sepsis)
- Inadequate insulin / non-adherence
- New-onset diabetes
- Acute coronary syndrome
Other Causes:
- Stroke, pulmonary embolism, acute pancreatitis
- Endocrinopathies: Cushing's, thyrotoxicosis, acromegaly
- Drugs: corticosteroids, SGLT-2 inhibitors (euglycemic DKA), clozapine, olanzapine, cocaine, thiazides
Clinical Features
Symptoms (hours to days):
- Polyuria, polydipsia, polyphagia
- Nausea, vomiting, anorexia
- Abdominal pain (~50% of patients, especially children)
- Weakness, lethargy, weight loss
Signs:
- Kussmaul breathing (deep, rapid respirations)
- Fruity/acetone odor on breath
- Tachycardia, orthostatic hypotension, or frank hypotension
- Dry mucous membranes (dehydration 5–10 L deficit)
- Altered mental status → coma in severe cases
- Fever rare from DKA itself — suggests infection
Laboratory Findings
| Parameter | DKA | HHS (comparison) |
|---|---|---|
| Glucose | >350 mg/dL | >700 mg/dL |
| Serum sodium | Low 130s mEq/L | 140s mEq/L |
| Potassium | 4.5–6.0 mEq/L (elevated initially) | ~5 mEq/L |
| Bicarbonate | <10 mEq/L | >15 mEq/L |
| BUN | 25–50 mg/dL | >50 mg/dL |
| Serum ketones | Present | Absent |
| pH | <7.3 (severe: <7.0) | >7.3 |
| Anion gap | Elevated | Normal/mildly elevated |
Key labs: ABG, BMP, serum/urine ketones (or bedside β-hydroxybutyrate), CBC, urinalysis, cultures, ECG, lipase if pancreatitis suspected.
⚠️ Ketone testing caveat: Nitroprusside strips detect only acetoacetate — NOT β-hydroxybutyrate (the predominant ketone). Results may appear falsely low. Bedside capillary β-hydroxybutyrate monitors are preferred.
Average Fluid/Electrolyte Deficits in Severe DKA (adult ≥20 kg):
- Water: 70–90 mL/kg
- Sodium: 8–10 mEq/kg
- Potassium: 5–7 mEq/kg
- Phosphorus: ~3 mEq/kg
Treatment
1. Fluids
- Initial: 0.9% NaCl (normal saline), 2–4 L over first 2–4 hours
- Children: 20 mL/kg NS in first hour
- When glucose ≤300 mg/dL → switch to D5W/0.45% NS to prevent hypoglycemia while continuing insulin
- Balanced electrolyte solutions (e.g., Lactated Ringer's) show faster DKA resolution vs. 0.9% NS in recent meta-analyses (PMID: 38925619)
2. Insulin
- Regular insulin 0.1 units/kg/hour IV infusion
- Do NOT start insulin if K⁺ < 3.3 mEq/L — replace potassium first
- Recent evidence supports subcutaneous basal insulin co-administered with IV insulin infusion to reduce rebound hyperglycemia after infusion stops (PMID: 41208563); subcutaneous insulin protocols may be non-inferior to IV infusion in mild-moderate DKA (PMID: 39090718)
3. Potassium
- Add 20–40 mEq KCl per liter when K⁺ < 5.5 mEq/L and urine output confirmed
- If K⁺ > 5.5 mEq/L → hold K⁺ replacement, monitor closely
- If K⁺ < 3.5 mEq/L → aggressive IV replacement before insulin
4. Phosphorus & Magnesium
- Phosphorus: routine replacement generally not required
- Magnesium: correct if low with 1–2 g MgSO₄ IV
5. Bicarbonate
- Routine use not recommended; consider only if pH < 6.9 with hemodynamic instability
- Bicarbonate can paradoxically worsen intracellular acidosis and hypokalemia
6. Treat Precipitant
- Identify and treat the underlying cause (infection, MI, medication non-adherence)
Monitoring
- Vital signs and urine output continuously
- Serum glucose hourly
- Electrolytes (K⁺, HCO₃⁻, Cl⁻), BUN, pH every 2–4 hours
- ECG monitoring (K⁺ changes)
Resolution Criteria
- Glucose < 200 mg/dL
- Serum bicarbonate ≥ 15 mEq/L
- Venous pH > 7.3
- Anion gap normalized
Transition to subcutaneous insulin only after oral intake tolerated and IV insulin overlap by 1–2 hours.
Complications of DKA and Treatment
- Cerebral edema (most feared complication, especially in children — from rapid osmolality shifts)
- Hypoglycemia (from excessive insulin)
- Hypokalemia (from insulin-driven K⁺ shift)
- Hyperchloremic non-anion gap metabolic acidosis (from large-volume NS)
- Aspiration (in altered mental status)
DKA vs. HHS at a Glance
| Feature | DKA | HHS |
|---|---|---|
| Insulin deficiency | Absolute | Relative |
| Onset | Hours–days | Days–weeks |
| Ketosis | Prominent | Absent/mild |
| Acidosis | Severe | Absent/mild |
| Osmolality | Mildly elevated | Markedly elevated |
| Mortality | 1–5% | Up to 15% |
Sources: Goldman-Cecil Medicine (9780323930345), Rosen's Emergency Medicine (9780323757898), Lippincott Biochemistry (9781975155063)
Recent Evidence:
- Balanced crystalloids (LR) resolve DKA faster than 0.9% NS — Szabó et al., 2024 (Meta-analysis, PMID 38925619)
- Subcutaneous vs. IV insulin in DKA management — Alnuaimi et al., 2024 (Systematic Review, PMID 39090718)
- Early subcutaneous basal insulin co-administration — Thammakosol et al., 2026 (Meta-analysis, PMID 41208563)
This is a shared conversation. Sign in to Orris to start your own chat.