internuceurb opthakmopegia
Reading File
search_medical_text
internuclear ophthalmoplegia INO medial longitudinal fasciculus clinical features
search_medical_text
internuclear ophthalmoplegia causes diagnosis multiple sclerosis treatment
search_medical_image
internuclear ophthalmoplegia eye movements diagram
GradeResponse
GradeResponse
GradeResponse
Internuclear Ophthalmoplegia (INO)
Anatomy & Pathophysiology
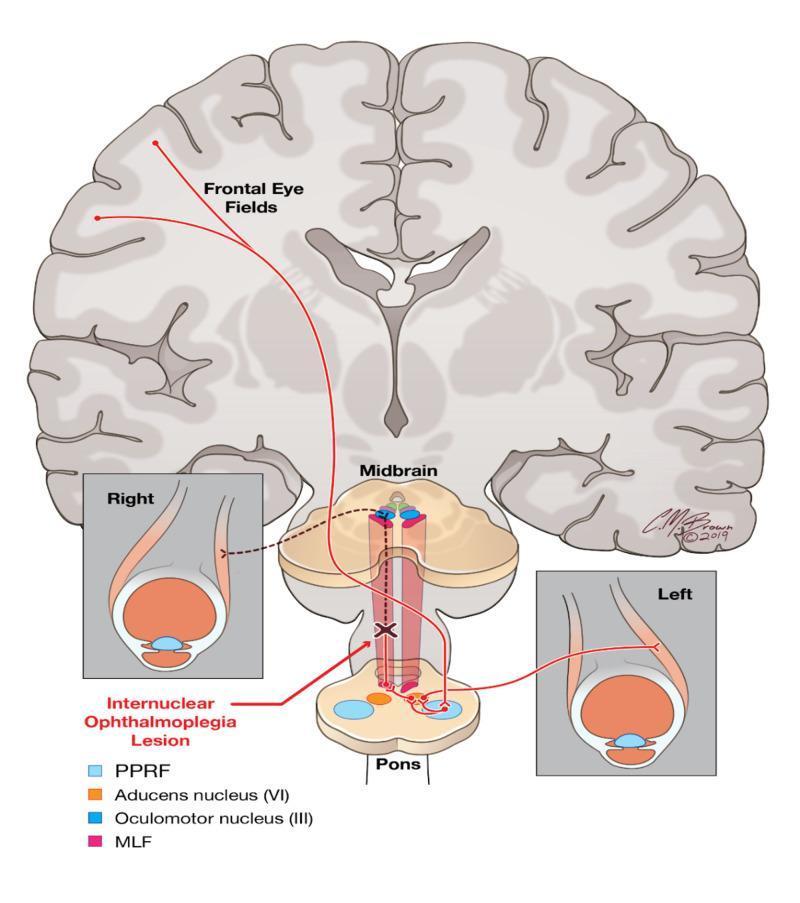
INO results from a lesion in the medial longitudinal fasciculus (MLF) — the white matter tract that ascends from the abducens nucleus (CN VI) in the pons to the oculomotor nucleus (CN III) in the midbrain. This tract coordinates horizontal conjugate gaze by relaying a signal from abducens interneurons to contralateral medial rectus motor neurons.
When the MLF is damaged, this cross-midline communication is severed, causing failure of adduction of the ipsilateral eye on attempted contralateral gaze, while the contralateral eye abducts normally (often with nystagmus).
Clinical Presentation
| Feature | Description |
|---|---|
| Ipsilateral eye | Slowed or absent adduction on attempted lateral gaze |
| Contralateral eye | Full abduction, often with abducting nystagmus |
| Convergence | Often preserved (uses a different pathway) |
| Bilateral INO | Both eyes fail to adduct; strongly suggests MS |
Example: A left INO = left eye fails to adduct when looking right, while the right eye abducts with nystagmus.
Causes
| Cause | Notes |
|---|---|
| Multiple sclerosis | Most common; typically younger patients, often bilateral |
| Brainstem stroke | Most common cause in older patients; typically unilateral |
| Tumor | Brainstem glioma, metastasis |
| Trauma | Brainstem injury |
| Wernicke's encephalopathy | Thiamine deficiency |
| Other | Infection, vasculitis, anti-NMDAR encephalitis |
Rule of thumb: Bilateral INO in a young person = MS until proven otherwise. Unilateral INO in an older patient = vascular (stroke).
Diagnosis
- Clinical exam is key: observe for adduction lag and contralateral abducting nystagmus
- MRI brain/brainstem (with DWI if acute): identifies demyelinating plaques or infarct in the MLF
- Work up the underlying cause (MS panel, vascular risk factors, etc.)
Associated Syndromes
- WEBINO (Wall-Eyed Bilateral INO): bilateral INO with exotropia at rest
- One-and-a-half syndrome: ipsilateral gaze palsy + INO — lesion involves both the PPRF/abducens nucleus AND the MLF on the same side; only preserved movement is contralateral abduction
Management
Treatment is directed at the underlying cause:
- MS: corticosteroids for acute relapse; disease-modifying therapy long-term
- Stroke: standard ischemic stroke management (thrombolysis/thrombectomy if eligible, antiplatelets, risk factor control)
- Symptomatic: prism glasses or patching may help with diplopia; INO from MS or stroke often improves spontaneously
(Harrison's Principles of Internal Medicine, 21st ed., p. 989)
This is a shared conversation. Sign in to Orris to start your own chat.