Perianal fistula
Reading File
Finding Sources
Searching PubMed
"perianal fistula" management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Excellent data. I now have comprehensive information from Sabiston, Bailey & Love, and Harrison's. Let me compile the full answer.
Perianal Fistula (Fistula-in-Ano)
Definition and Pathophysiology
A perianal fistula is a chronic abnormal communication extending from the anorectal lumen (the internal opening) to an external opening on the perianal skin, perineum, or buttock (or rarely to the vagina in women). The vast majority are cryptoglandular in origin - arising from infection of anal glands that open at the dentate line. Fistulae are lined by granulation tissue, not epithelium.
The sequence: anal gland infection → perianal abscess → spontaneous or surgical drainage → persistent communication = fistula. Approximately 30-50% of perianal abscesses will ultimately develop into a fistula. - Sabiston Textbook of Surgery, p. 2162; Harrison's Principles, p. 2628
Aetiology
| Category | Examples |
|---|---|
| Cryptoglandular (majority) | Idiopathic anal gland sepsis |
| Inflammatory bowel disease | Crohn's disease (most common IBD cause) |
| Infections | Tuberculosis, lymphogranuloma venereum, actinomycosis |
| Malignancy | Can arise within a longstanding fistula |
| Miscellaneous | Foreign body, rectal duplication, radiation |
- Bailey & Love's Short Practice of Surgery, 28th ed., p. 1457
Classification - Parks' System
The most widely used classification is based on the relationship of the primary tract to the external anal sphincter:
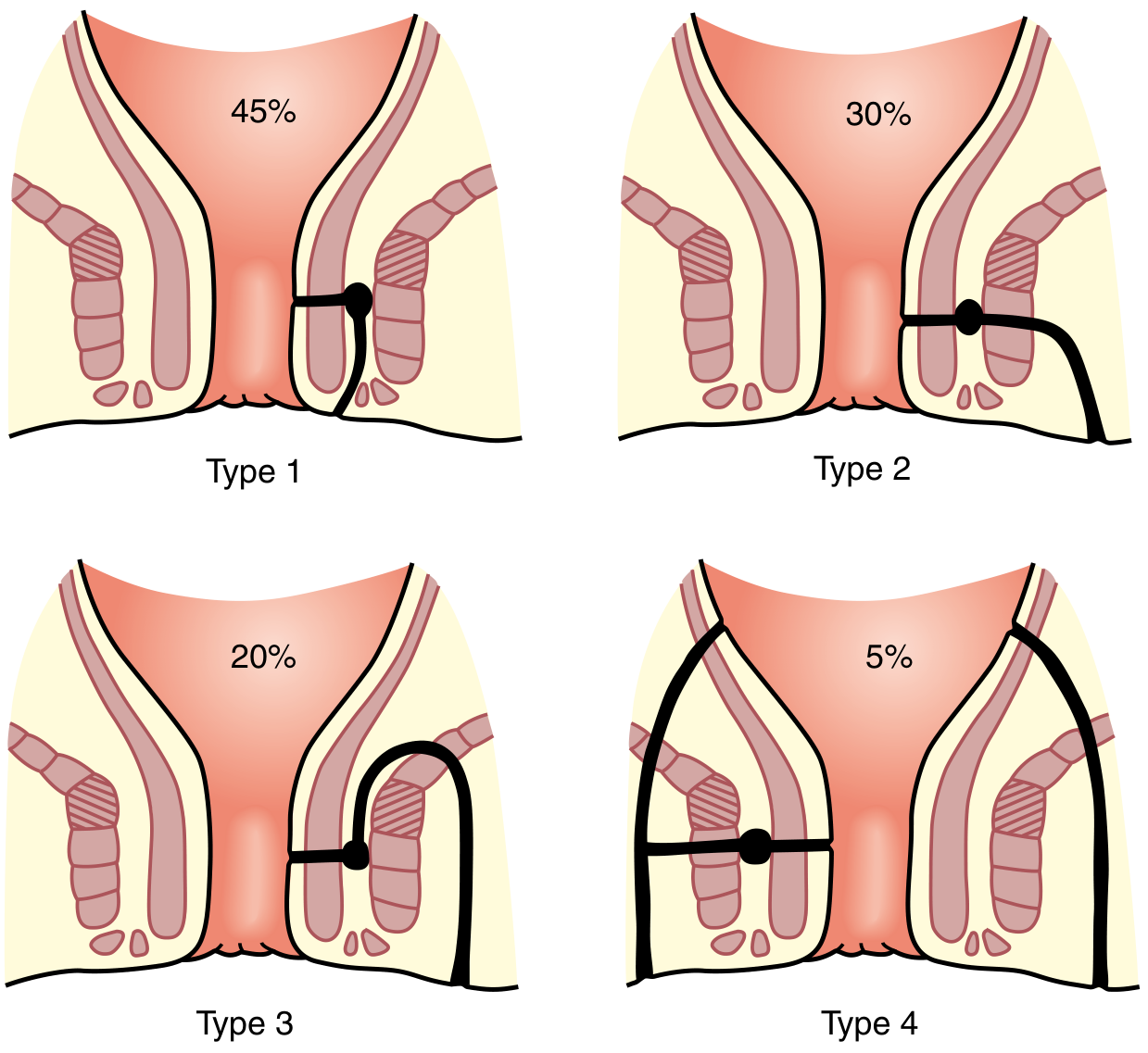
| Type | Description | Frequency |
|---|---|---|
| Type 1 - Intersphincteric | Track confined to the intersphincteric plane; does not cross the external sphincter | 45% |
| Type 2 - Transsphincteric | Crosses both internal and external sphincters; passes through ischiorectal fossa to perianal skin | 30-40% |
| Type 3 - Suprasphincteric | Track rises above puborectalis, curves down through levators and ischioanal fossa | 20% |
| Type 4 - Extrasphincteric | No specific relation to sphincters; usually from pelvic disease or trauma | 5% |
The American Gastroenterology Association (AGA) classification simplifies this into:
-
Simple fistula: low (superficial, low intersphincteric or low transsphincteric), single external opening
-
Complex fistula: high tract, extra- or suprasphincteric, associated abscess, anovaginal, anal stricture, or prior radiation/IBD
-
Bailey & Love's, p. 1457-1458
Clinical Features
- Intermittent purulent (sometimes bloody) discharge from the external opening
- Cyclical pain and swelling that temporarily resolves upon drainage
- History of prior anorectal abscess in most cases
- Passage of flatus/faeces through external opening suggests a rectal (rather than anal) internal opening
- Bilateral external openings → suspect a fistula involving the deep postanal space
- Multiple external openings ("watering can perineum") → strongly suggests perianal Crohn's disease
Goodsall's Rule
This rule predicts the internal opening based on the location of the external opening:
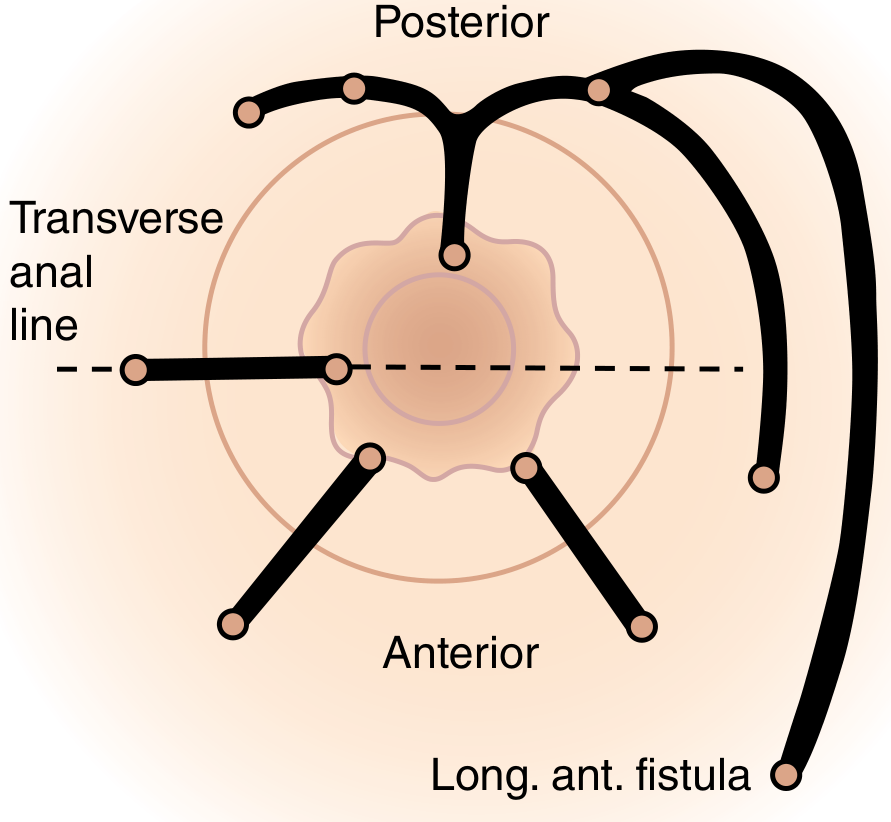
-
Anterior external opening (anterior to transverse anal line): track runs radially (directly) into the nearest anal crypt
-
Posterior external opening: track runs curvilinearly to a posterior midline internal opening
-
Exception: A fistula opening >3 cm from the anal verge anteriorly may be an anterior extension of a horseshoe fistula originating posteriorly
-
Sabiston, p. 2163; Harrison's, p. 2629
Investigations
Clinical Assessment
- Full history including obstetric, GI, anal surgical, and continence history
- Proctosigmoidoscopy to exclude IBD, malignancy
- Key goals: identify internal opening, external opening(s), primary track course, secondary extensions
Intraoperative
- Gentle fistula probe passed from external to internal opening
- Hydrogen peroxide / methylene blue / milk injected through external opening to identify the internal opening
- Examination under anaesthesia (EUA) is the gold standard for fistula evaluation
Imaging
-
MRI (pelvic/anal fistula protocol): Best modality for complex fistulae; identifies tracts with ~80% accuracy. Preferred for preoperative planning of high/complex fistulae
-
Endoanal ultrasound (EAUS): Useful for sphincter integrity assessment, especially with hydrogen peroxide instillation; comparable to MRI for most fistulae
-
Fistulography and CT have limited accuracy and are not routinely recommended
-
Sabiston, p. 2162-2163; Bailey & Love's, p. 1458-1459
Treatment
The goals of treatment are to:
- Treat undrained infection
- Define fistula anatomy
- Remove or ablate epithelialised tracts
- Avoid/minimize fecal incontinence (the primary risk)
- Prevent recurrence
Simple / Low Fistulae (involving <1/3 of external sphincter)
Fistulotomy (lay-open) - the standard treatment
- The entire fistula tract is unroofed and left to heal by secondary intention
- Success rate: ~94%
- Risk of mild fecal incontinence: ~13% (systematic review); <5% in patients with normal preoperative sphincter function and simple low fistulae
- Recurrence rate: 2-8%
Seton Placement (all complex / high fistulae, uncertain sphincter involvement)
A silastic vessel loop or rubber band is threaded through the fistula tract. Uses:
- Draining seton - maintains tract patency, reduces recurrent infection; allows anatomy to be defined once inflammation subsides (4-6 weeks), then definitive repair
- Cutting seton - progressively tightened to slowly divide the sphincter in a controlled manner; largely fallen out of favour due to incontinence risk
Sphincter-Sparing Procedures (high / complex fistulae)
| Procedure | Description | Success Rate |
|---|---|---|
| Anorectal advancement flap | Mobilization of a flap of rectal mucosa/submucosa/muscle to cover the internal opening | Up to 78% |
| LIFT procedure (Ligation of Intersphincteric Fistula Tract) | Dissection into intersphincteric plane; fistula tract divided and suture-ligated; sphincters preserved | ~65-70% |
| Fibrin glue / Cyanoacrylate glue | Biological plug injected into tract | Lower success (~50%) |
| Anal fistula plug (AFP) | Bioabsorbable plug placed in the tract | Variable; ~50% |
| FiLaC (Fistula Laser Closure) | Radially emitting laser ablates the fistula tract from within | ~65% healing at 24 months |
| Video-Assisted Anal Fistula Treatment (VAAFT) | Endoscopic identification and ablation under direct vision | Promising short-term results |
Sphincter-sparing procedures achieve up to 78% success with no incontinence risk. - Harrison's, p. 2629; Sabiston, p. 2163-2165
Crohn's-Associated Perianal Fistula
This is a particularly challenging subset requiring a multidisciplinary approach:
-
Anti-TNF agents (infliximab, adalimumab) are first-line medical therapy; infliximab has the best evidence (ACCENT II trial)
-
Adalimumab biosimilars show similar efficacy per a 2025 systematic review and meta-analysis (PMID 41267606)
-
Mesenchymal stem cell therapy (darvadstrocel - Alofisel): The ADMIRE trial (n=212) showed fistula remission at 52 weeks in 59% vs 42% placebo; now an established option for complex perianal Crohn's fistulae where anti-TNFs have failed
-
Seton drainage is used to control sepsis before medical therapy
-
Caution with any sphincter-cutting surgery due to already-impaired anorectal function in Crohn's disease
-
A 2025 consensus statement also highlights the risk of fistula-associated anorectal cancer in long-standing Crohn's fistulizing disease
-
Harrison's Principles, 22nd ed., p. 2629-2630
Prognosis and Complications
- Main risk of all surgical treatment: fecal incontinence (ranges from minor soiling to complete loss; dependent on sphincter involvement)
- Recurrence more common with complex/high fistulae
- Untreated fistulae can lead to recurrent abscesses, sepsis, and rarely malignant transformation in very long-standing cases
Key sources: Sabiston Textbook of Surgery, 21st ed.; Bailey & Love's Short Practice of Surgery, 28th ed.; Harrison's Principles of Internal Medicine, 22nd ed. (2025)
This is a shared conversation. Sign in to Orris to start your own chat.