Retro sternal goiter with images of ct
Reading File
Finding Sources
Finding Sources
Searching the Web
retrosternal goiter CT scan imaging findings diagnosis
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content and multiple CT/imaging examples. Here is the full answer:
Retrosternal (Substernal) Goiter
Definition and Terminology
Retrosternal (substernal) goiter refers to an enlarged thyroid gland with extension below the thoracic inlet into the mediastinum. A widely used working definition is: a goiter that requires mediastinal exploration and dissection for complete removal, or one with an intrathoracic component extending >3 cm below the thoracic inlet. The upper limit of the normal thyroid in an iodine-replete adult is ~20 g; anything larger that descends behind the sternum qualifies.
Two subtypes are recognized:
- Goiter with intrathoracic extension - most common; the bulk originates in the neck and descends, maintaining continuity with the cervical thyroid
- Primary intrathoracic (ectopic) goiter - rare; entirely within the mediastinum with no cervical connection, derives from ectopic thyroid tissue
Epidemiology and Etiology
- More common in older women (F:M ~3:1)
- Associated with chronic iodine deficiency and multinodular goiter
- Up to ~5% of all goiters extend substernally
- Can be euthyroid (~80%), subclinically thyrotoxic (~30% with suppressed TSH), or rarely overtly hyperthyroid
Clinical Presentation
Approximately 40% are asymptomatic - often discovered incidentally on chest X-ray. Symptomatic patients present with:
| Symptom/Sign | Mechanism |
|---|---|
| Dyspnea, stridor, orthopnea | Tracheal compression or deviation |
| Dysphagia | Esophageal compression |
| Hoarseness | Recurrent laryngeal nerve compression |
| Pemberton's sign | Facial/cervical congestion + cyanosis on raising arms - indicates raised thoracic inlet pressure |
| SVC syndrome | Venous obstruction - dilated neck/chest veins, facial edema, plethora, papilledema |
| Horner's syndrome | Sympathetic chain compression |
| Chylothorax | Thoracic duct compression |
| Acute distress | Up to 20% - sudden airway compromise |
- Schwartz's Principles of Surgery, 11th ed. - "Retrosternal extension of a large goiter may result in impeded flow in the superior vena cava, leading to dilated veins over the chest wall. This may become more prominent when patients raise their arms above the head - Pemberton's sign."
Imaging
1. Chest X-Ray (CXR)
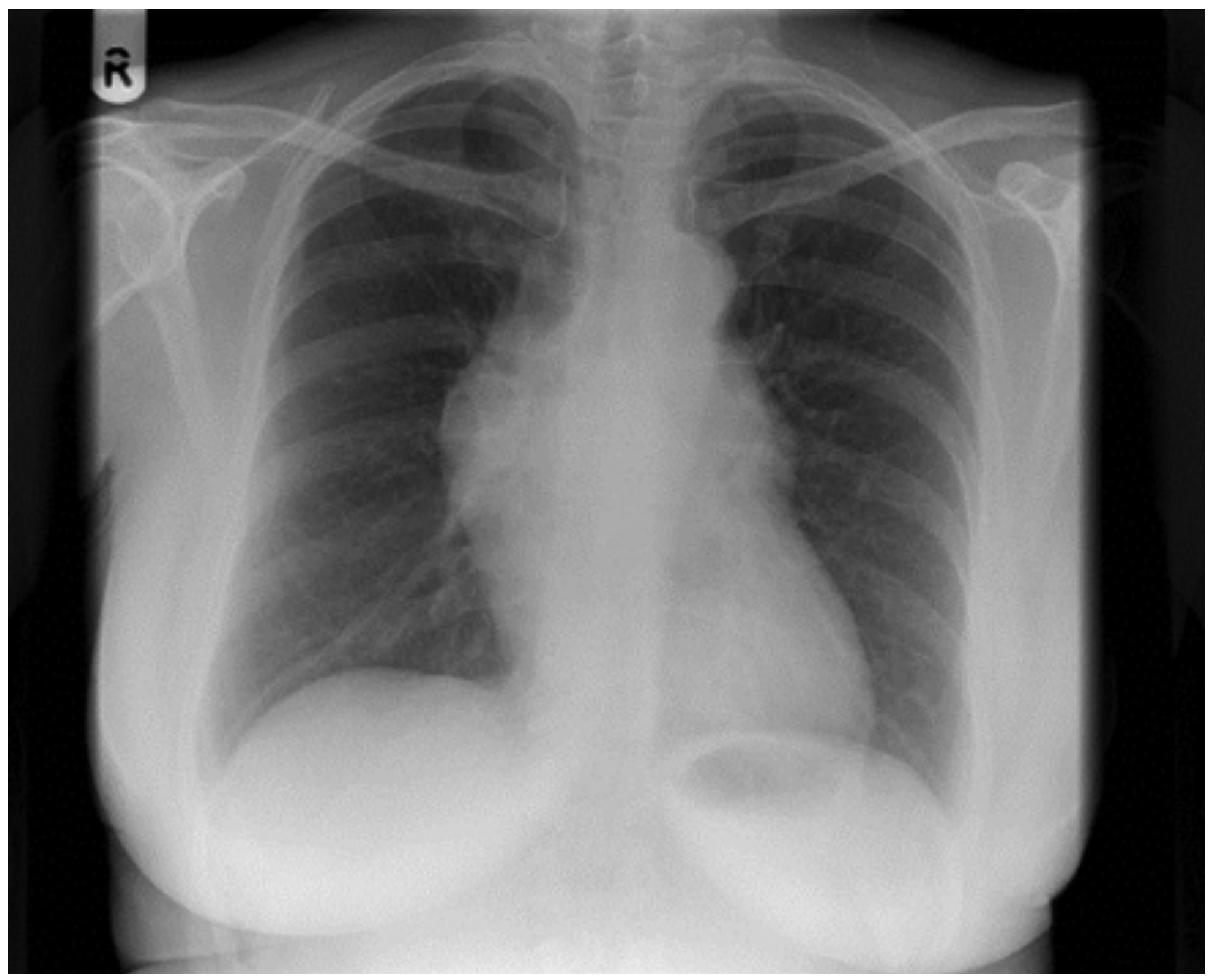
The first clue is often an incidental CXR abnormality. Findings include:
- Superior mediastinal widening (radiopaque mass)
- Tracheal deviation to the opposite side
- Cervicothoracic sign - the superior margin of the mass is not traceable (the mass extends above the thoracic inlet, distinguishing thyroid from vascular causes)
- Calcifications may be visible
Figure 70.1 - Incidental CXR showing mediastinal widening from a primary intrathoracic goiter (Scott-Brown's Otorhinolaryngology):
2. CT Scan - The Gold Standard
CT of the neck and chest is the best and most important imaging modality for retrosternal goiter. It should be performed without iodinated contrast whenever possible to avoid triggering thyrotoxicosis and to preserve the possibility of subsequent nuclear thyroid imaging (which cannot be performed for weeks after an iodine load).
CT findings that define retrosternal goiter:
| CT Feature | Significance |
|---|---|
| Continuity with cervical thyroid | Confirms thyroidal origin (key differentiating feature) |
| High attenuation on non-contrast CT | Due to intrinsic iodine content - thyroid tissue is naturally dense (80-100 HU vs soft tissue ~40 HU) |
| Heterogeneous texture | Colloid nodules, cystic degeneration, calcifications, fibrosis |
| Calcifications | Common in multinodular goiter - coarse, dense, "eggshell" or dystrophic |
| Tracheal deviation and/or compression | Present in essentially 100% of symptomatic cases |
| Esophageal displacement | Posterior compression |
| Vascular displacement | Great vessel displacement indicates significant bulk |
| Well-defined capsule | Usually retained in benign disease |
| Avid contrast enhancement | Thyroid tissue enhances brightly (when contrast used) |
| Inferior extension | Below thoracic inlet into anterior or posterior mediastinum |
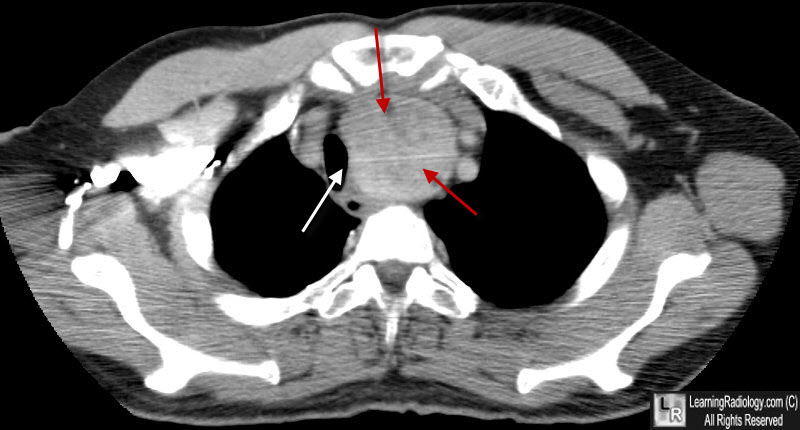
CT Images
Axial CT at the thoracic inlet level - showing the goiter mass occupying the anterior mediastinum with marked tracheal compression (white arrow) and displacement (red arrows). The mass is of heterogeneous density with internal calcifications, characteristic of multinodular goiter:
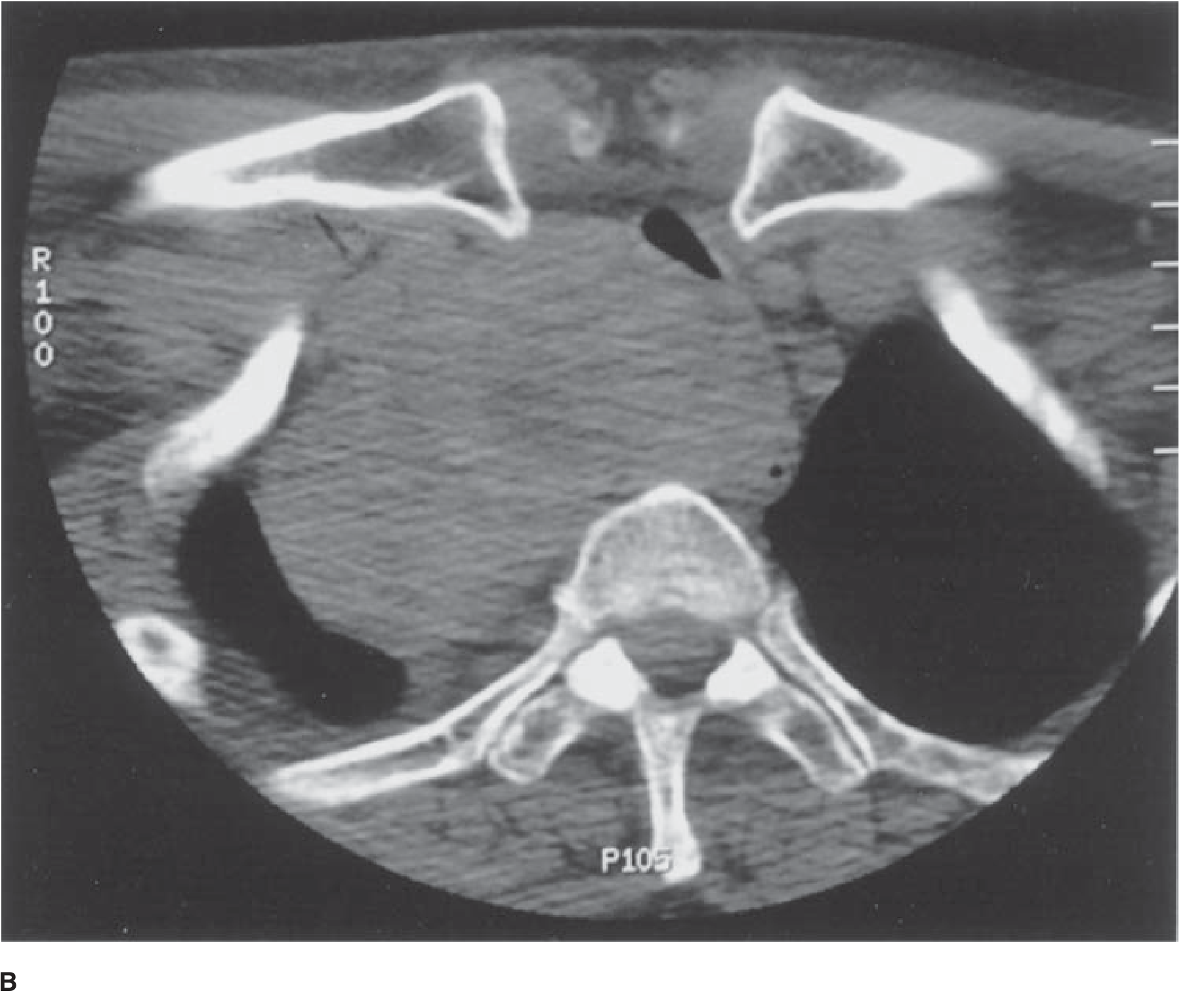
Axial CT through the upper chest (Radiopaedia case) - showing a large heterogeneous thyroid mass in the superior mediastinum, compressing and displacing mediastinal structures:

Textbook CT (Schwartz's Surgery, Fig. 38-13B) - Axial CT demonstrating retrosternal extension with tracheal deviation and compression from a large goiter:
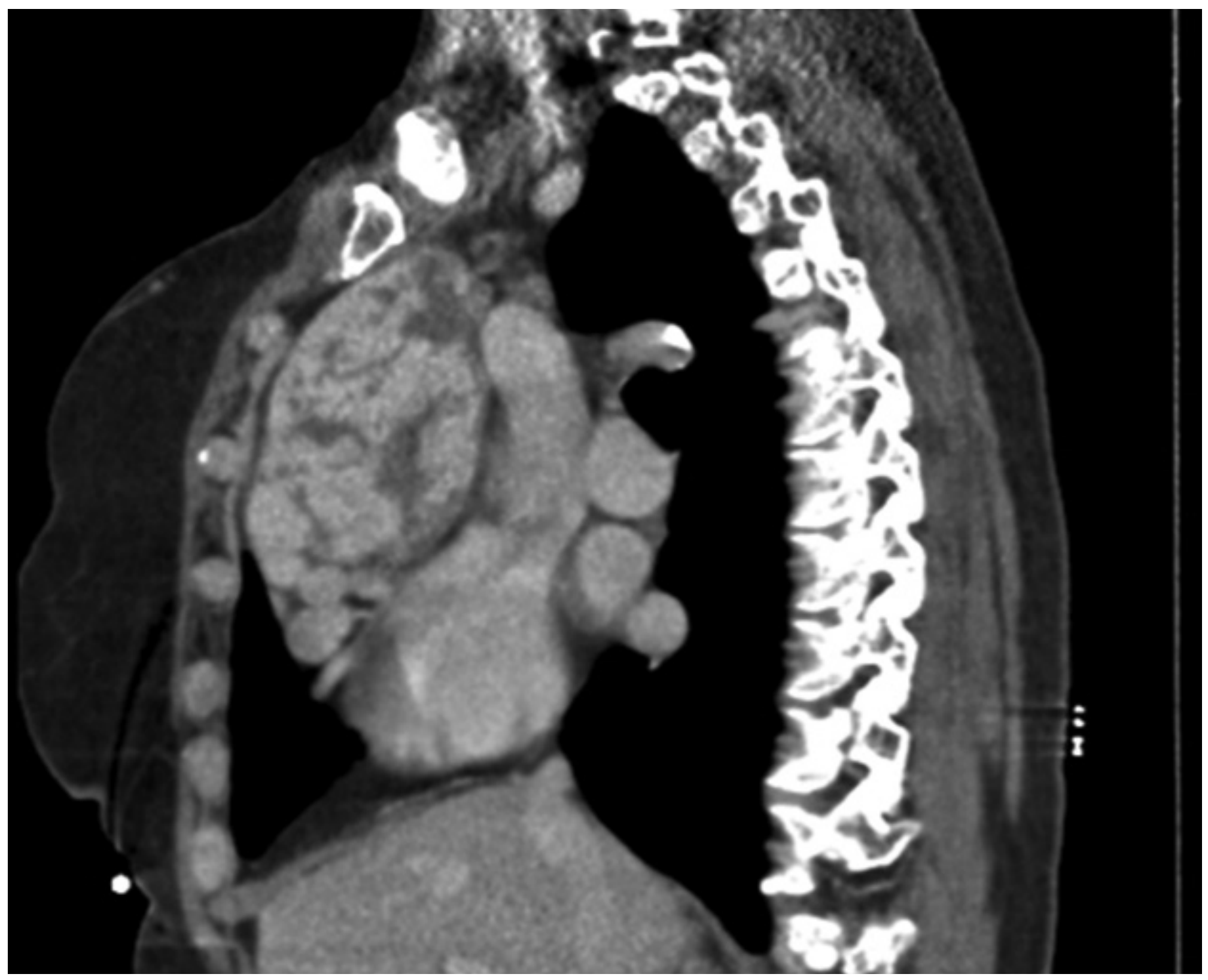
Sagittal/coronal CT reconstruction - demonstrating the full craniocaudal extent of a large multinodular goiter with retrosternal extension, showing the lobulated thyroid mass descending behind the sternum alongside the vertebral column:
CT-Based Classification (Surgical Planning)
CT findings that predict the need for a thoracic approach (sternotomy or thoracotomy) rather than a standard cervical incision:
| CT Finding | Implication |
|---|---|
| Extension below the aortic arch | Sternotomy likely required |
| Posterior mediastinal location | Lateral thoracotomy more likely needed |
| Right-sided primary intrathoracic goiter | Higher risk of needing thoracotomy |
| Evidence of extra-thyroid extension | Raises concern for malignancy |
| Malignancy risk up to 11% in intrathoracic extension |
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery, Vol. 1
3. Other Imaging Modalities
| Modality | Role |
|---|---|
| Ultrasound | Good for cervical component only; cannot visualize intrathoracic extension |
| MRI | Alternative to CT; excellent soft tissue detail; no radiation; longer acquisition time |
| Nuclear scintigraphy (¹²³I/⁹⁹ᵐTc) | Limited - intrathoracic goiters often show reduced iodine avidity; not used in euthyroid patients preoperatively |
| Barium swallow | May show esophageal compression; limited preoperative utility |
| Flow-volume loop spirometry | Functional assessment of airway obstruction; shows characteristic plateau pattern |
Investigations Summary
- TSH and FT4 - assess thyroid function
- Calcium + PTH - baseline before surgery
- CT neck + chest - mandatory if the distal extent of the goiter cannot be palpated
- Laryngoscopy - assess vocal cord mobility preoperatively
- FNAC - if malignancy suspected (up to 25% may have it pre-operatively)
Management
Surgery (total or near-total thyroidectomy) is the treatment of choice. Key operative principles:
- Cervical approach first - most (80-90%) can be removed via collar incision with neck extension
- Thyroid spoon / finger dissection - lateral to medial to deliver the retrosternal portion into the field
- Dividing the isthmus + taking down the superior pole - aids delivery of the substernal portion
- Sternotomy - required when goiter extends below the aortic arch or is too large for cervical delivery
- Thoracic surgery standby - always advisable for posterior mediastinal goiters
- Parathyroid and RLN identification - critical given distorted anatomy
Non-surgical options (radioiodine, levothyroxine suppression) are generally avoided due to poor iodine uptake and the mechanical risks of an enlarging intrathoracic mass.
Sources:
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery, Vol. 1 - Chapter 70
- Schwartz's Principles of Surgery, 11th ed. - Chapter 38
- Fischer's Mastery of Surgery, 8th ed. - Substernal Thyroid Extension
- Radiopaedia - Substernal Goitre
- PMC - CT classification of retrosternal goiter
This is a shared conversation. Sign in to Orris to start your own chat.