So I have pain in the medial aspect of knee when I, um, am lying down and my knee is little hyper-extended from neutral. So that time, non-weight-bearing while bending the knee pains a lot on the medial aspect. Whereas while walking and all, there's no pain, but my knee is in neutral position most of the times. A little hyper-extension in weight-bearing as well. Slight pain, but that is almost 50% less than non-weight-bearing.
Key Clinical Features
- Medial aspect knee pain
- Provoked by hyperextension, not neutral or flexion
- Non-weight-bearing + hyperextension = severe pain
- Weight-bearing + mild hyperextension = ~50% less pain
- Walking (neutral position) = no pain
Why Hyperextension Causes Medial Knee Pain
- The posterior horn of the medial meniscus is impinged/compressed between the femoral condyle and tibial plateau as the joint "opens up" posteriorly
- The posteromedial capsule and posterior oblique ligament (POL) are tensioned
- The semimembranosus tendon and its expansions (which insert posteromedially and contribute to the oblique popliteal ligament) are stressed
- The superficial MCL can be stressed if there is valgus combined with hyperextension
Most Likely Diagnoses
1. Posterior Horn Medial Meniscus Tear (Top Suspect)
"Common physical findings include pain with hyperflexion and with hyperextension, joint line tenderness, and an effusion."
2. Semimembranosus Tendinitis / Posteromedial Corner Irritation
"Semimembranosus tendinitis can be diagnosed by eliciting point tenderness over the posteromedial corner of the knee just distal to the joint line. The tendon usually is easily palpated. A provocative test of resisted internal tibial rotation of a knee flexed at 90 degrees also may pinpoint the pain."
3. Posteromedial Corner (PMC) Laxity/Injury
"Unrepaired severe posteromedial corner injuries may result in chronic pain, anteromedial rotatory instability, and genu recurvatum instability."
4. MCL Sprain (Lower on the List)
5. Pes Anserine Bursitis (Less Likely)
The Non-Weight-Bearing vs. Weight-Bearing Difference - Explained
- In weight-bearing, the ground reaction force compresses the joint and actually stabilizes the posterior horn and posteromedial structures - the tibia doesn't sag posteriorly
- In non-weight-bearing hyperextension (lying down, letting the leg dangle or actively extending), there is no axial load to stabilize, and the posterior structures (meniscal horn, capsule, tendons) bear the full tensile/compressive stress
- This pattern is more consistent with a tensile/structural problem (posterior horn meniscus, posteromedial capsule, semimembranosus) rather than an inflammatory/compressive problem like bursitis
What You Should Do
- Medial joint line tenderness - press just at the joint line on the medial side; if very tender, think meniscus
- McMurray's test - knee flex 90° + external rotation + extend; click or pain = medial meniscus
- Valgus stress test at 0° and 30° - for MCL integrity
- Recurvatum test - lift the leg by the toe; >10° recurvatum suggests posterior laxity
- Resisted internal tibial rotation at 90° flexion - if this reproduces posteromedial pain, think semimembranosus tendinitis
- MRI of the knee is the investigation of choice - it will show posterior horn meniscal tears (especially on sagittal and coronal sequences), semimembranosus tendon changes, and POL/posteromedial capsule integrity
Disclaimer: This is an educational analysis based on the pattern you described - not a clinical diagnosis. Please see a qualified clinician for proper examination and imaging.
Please retry what I asked you.
Step 1: Physical Examination (See a Clinician)
| Test | How it's Done | What a Positive Means |
|---|---|---|
| Medial joint line palpation | Thumb pressed directly on the medial joint line with knee slightly flexed | Sharp tenderness = meniscal pathology |
| McMurray's test | Knee flexed 90°, externally rotate the tibia, extend the knee - feel/hear for a click | Click or pain at medial line = medial meniscus tear |
| Apley compression test | Prone, knee at 90°, axial pressure + tibial rotation | Pain with compression = meniscus; pain with distraction = ligament |
| Valgus stress test at 0° and 30° | Sideways force applied to knee in full extension and at 30° flexion | Laxity/pain = MCL injury |
| Recurvatum test | Lift the leg by the toe with knee relaxed | >10° hyperextension compared to other side = posteromedial laxity |
| Resisted internal tibial rotation at 90° flexion | Patient tries to rotate tibia inward against resistance | Pain posteromedially = semimembranosus tendinitis |
Step 2: Imaging
-
It is the diagnostic standard for soft tissue knee pathology - meniscal tears, ligament injuries, cartilage damage
-
For your presentation (hyperextension-provoked medial pain), the radiologist should be asked specifically to evaluate: posterior horn of the medial meniscus, posteromedial capsule/posterior oblique ligament, and semimembranosus tendon
-
An X-ray first is reasonable to rule out bony causes (osteophytes, loose bodies, genu recurvatum deformity), but it will not show soft tissue
-
Swanson's Family Medicine Review states directly: "The diagnostic test of choice for a suspected medial meniscal tear with locking is an MRI scan."
Step 3: Immediate Self-Management (While You Wait)
- Avoid hyperextension - do not let the knee snap into that end-range position; keep a slight bend at rest and when standing
- RICE for flare-ups: Rest, Ice (15-20 min, not directly on skin), Compression, Elevation
- NSAIDs (e.g., ibuprofen 400 mg with food) for short-term pain relief if no contraindications - reduces local inflammation
- No high-impact activity that involves sudden pivoting, jumping, or forced extension until you have a diagnosis
- Gentle range-of-motion exercises staying within a pain-free arc (roughly 10°-90° flexion, not pushing into full extension)
Step 4: Definitive Management (Depends on Diagnosis)
- Conservative first (for degenerative/minor tears): physiotherapy focusing on quadriceps and hamstring strengthening, activity modification, NSAIDs. Campbell's Operative Orthopaedics notes: "Numerous studies have found no difference between arthroscopic meniscal debridement and nonoperative management as a first-line treatment strategy" - so surgery is not automatically required
- Arthroscopic surgery (partial meniscectomy or repair) if conservative management fails after 6-12 weeks, or if there are mechanical symptoms (locking, true giving way)
- Meniscal repair is preferred in younger patients in the vascular zone; partial meniscectomy for degenerative tears
- Conservative treatment almost always works: activity modification, physiotherapy (eccentric strengthening, soft tissue work), NSAIDs, corticosteroid injection if refractory
- Surgery (semitendinosus tendon transfer) is rare and only if all conservative measures fail
- Grade I-II: conservative (bracing, physiotherapy, 6-12 weeks)
- Grade III or combined injuries: orthopaedic surgical referral
Who to See
- First visit: Sports medicine physician or orthopaedic surgeon - they can do all the physical tests above and order imaging in one visit
- After diagnosis: If soft tissue/rehabilitation, a sports physiotherapist is your primary manager
- If imaging shows significant meniscal or ligamentous injury: Orthopaedic surgeon for surgical discussion
Bottom line for you right now: Avoid hyperextension, use ice and ibuprofen for flare-ups, and get a clinical examination + knee MRI. The key question the MRI will answer is whether the posterior horn of the medial meniscus is torn - that's the most likely structural cause of your specific pain pattern.
Disclaimer: This is educational guidance, not a substitute for in-person clinical assessment.
orris logo New Chat Recent Medial knee pain with hyperextension Jul 1, 2026 Protein Powder Recommendations Egg-Based Diet for Kidney Stone Management Kidney Stone Management and Prevention Jun 28, 2026 Right Axilla Throbbing Pain Jun 27, 2026 Intermittent Right Chest Pain Cerebral Palsy GMFCS Level 3 Child Dr. Himani Dalmia Manchanda So I have pain in the medial aspect of knee when I, um, am lying down and my knee is little hyper-extended from neutral. So that time, non-weight-bearing while bending the knee pains a lot on the medial aspect. Whereas while walking and all, there's no pain, but my knee is in neutral position most of the times. A little hyper-extension in weight-bearing as well. Slight pain, but that is almost 50% less than non-weight-bearing.
- Your presentation (medial knee pain provoked specifically by hyperextension, worse non-weight-bearing than weight-bearing, no pain walking in neutral) points most strongly to posterior horn medial meniscus pathology or posteromedial corner/semimembranosus involvement
- The action plan was: clinical examination with specific provocation tests → knee MRI → management based on findings
- Short-term: avoid hyperextension, ice/NSAIDs for flare-ups, no high-impact pivoting/jumping
- About the physical tests you can check at home before seeing a doctor
- About what to expect from an MRI appointment
- About exercises that are safe vs. ones to avoid right now
- About any other symptom you want to add to the picture
The rotation is not painful
-
Meniscal tear - McMurray's and Apley tests both rely on rotation to provoke pain. If tibial rotation in any direction doesn't hurt, a meniscal tear becomes significantly less likely. Meniscal tears typically hurt with the combination of compression + rotation as the torn fragment gets caught.
-
Semimembranosus tendinitis - the classic provocative test is resisted internal tibial rotation. If rotation is painless, this also moves down the list.
-
Posterior Oblique Ligament (POL) / Posteromedial Capsule - this is the structure most directly tensioned in hyperextension on the medial side. It is a static stabilizer against hyperextension and is not particularly stressed by rotation alone.
-
Deep MCL / Medial capsular ligament - the posterior third of the deep MCL blends with the posteromedial capsule and becomes taut in hyperextension. Not primarily a rotational restraint.
-
Medial patellofemoral or medial retinacular structures - less likely given the medial joint line location you described.
- Pain on hyperextension ✓
- Medial side ✓
- Non-weight-bearing worse than weight-bearing ✓
- Rotation painless ✓ (capsule/ligament, not meniscus or tendon)
- Right at the joint line = more intra-articular (still possibly meniscal root, but less likely given no rotational pain)
- Just below = pes anserine area
- Just behind the joint line, posteromedially = POL/capsule
One more thing. Vulgar stress is extremely painful. Valgus, not vulgar.
The Valgus Stress Finding is the Key
"MCL injury occurs as a result of valgus stress to the knee. Pain and instability with valgus stress testing at 30 degrees of flexion (and not in full extension) are diagnostic."
| Finding | Interpretation |
|---|---|
| Medial pain on hyperextension | MCL is tensioned at end-range extension |
| Valgus stress extremely painful | MCL injury - primary finding |
| Rotation not painful | Rules out meniscus, semimembranosus |
| Walking in neutral = no pain | MCL is not stressed in neutral gait |
| Non-weight-bearing worse | Unguarded valgus moment without ground stabilization |
Grading Your MCL Injury
- Grade I (3-5 mm opening on valgus stress): Microscopic tear, painful but stable. Tender over the ligament, no laxity.
- Grade II (6-10 mm opening): Partial tear. Painful with valgus stress, some laxity but a firm endpoint still present.
- Grade III (>10 mm opening): Complete tear. Significant laxity, often less painful than Grade II because fibers are fully disrupted.
- Pain/laxity at 30° but not full extension = isolated MCL injury
- Pain/laxity in full extension too = likely combined MCL + ACL or PCL injury
Management Algorithm
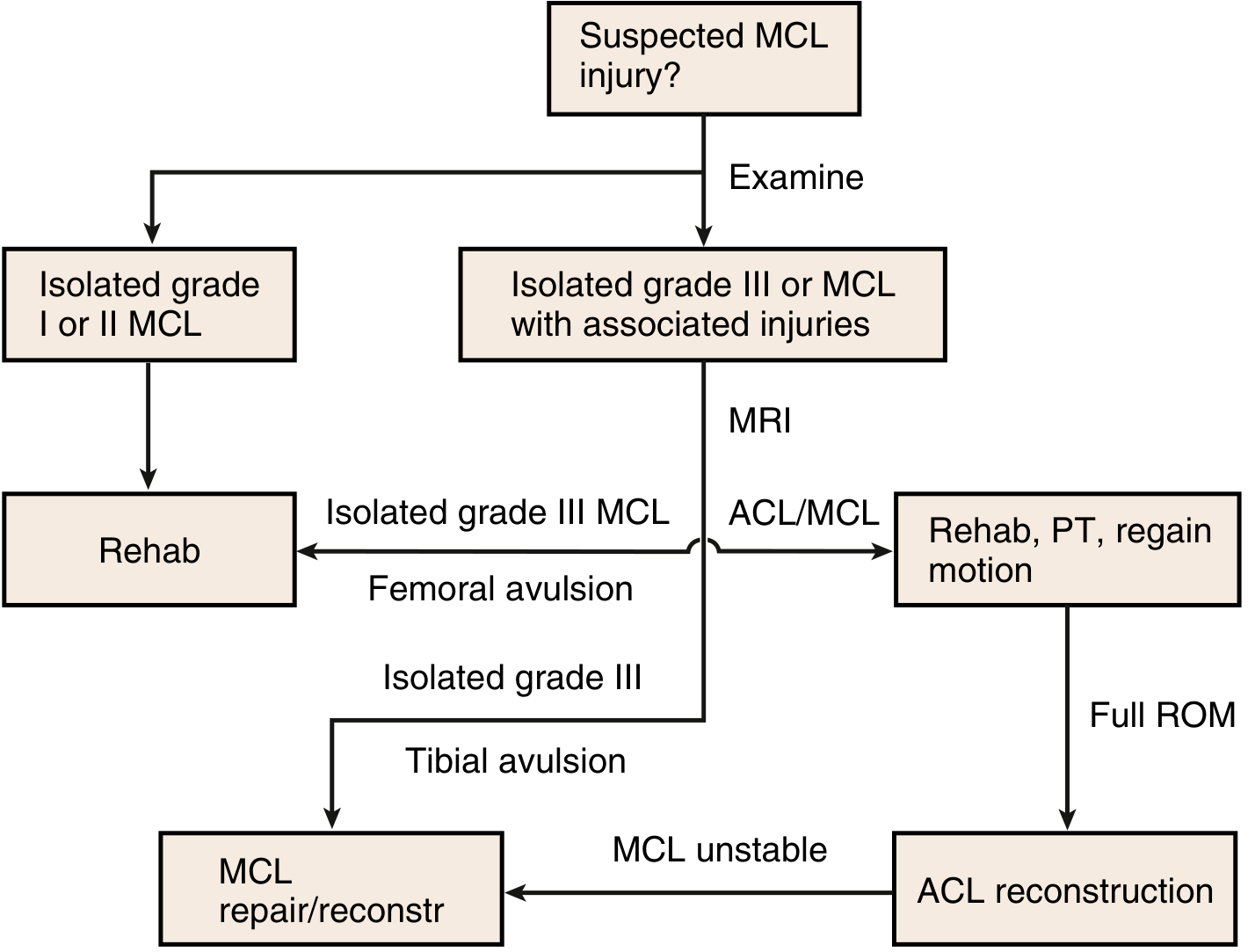
- Grade I or II isolated MCL: Rehabilitation - no surgery needed. Hinged knee brace + physiotherapy. Highly successful.
- Grade III isolated MCL: Still usually treated with rehab first, but MRI is needed to rule out associated injuries
- MCL + ACL/cruciate injury: MRI first, then rehab to regain motion, then consider ACL reconstruction. If MCL remains unstable after ACL reconstruction, then MCL repair/reconstruction.
What You Should Do Right Now
- See an orthopaedic surgeon or sports medicine physician - the grading of your MCL injury on examination (how much laxity is there at 30°? at 0°?) determines everything
- MRI of the knee - to confirm MCL grade, locate the tear (femoral vs. tibial end - femoral origin tears are most common), and rule out ACL/PCL involvement given your hyperextension symptom
- In the meantime:
- A hinged knee brace (available at a pharmacy/medical store) will protect the MCL immediately - it prevents valgus and hyperextension stress while allowing normal flexion-extension
- Avoid any activity that loads the knee in valgus (sitting cross-legged, squatting with knees caving in)
- Ice + NSAIDs for pain/swelling
Disclaimer: This is educational analysis. Please see a clinician for examination and imaging to confirm the diagnosis and grade.