Psoas abscess culture has come positive for TB. What are the precautions to be taken by the patient and caregiver.? Does this spread? Is the patient at serious risk? What are the home care measures to be taken?
Reading File
Finding Sources
Finding Sources
Searching the Web
psoas abscess tuberculosis TB precautions infection control home care management
Searching PubMed
"psoas abscess" AND tuberculosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I now have enough comprehensive information to give a thorough, well-sourced answer. Let me compile it.
TB Psoas Abscess: Your Complete Guide
What Is This Exactly?
A psoas abscess culture positive for TB means Mycobacterium tuberculosis has spread - usually from a nearby infected spine (Pott's disease) - into the iliopsoas muscle, forming a pus collection in the retroperitoneum. This is extrapulmonary tuberculosis (EPTB), which carries specific implications for infectiousness and management. - Bailey and Love's Short Practice of Surgery, 28th Ed.
1. Does It Spread? (The Most Important Question First)
The short answer: the psoas abscess itself is NOT directly contagious to caregivers or household contacts.
Here is why this matters:
- TB spreads almost exclusively via the airborne route - tiny droplet nuclei expelled when a person with pulmonary or laryngeal TB coughs, sneezes, or shouts. - Wisconsin Dept. of Health
- A psoas abscess is a closed, deep tissue collection. The TB bacteria are contained within the muscle and pus. They are not being expelled into the air.
- Extrapulmonary TB (bones, muscles, lymph nodes, abdominal organs) is generally considered non-infectious to others, unlike pulmonary TB. - Miller's Anesthesia, 10th Ed.
- However, the psoas abscess is almost always caused by spread from a spinal focus (Pott's disease). The treating physician must rule out concurrent pulmonary TB with a chest X-ray and sputum test. If pulmonary TB is also present, then airborne precautions ARE needed.
Key rule: If there is no active pulmonary TB, strict isolation is NOT required. If pulmonary TB coexists, full airborne precautions apply.
2. Is the Patient at Serious Risk?
Yes - this is a serious condition, but it is very treatable if managed properly. Risks include:
- The abscess itself: Pain, fever, back pain, and a swelling that may track down into the groin. Untreated, it can cause lumbar plexopathy (nerve damage), femoral neuropathy, hip flexion deformity, or sepsis. - Bradley and Daroff's Neurology in Clinical Practice
- The underlying spinal disease (Pott's disease): Can cause vertebral collapse, spinal cord compression, and paralysis if not treated.
- Systemic TB: Spread to other organs (miliary TB, meningitis) is possible, especially in immunocompromised patients.
- Complications of treatment: Anti-TB drugs have side effects including liver toxicity (monitor LFTs), optic neuritis (ethambutol), peripheral neuropathy (isoniazid).
Prognosis is good with proper treatment - most patients respond well to a full anti-TB drug course combined with drainage.
3. Treatment Outline
Treatment of extrapulmonary TB (including psoas TB) follows a standard protocol: - Brenner and Rector's The Kidney, 2-Vol Set | Bailey and Love's
| Phase | Drugs | Duration |
|---|---|---|
| Intensive phase | Isoniazid + Rifampicin + Pyrazinamide + Ethambutol (4 drugs) | 2 months |
| Continuation phase | Isoniazid + Rifampicin (2 drugs) | 4-10 months |
| Total for musculoskeletal/spinal TB | - | 9-18 months (longer than pulmonary TB) |
- The abscess itself usually requires CT-guided percutaneous drainage in addition to antibiotics. Surgery is reserved for failures.
- Directly Observed Therapy (DOT) is strongly recommended - a health worker supervises each dose to ensure compliance and prevent drug resistance.
4. Precautions for the Patient
Medication Compliance (Most Critical)
- Take ALL anti-TB medications every single day without missing doses, even after feeling better. Incomplete treatment is the leading cause of drug-resistant TB (MDR-TB).
- Do not stop medicines on your own even if side effects occur - report to your doctor.
- Store medicines correctly (away from heat, moisture, direct sunlight).
Activity and Rest
- Avoid heavy physical exertion, especially movements that strain the back or hip.
- Complete bed rest is not required, but strenuous activity should wait until fever resolves and the abscess is draining/draining has been done.
- If Pott's disease (spinal TB) is confirmed, follow the spine specialist's instructions about bracing and mobility strictly.
Nutrition
- Eat a high-protein, calorie-rich diet (eggs, lentils, milk, fish, meat, nuts) - TB is a catabolic disease and malnutrition worsens outcomes.
- Avoid alcohol completely - it worsens isoniazid-related liver toxicity.
- Take Vitamin B6 (Pyridoxine) 25-50 mg/day alongside isoniazid to prevent peripheral neuropathy (usually prescribed by the doctor).
Monitoring and Follow-up
- Regular liver function tests (LFTs), especially in the first 2 months.
- Eye check if on ethambutol (report any blurring or color changes immediately).
- Scheduled follow-up with the treating physician and/or TB clinic every 2-4 weeks initially.
- Report to the doctor immediately if: fever worsens, new swelling appears, back pain increases suddenly, weakness in legs occurs (sign of cord compression), or jaundice develops.
5. Precautions for the Caregiver
If NO Pulmonary TB (Most Likely Scenario for Psoas TB)
- No special isolation or masking is required for day-to-day contact.
- You can share meals, the same room, and provide physical care without risk from this abscess.
- Wear gloves when handling wound dressings or drainage from the abscess - dispose of soiled materials in a sealed bag.
- Wash hands thoroughly with soap after dressing changes.
If Pulmonary TB Is Also Confirmed
- The patient should sleep in a separate, well-ventilated room.
- Caregivers should wear an N95 respirator (not a regular surgical mask) when in close contact, especially during coughing episodes.
- Open windows frequently to improve natural ventilation - fresh air dilutes any airborne particles significantly.
- Avoid enclosed, poorly ventilated spaces together (car with windows up, small rooms).
- All household contacts should be tested for TB infection (Tuberculin Skin Test or IGRA blood test) - CDC household contact testing guidance.
General Caregiver Measures
- Do not allow visitors who are immunocompromised (HIV+, on chemotherapy, elderly with diabetes) until the doctor confirms non-infectiousness.
- Take the patient to ALL medical appointments - missed visits are the number one cause of treatment failure.
- Psychological support is important - TB treatment is long (9-18 months) and depression/fatigue during treatment is common.
6. Home Care Measures
| Area | What to Do |
|---|---|
| Wound/drain care | Keep drain site clean and dry. Change dressings as instructed. Gloves always. |
| Ventilation | Keep rooms well-ventilated with open windows. Fresh air is protective. |
| Nutrition | High-protein meals 3x/day. Vitamin B6 supplement. No alcohol. |
| Medication | Use a pill organizer or DOT schedule. Never skip a dose. |
| Hygiene | Dedicated towels, pillow covers. Regular washing in hot water is sufficient. No need to discard or isolate utensils. |
| Exercise | Gentle walking when comfortable. No heavy lifting or twisting at the waist. |
| Mental health | Stay connected socially (TB abscess patients are NOT contagious via normal contact). Watch for signs of depression during long treatment. |
| Red flag signs | Sudden back pain increase, leg weakness, high fever, yellowing of skin/eyes, blurred vision - go to ER immediately. |
Summary
| Question | Answer |
|---|---|
| Does it spread? | Psoas TB abscess does NOT spread to caregivers in normal contact. Only pulmonary TB is contagious. |
| Is the patient at serious risk? | Yes - serious but very treatable. Main risks are spinal complications and drug side effects. |
| Isolation needed? | Only if pulmonary TB is also present. Otherwise no. |
| Treatment duration? | 9-18 months of anti-TB drugs + drainage of abscess. |
| Most important action? | Never miss a dose of anti-TB medication. |
The most important step is to have the doctor confirm whether there is concurrent pulmonary TB. If the chest X-ray and sputum tests are negative, the patient and family can live normally - precautions relate to wound care and drug compliance, not airborne isolation. - Goldman-Cecil Medicine, International Ed.
Is there a possibility that the patient doesn't have any history of TB, but then she gets psoas abscess tb positive and no pulmonary involvement or discomfort
Finding Sources
Finding Sources
Searching the Web
psoas abscess TB positive no pulmonary involvement no history of tuberculosis primary extrapulmonary TB
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Excellent - that diagram is perfect. Here is the complete, well-sourced answer:
Yes - This Is Entirely Possible and Well Documented
A patient can absolutely have a TB-positive psoas abscess with no prior TB history and no pulmonary symptoms. This is not a rare curiosity - it has a clear biological explanation and published case reports confirm it. Here is exactly how and why it happens.
The Biological Mechanism: How TB Gets to the Psoas Without Lung Disease
This diagram from Robbins Pathology explains the whole story visually:
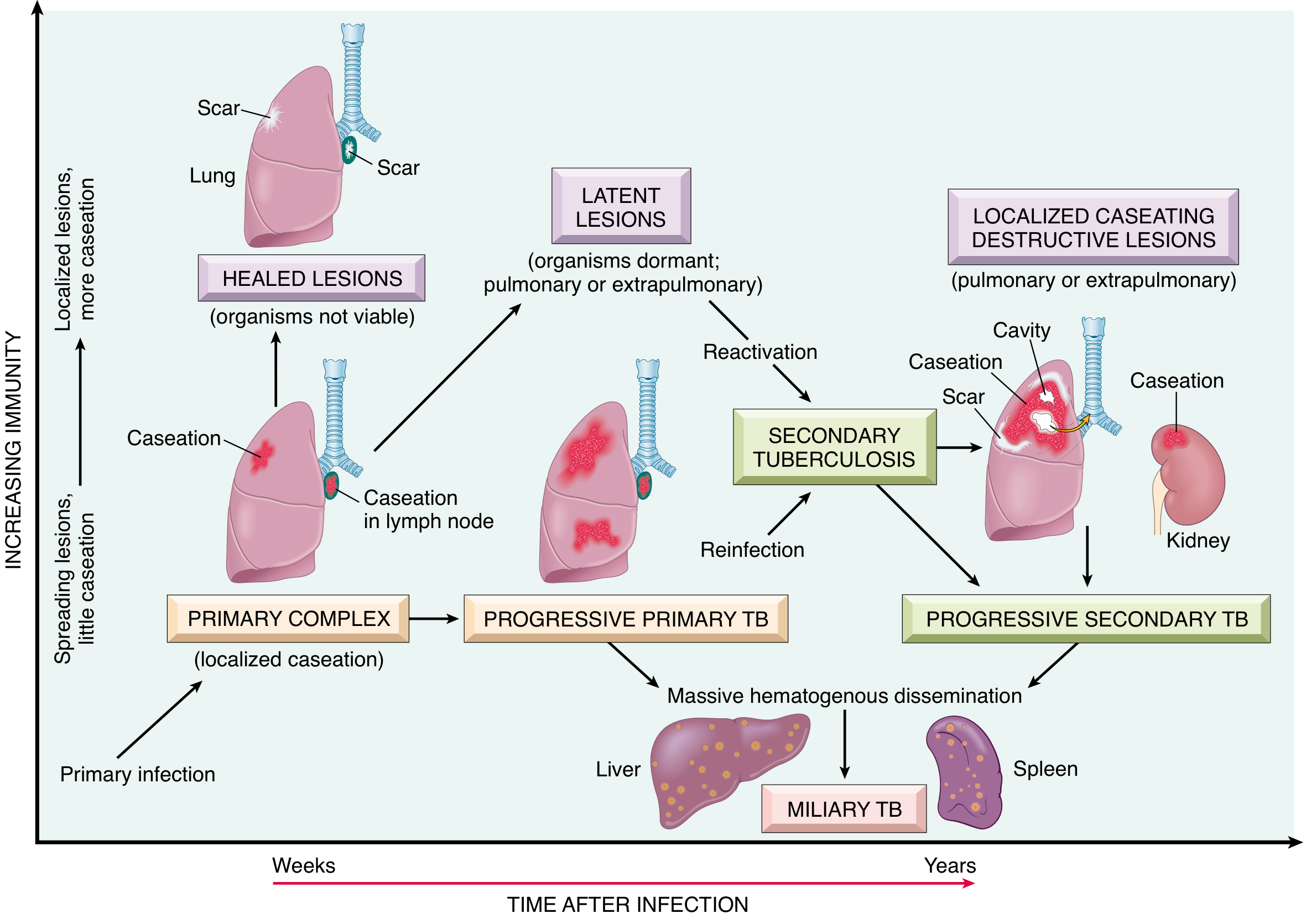
Step 1: The Silent Primary Infection (Often in Childhood)
When a person first inhales TB bacilli, the bacteria implant in the lung and form a small focus called the Ghon complex (lung lesion + hilar lymph node). In approximately 95% of people, the immune system successfully contains this - the Ghon complex calcifies and heals, and the person has no symptoms whatsoever. They do not know they were ever infected. - Robbins Pathologic Basis of Disease
Crucially, during those first few weeks of primary infection, bacteria spread via the bloodstream (hematogenous dissemination) to other organs - bones, kidneys, lymph nodes, liver, spleen. The immune system contains these seeded sites too, leaving microscopic dormant foci scattered throughout the body. The person remains completely well.
Step 2: Decades of Dormancy (Latent TB)
The bacteria are alive but dormant - walled off inside granulomas. The person has no symptoms, a normal chest X-ray, and does not know they carry TB. This latent state can persist for months to decades. - Robbins
Step 3: Reactivation at the Extrapulmonary Site
Years or decades later, if the immune system is weakened even mildly - by stress, poor nutrition, diabetes, aging, steroids, pregnancy, subclinical HIV, or sometimes no identifiable cause - the dormant bacteria at the extrapulmonary site reactivate. The psoas/spine is a classic site for this because:
- Bone and muscle foci seeded during primary infection are slow to reactivate
- They can form caseating granulomas and eventually a cold abscess over months to years
- The lung focus may have completely healed and calcified, leaving no active pulmonary disease
This is why the patient has:
- No history of TB (primary infection was silent)
- No pulmonary symptoms (lung healed decades ago)
- Active TB in the psoas (reactivation of a silently seeded focus)
What the Literature Says
Published case reports confirm this pattern precisely:
- A 2022 case report (Springer Nature) describes primary psoas TB abscess with iliac bone involvement - no active TB elsewhere at diagnosis, confirmed by negative pulmonary workup.
- A 2022 PMC case reports a young patient with no predisposing illness, normal chest and spine imaging, where the only positive specimen was TB-PCR from the psoas pus - classified as primary psoas abscess.
- A 2025 PMC bilateral psoas TB case involved a 22-year-old with no medical history, persistent back pain for 18 months, bilateral psoas abscesses - all three sputum samples negative for TB, confirming no pulmonary involvement. Successfully treated with standard 6-month anti-TB therapy.
Two Possible Explanations in This Patient's Case
| Scenario | Explanation |
|---|---|
| Latent TB reactivation (more common) | Silent primary infection in the past (possibly childhood, forgotten exposure). Bacteria seeded the spine/psoas hematogenously and lay dormant. Reactivated now - perhaps triggered by a mild immune dip. |
| Primary psoas TB (less common but documented) | TB directly infected the psoas/iliac area without a clear prior pulmonary phase - via lymphatic seeding from gut or lymph nodes, or direct hematogenous spread during an otherwise contained primary infection. |
In both cases, the lung is not the active site and the patient is not contagious via the airborne route.
What This Means Practically
-
This does NOT mean the patient is unusual or lying about no prior TB history. Silent primary TB in childhood is extremely common in TB-endemic countries (India, Southeast Asia, Africa, etc.).
-
IGRA (QuantiFERON) or Mantoux test will likely be positive, confirming past exposure - but this does not change management.
-
Chest X-ray may show an old calcified Ghon complex - a small calcified nodule, which is the healed scar of the original silent infection. This is not active disease.
-
Sputum tests will be negative (as confirmed in the case reports above) - the patient is not exhaling TB bacilli.
-
The treatment is exactly the same as any extrapulmonary TB: standard 4-drug regimen (RHEZ) for 2 months followed by 2-drug continuation for 4-10 months, plus abscess drainage.
-
All close household contacts should still be tested (IGRA or Mantoux) - not because she is currently infectious, but to identify others who may have been exposed to the same original TB source in the past and may carry latent TB themselves.
Bottom Line
This clinical picture - TB psoas abscess, no pulmonary disease, no prior history - is a textbook example of latent TB reactivation at an extrapulmonary site seeded silently during an earlier, unrecognized primary infection. It is well-recognized in TB-endemic regions. The patient should be reassured that she is not contagious to her family, and the focus should be on completing the full course of anti-TB treatment without interruption. - Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.