I now have all the information needed for a thorough, well-referenced answer. Let me compile the complete response.
Carpal Tunnel Syndrome - Complete Anatomical Analysis
a) What is Carpal Tunnel Syndrome?
Carpal tunnel syndrome (CTS) is the most common entrapment neuropathy, caused by compression of the median nerve within the carpal tunnel.
The carpal tunnel is a fibro-osseous canal at the wrist formed by:
- Floor and sides: the concave carpal arch (formed by the carpal bones - pisiform and hook of hamate medially; tubercles of the scaphoid and trapezium laterally)
- Roof: the flexor retinaculum (transverse carpal ligament), a thick connective tissue band bridging the medial and lateral walls
When pressure within this fixed-volume tunnel rises, venous congestion produces nerve edema and anoxic damage to the capillary endothelium of the median nerve, causing the characteristic symptoms.
Causes/associations include:
- Occupational repetitive use (e.g., typists, assembly workers)
- Rheumatoid arthritis (tenosynovitis)
- Pregnancy (fluid retention)
- Hypothyroidism, diabetes mellitus, acromegaly
- Amyloidosis
- Ganglion cysts from carpal joints
"Carpal tunnel syndrome is an entrapment syndrome caused by pressure on the median nerve within the carpal tunnel... Increased pressure in the carpal tunnel is thought to cause venous congestion that produces nerve edema and anoxic damage to the capillary endothelium of the median nerve itself." - Gray's Anatomy for Students
b) Structures Passing Through the Carpal Tunnel
The carpal tunnel transmits 10 structures:
| # | Structure |
|---|
| 1 | Median nerve (anterior to tendons, most superficial) |
| 2 | Tendon of flexor pollicis longus (in its own synovial sheath) |
| 3-6 | Four tendons of flexor digitorum superficialis (in a common synovial sheath) |
| 7-10 | Four tendons of flexor digitorum profundus (in the same common synovial sheath) |
Structures NOT in the carpal tunnel (pass anterior to the flexor retinaculum):
- Ulnar nerve and ulnar artery (pass through Guyon's canal)
- Palmaris longus tendon
- Palmar cutaneous branch of the median nerve (exits the median nerve just proximal to the retinaculum - this is why palm sensation is preserved in CTS)
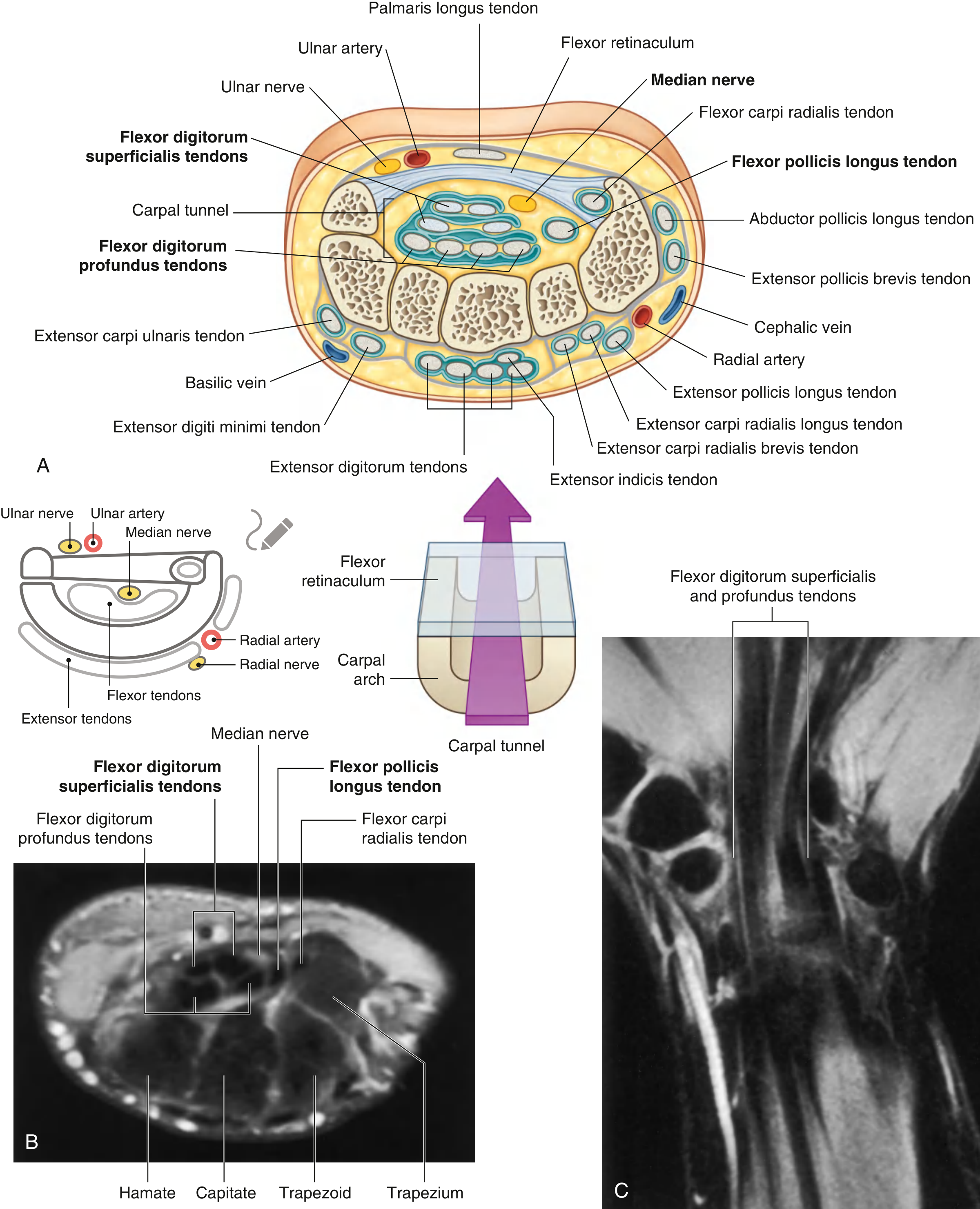
Diagram of Carpal Tunnel Contents
Below is a cross-sectional diagram from Gray's Anatomy for Students showing all structures at the level of the carpal tunnel:
Fig. 7.98 Carpal Tunnel. (A) Cross-sectional diagram showing structures and relations. (B) Axial MRI of a normal wrist. (C) Coronal MRI of a normal wrist. - Gray's Anatomy for Students
Key points from the diagram:
- The median nerve lies most anteriorly (just deep to the flexor retinaculum)
- Flexor digitorum superficialis tendons form the middle layer (4 tendons, in pairs)
- Flexor digitorum profundus tendons lie posteriorly (4 tendons)
- Flexor pollicis longus lies on the radial (lateral) side in its own sheath
- The ulnar nerve and artery lie medial but outside the tunnel (in Guyon's canal)
c) Motor and Sensory Distribution of the Median Nerve in the Hand
After passing through the carpal tunnel, the median nerve divides into two main branches:
Motor Distribution
The median nerve innervates the "LOAF" muscles in the hand:
| Muscle Group | Specific Muscles | Function |
|---|
| Thenar muscles (via Recurrent branch) | Abductor pollicis brevis | Abduction of thumb |
| Opponens pollicis | Opposition of thumb |
| Flexor pollicis brevis (superficial head) | Flexion of thumb MCP joint |
| Lumbricals | Lateral two lumbrical muscles (1st and 2nd) | Flex MCPs, extend IPs of index/middle fingers |
The recurrent branch of the median nerve originates from the lateral side of the main trunk near the distal margin of the flexor retinaculum and curves back proximally to supply the thenar muscles. This branch is the key to thenar muscle function and thumb opposition.
Sensory Distribution
The median nerve provides cutaneous sensation to:
Palmar surface:
- Thumb (palmar surface)
- Index finger (palmar surface)
- Middle finger (palmar surface)
- Lateral (radial) half of the ring finger (palmar surface)
Dorsal surface:
- Dorsal aspects of the distal phalanges (nail beds) of the same lateral 3½ digits
Important exception - Palmar cutaneous branch:
- Arises from the median nerve proximal to the flexor retinaculum
- Passes superficial to (not through) the carpal tunnel
- Supplies skin over the thenar eminence and proximal central palm
- Therefore, palm sensation is SPARED in carpal tunnel syndrome
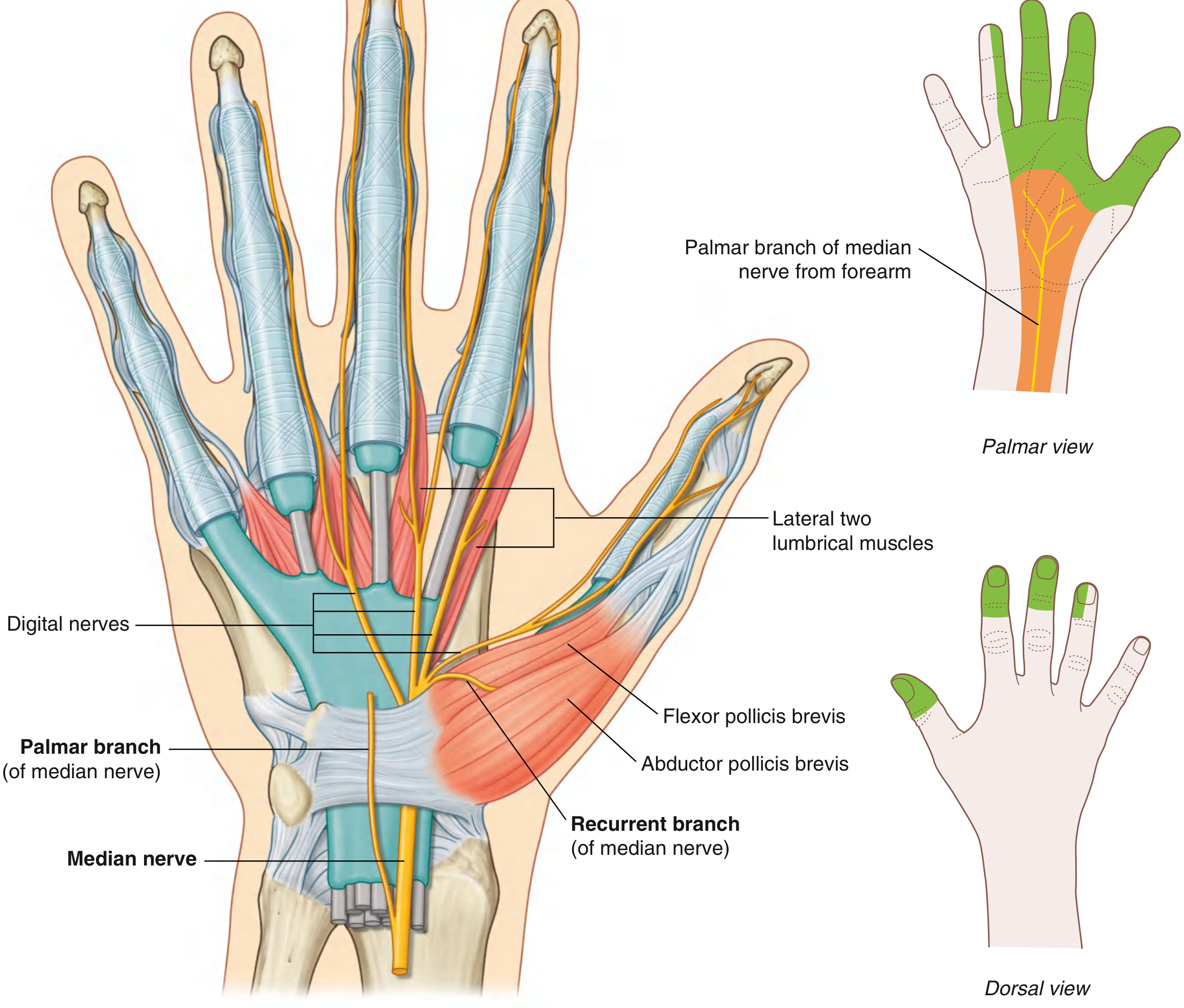
Median Nerve Distribution Diagram
Fig. 7.115 Median Nerve in the Hand - showing the recurrent branch to thenar muscles, digital nerves, lateral two lumbricals, palmar branch, and sensory maps (palmar and dorsal views in green). - Gray's Anatomy for Students
d) Correlation of Symptoms with Anatomical Structures
| Symptom in the Case | Anatomical Explanation |
|---|
| Tingling and pain in thumb, index, middle, and lateral ring finger | These are the territories of the palmar digital branches of the median nerve. Compression of the median nerve in the carpal tunnel causes paresthesias (tingling/pins-and-needles) in exactly these four digits. |
| Sensation to the palm is NOT affected | The palmar cutaneous branch of the median nerve arises proximal to the flexor retinaculum and passes superficial to it, so it is NOT compressed within the tunnel. |
| Weakness in grasping and holding instruments | The lateral two lumbricals (median nerve) contribute to precision grip. Also, the thenar muscles are affected, compromising thumb opposition - essential for power grip and grasping. |
| Weakness of thumb movements | Loss of power in the thenar muscles (abductor pollicis brevis, opponens pollicis, flexor pollicis brevis), all supplied by the recurrent branch of the median nerve. The abductor pollicis brevis is the most sensitive indicator and shows early denervation in CTS. |
| Impaired light touch and pin-prick in thumb, index, middle, and lateral ring finger | Compression of the median nerve's sensory fibers within the tunnel → impaired sensation in its distribution (lateral 3½ digits). The sensory fibers traveling in the digital branches are affected. |
| Tapping/pressure over flexor retinaculum produces tingling (Tinel's sign) | The median nerve lies directly posterior to the flexor retinaculum. Tapping (percussion) over an injured or compressed nerve generates an ectopic impulse that produces tingling (paresthesias) in the nerve's distribution - this is the Tinel's sign, positive in CTS. |
| Occupational link (typist - repetitive wrist use) | Repetitive wrist flexion/extension increases pressure within the fixed-volume carpal tunnel, causing intermittent compression of the median nerve. CTS is recognized as an occupational hazard of repetitive stress jobs. |
Summary Diagram of the Pathophysiology
Repetitive wrist use (typing)
↓
↑ Pressure in carpal tunnel
↓
Venous congestion → Nerve edema → Anoxic damage to median nerve
↓
Sensory fibers (digital branches) → Tingling/pain in lateral 3½ digits
Motor fibers (recurrent branch) → Weakness of thenar muscles + lumbricals
Palmar cutaneous branch (above retinaculum) → Palm sensation PRESERVED
↓
Tinel's sign: Tapping over flexor retinaculum → tingling in median distribution
Sources:
- Gray's Anatomy for Students (Sections 7.98, 7.115, pp. 919-939)
- Bradley and Daroff's Neurology in Clinical Practice (p. 549)
- Firestein & Kelley's Textbook of Rheumatology
- Imaging Anatomy: Bones, Joints, Vessels and Nerves