Thyroid hormones and functions
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of thyroid hormones and their functions, drawn from Guyton & Hall Textbook of Medical Physiology and Costanzo Physiology.
Thyroid Hormones: Synthesis, Mechanism, and Functions
The Two Thyroid Hormones
The thyroid gland produces two main iodinated hormones:
| Hormone | Full Name | Iodine Atoms | Activity |
|---|---|---|---|
| T4 (Thyroxine) | Tetraiodothyronine | 4 | Prohormone - less active |
| T3 | Triiodothyronine | 3 | Principal active hormone |
T4 is secreted in far greater amounts, but is much less active. In target tissues, 5'-iodinase converts T4 to T3, which is the biologically active form. T4 can also be converted to reverse T3 (rT3), which is physiologically inactive.
Synthesis of Thyroid Hormones
The synthesis occurs in the follicular epithelial cells of the thyroid gland. The follicles store hormones as colloid in their lumen until TSH stimulates secretion. The key steps are:
- Thyroglobulin (TG) synthesis - Follicular cells synthesize TG (a glycoprotein, MW ~335,000), which contains ~70 tyrosine residues. TG is extruded into the follicular lumen.
- Iodide trapping - I⁻ is actively transported into follicular cells via the Na⁺/I⁻ symporter (NIS) against chemical and electrical gradients.
- Oxidation of iodide - Thyroid peroxidase (TPO) and H₂O₂ oxidize I⁻ to active iodine (I₂), which enters the colloid.
- Organification - Oxidized iodine binds tyrosine residues on TG, forming monoiodotyrosine (MIT) and diiodotyrosine (DIT).
- Coupling - DIT + DIT → T4; DIT + MIT → T3.
- Secretion - When stimulated by TSH, follicular cells endocytose TG from the colloid, lysosomes cleave T3/T4 from TG, and free hormones are released into the bloodstream.
Once in the blood, >99% of thyroid hormones are bound to carrier proteins (thyroxine-binding globulin, albumin, transthyretin). Only the free fraction is biologically active.
Mechanism of Action
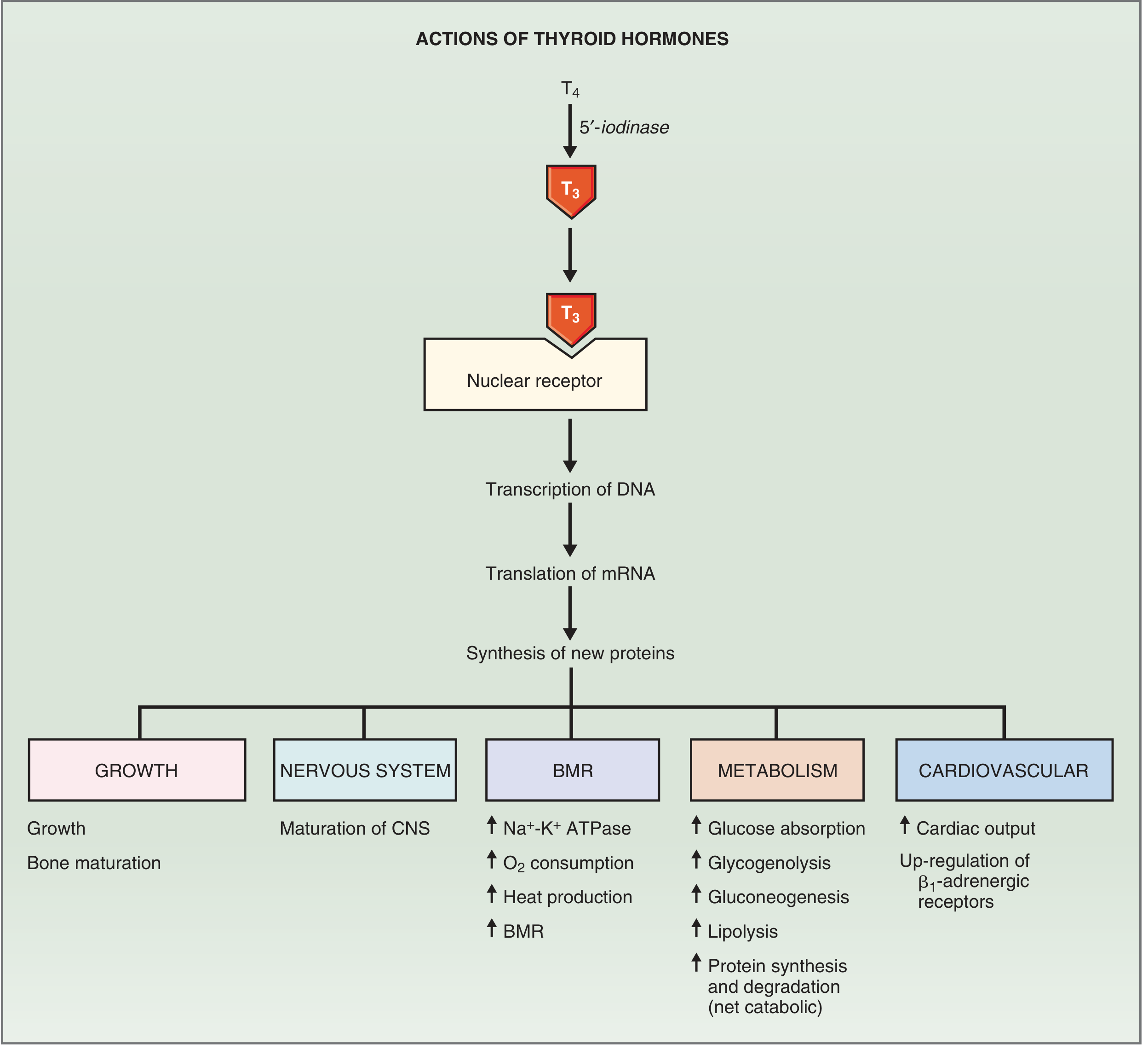
Fig. 9.20 from Costanzo Physiology - Mechanism of action of thyroid hormones
Genomic (primary) mechanism:
- T4 enters target cells and is converted to T3 by 5'-iodinase
- T3 enters the nucleus and binds a nuclear thyroid hormone receptor, which forms a heterodimer with the Retinoid X Receptor (RXR)
- This T3-receptor complex binds to thyroid hormone response elements (TREs) on DNA
- This stimulates transcription of many genes, leading to synthesis of new proteins including: Na⁺-K⁺ ATPase, cardiac myosin, β₁-adrenergic receptors, lysosomal enzymes, metabolic enzymes, and structural proteins
- These new proteins are responsible for the multiple physiological effects
Nongenomic mechanism:
- Some effects occur too rapidly to be explained by gene transcription
- Nongenomic actions occur at the plasma membrane, cytoplasm, and mitochondria
- Include regulation of ion channels and oxidative phosphorylation via cAMP and protein kinase cascades
Functions of Thyroid Hormones
1. Basal Metabolic Rate (BMR)
- Increase oxygen consumption in all tissues except the brain, gonads, and spleen
- Raise BMR by 60-100% above normal in excess
- Mechanism: upregulation of Na⁺-K⁺ ATPase activity → increased ATP hydrolysis → increased O₂ consumption and heat production
- This is why thyroid hormones are thermogenic
2. Metabolism
- Carbohydrates: Increase glucose absorption from GI tract, potentiate gluconeogenesis and glycogenolysis (via catecholamine and glucagon synergy)
- Fats: Stimulate lipolysis; increase fat mobilization and oxidation
- Proteins: Increase both protein synthesis and degradation - net effect is catabolic (decreased muscle mass), leading to negative nitrogen balance in excess
- Key enzymes induced: cytochrome oxidase, NADPH cytochrome C reductase, α-glycerophosphate dehydrogenase, malic enzyme
3. Cardiovascular System
- Increase cardiac output via:
- ↑ Heart rate (chronotropy)
- ↑ Stroke volume / contractility (inotropy)
- Mechanism: upregulation of β₁-adrenergic receptors in myocardium + synthesis of cardiac myosin and sarcoplasmic reticulum Ca²⁺ ATPase
- This explains why β-blockers (e.g. propranolol) control many symptoms of hyperthyroidism
- Also increase respiratory rate and ventilation to match increased O₂ demand
4. Growth and Development
- Synergize with growth hormone and somatomedins to promote bone formation
- Promote ossification, fusion of bone plates, and bone maturation
- In hypothyroidism: bone age lags chronologic age
5. Central Nervous System (CNS)
- Perinatal period: Essential for normal CNS maturation. Hypothyroidism here causes irreversible mental retardation (cretinism) - this is why neonatal thyroid screening is mandatory
- Adults:
- Hypothyroidism → lethargy, slowed movement, somnolence, impaired memory, decreased mental capacity
- Hyperthyroidism → hyperexcitability, hyperreflexia, irritability, tremor
6. Autonomic Nervous System
- Synergize with catecholamines - effects on BMR, heat production, heart rate, and stroke volume mirror adrenergic effects
- Sensitize tissues to sympathetic stimulation (via β₁ receptor upregulation)
Regulation (HPT Axis)
The Hypothalamic-Pituitary-Thyroid (HPT) axis regulates thyroid hormone levels:
- Hypothalamus releases TRH (thyrotropin-releasing hormone)
- Anterior pituitary responds by releasing TSH (thyroid-stimulating hormone)
- TSH stimulates T3/T4 synthesis and secretion
- Negative feedback: Elevated T3/T4 inhibits both TRH and TSH secretion, maintaining homeostasis
Notable regulatory stimuli:
- Cold exposure stimulates TRH → TSH → ↑ thyroid hormones (thermogenic adaptation)
- Fasting / low leptin → ↓ TRH → ↓ metabolic rate (energy conservation)
- Emotional stress / anxiety → acute ↓ TSH
Hyperthyroidism vs. Hypothyroidism at a Glance
| Feature | Hyperthyroidism | Hypothyroidism |
|---|---|---|
| BMR | ↑ | ↓ |
| Weight | Loss | Gain |
| Heat tolerance | Poor (heat intolerance) | Poor (cold intolerance) |
| Cardiac output | ↑ | ↓ |
| Nitrogen balance | Negative | Positive |
| CNS | Hyperexcitable, tremor | Lethargic, somnolent |
| Eye changes | Exophthalmos | Drooping eyelids |
| Skin | Sweating | Myxedema |
| Causes | Graves disease, TSH excess, neoplasm | Hashimoto thyroiditis, I⁻ deficiency, surgery |
| Treatment | Propylthiouracil, ¹³¹I, thyroidectomy, β-blockers | Hormone replacement |
Sources:
- Guyton and Hall Textbook of Medical Physiology, Ch. 77
- Costanzo Physiology, 7th Ed., Ch. 9 (pp. 423-429)
- Sabiston Textbook of Surgery, Ch. 73
Glucocorticoids
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of glucocorticoids, sourced from Medical Physiology (Boron & Boulpaep), Katzung's Basic and Clinical Pharmacology, and Goodman & Gilman's Pharmacological Basis of Therapeutics.
Glucocorticoids
Origin and Structure
Glucocorticoids are steroid hormones derived from cholesterol and produced by the zona fasciculata of the adrenal cortex (and to a lesser extent zona reticularis).
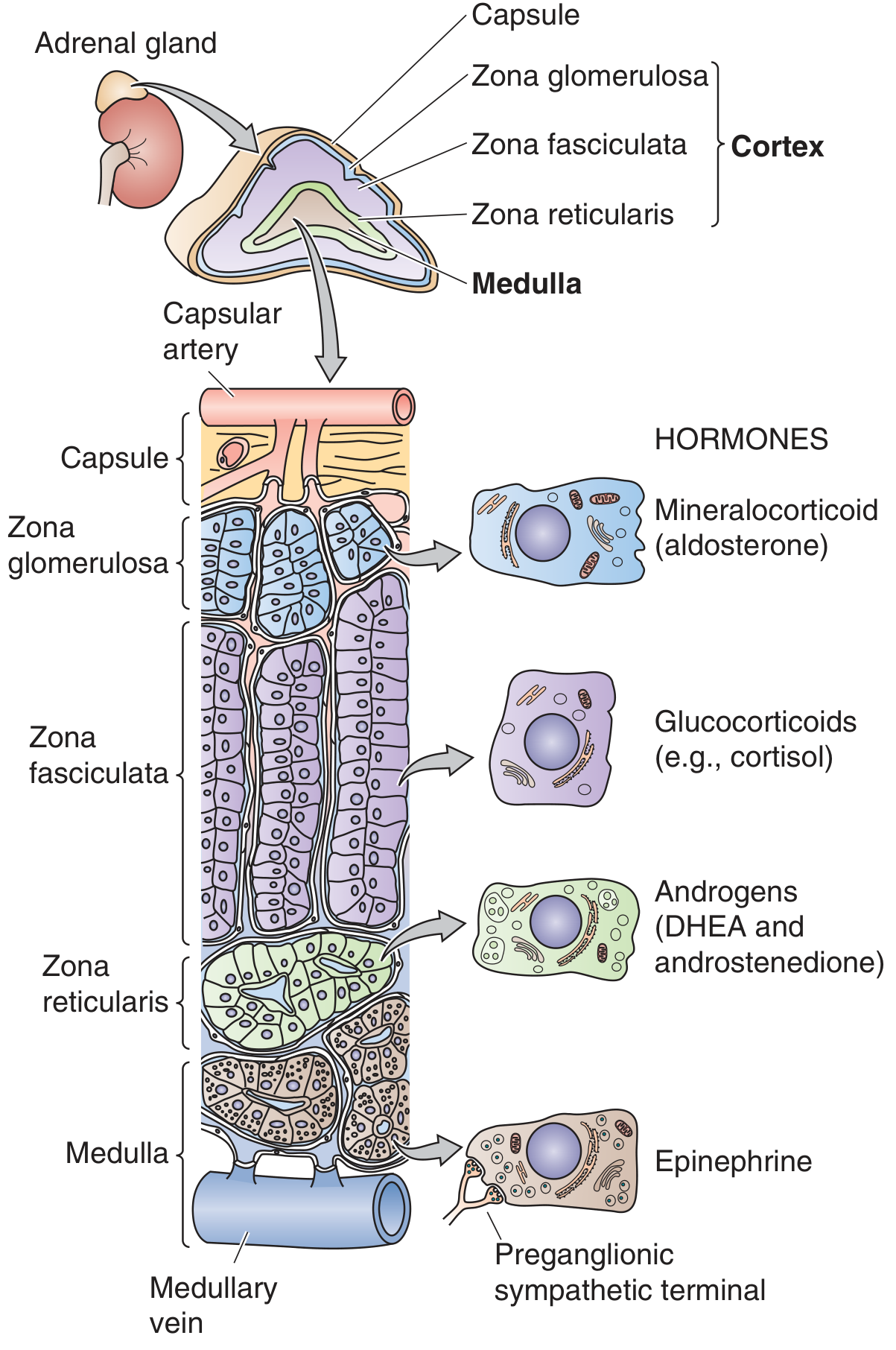
The principal endogenous glucocorticoid in humans is cortisol (hydrocortisone). Corticosterone is present in smaller amounts but is the primary glucocorticoid in rodents.
Adrenal Cortex Zonation (GFR Rule)
| Zone | Product |
|---|---|
| Zona Glomerulosa | Aldosterone (mineralocorticoid) |
| Zona Fasciculata | Cortisol (glucocorticoid) |
| Zona Reticularis | DHEA, androstenedione (androgens) |
Synthesis
- Cholesterol (from LDL or local synthesis) enters adrenal cells
- Mitochondrial enzyme StAR (steroidogenic acute regulatory protein) transfers cholesterol into the inner mitochondrial membrane - this is the rate-limiting step
- Cholesterol → Pregnenolone → Progesterone → 17α-hydroxyprogesterone → 11-deoxycortisol → Cortisol
- Key enzymes: 21α-hydroxylase (most common site of congenital adrenal hyperplasia) and 11β-hydroxylase
Once synthesized, cortisol diffuses freely into plasma:
- ~90% bound to corticosteroid-binding globulin (CBG / transcortin) - synthesized by the liver
- ~7% bound to albumin
- ~3-4% free (biologically active fraction)
Cortisol is inactivated by 11β-hydroxysteroid dehydrogenase (11β-HSD):
- 11β-HSD1 (liver, adipose): reversible; converts cortisone ⇌ cortisol (locally regenerates active cortisol)
- 11β-HSD2 (kidney, colon): irreversible; converts cortisol → inactive cortisone, protecting mineralocorticoid receptors from cortisol's actions
Mechanism of Action
Genomic (primary):
- Cortisol diffuses into the cell and binds the cytosolic glucocorticoid receptor (GR)
- The GR undergoes conformational change, releasing heat shock proteins, and the hormone-receptor complex translocates to the nucleus
- The GR binds glucocorticoid response elements (GREs) on DNA as a homodimer
- Activates or represses transcription of target genes (10-20% of all expressed genes are GR-regulated)
- Coactivators (with histone acetylase activity) and corepressors modulate transcriptional output
Nongenomic:
- Effects occurring within minutes (too fast for gene transcription)
- Mediated via membrane-associated GRs, G-protein-coupled receptors, and effects on ion channels
- Examples: rapid feedback suppression of ACTH, effects on glutamatergic neurons
Note: Cortisol can bind the mineralocorticoid receptor (MR) with similar affinity to aldosterone. In the kidney, 11β-HSD2 prevents this by inactivating cortisol locally, allowing aldosterone to act selectively.
Regulation: HPA Axis
Hypothalamus → CRH (corticotropin-releasing hormone)
↓
Anterior Pituitary → ACTH (derived from POMC precursor)
↓
Zona Fasciculata → Cortisol
↓ (negative feedback)
Inhibits both CRH and ACTH secretion
Key regulatory features:
- Circadian rhythm: Cortisol peaks in early morning (~6-8 AM), troughs at midnight. Controlled by the suprachiasmatic nucleus.
- Stress override: Physical or emotional stress activates higher CNS centers to stimulate CRH release, overriding normal feedback
- Pulsatile secretion: ACTH and cortisol are secreted in episodic pulses (~15-18/day)
- Arginine vasopressin (AVP): A secondary ACTH secretagogue, important during dehydration and trauma
Physiological Functions of Glucocorticoids
1. Metabolic Effects
Carbohydrate metabolism (glucose-raising):
- Stimulate gluconeogenesis in the liver (upregulate PEPCK, glucose-6-phosphatase, glycogen synthase)
- Promote glycogen synthesis in the liver
- Inhibit glucose uptake in peripheral muscle and adipose tissue (anti-insulin effect → hyperglycemia)
- Net result: maintain blood glucose supply to the brain, especially in the fasting state
Protein metabolism (catabolic):
- Catabolic in muscle, lymphoid tissue, connective tissue, skin, and bone
- Promote protein breakdown and release of amino acids → used as gluconeogenic substrate
- Stimulate protein synthesis only in the liver
- Chronic excess: muscle weakness, skin thinning, osteoporosis
Fat metabolism:
- Stimulate lipolysis via hormone-sensitive lipase
- Increased insulin (secondary to hyperglycemia) promotes lipogenesis simultaneously
- Net effect: fat redistribution - central (visceral) fat deposition, with peripheral fat loss (classic Cushingoid appearance: moon face, buffalo hump, truncal obesity, thin limbs)
2. Anti-inflammatory and Immunosuppressive Effects
This is the basis for widespread therapeutic use:
On leukocytes (after a single dose):
- ↑ Neutrophils in circulation (from bone marrow mobilization + reduced margination)
- ↓ Lymphocytes (T and B cells), monocytes, eosinophils, basophils
- Peak effect at 6 hours, dissipates in 24 hours
Molecular mechanisms of anti-inflammation:
- Inhibit production of inflammatory cytokines (IL-1, IL-2, IL-6, TNF-α, IFN-γ)
- Suppress arachidonic acid metabolism - inhibit phospholipase A2 (via annexin/lipocortin induction) → reduce prostaglandins, leukotrienes, and thromboxanes
- Suppress NF-κB (master regulator of inflammatory gene expression)
- Reduce capillary permeability and vasodilation (suppress histamine release from mast cells/basophils)
- Inhibit leukocyte adhesion molecule expression → prevent extravasation to sites of inflammation
- At high doses: reduce antibody production
3. Cardiovascular Effects ("Permissive" Actions)
- Permissive effect: Vascular smooth muscle responsiveness to catecholamines is diminished without cortisol - even physiological amounts restore normal vasomotor tone
- Increase blood pressure via enhanced vascular reactivity
- At high doses: some mineralocorticoid activity → sodium retention → hypertension
4. Renal Effects
- Cortisol deficiency → impaired GFR, augmented vasopressin secretion, inability to excrete a water load freely
- Physiological levels required for normal free water clearance
5. Central Nervous System Effects
- Adrenal insufficiency: slowed EEG alpha rhythm, depression
- Excess glucocorticoids: insomnia, euphoria (acute), then depression (chronic)
- Large doses: may raise intracranial pressure (pseudotumor cerebri)
- Hippocampal damage: genomic and nongenomic cortisol actions can be neurotoxic to hippocampal cells (which mediate negative feedback), contributing to a vicious cycle in chronic stress
6. Bone and Calcium Metabolism
- Inhibit osteoblast activity → reduced bone formation
- Increase osteoclast activity → increased bone resorption
- Inhibit calcium absorption from the gut (antagonize vitamin D)
- Long-term use → osteoporosis (major adverse effect of chronic steroid therapy)
7. Hematopoietic Effects
- ↑ Neutrophils, platelets, and red blood cells
- ↓ Lymphocytes, eosinophils, basophils, monocytes
8. Developmental / Fetal Effects
- Stimulate fetal lung maturation - induce surfactant production near term
- This is the basis for giving antenatal corticosteroids (betamethasone) to women at risk of preterm delivery
- Epigenetic effects on target genes: prenatal glucocorticoid exposure may have long-term consequences including predisposition to metabolic syndrome and depression
9. Effects on Other Endocrine Axes
- Chronic excess suppresses pituitary release of ACTH, GH, TSH, and LH
- Associated with peptic ulcer risk (possibly by suppressing local immune response to H. pylori)
Cushing Syndrome vs. Addison Disease
| Feature | Cushing Syndrome (Excess) | Addison Disease (Deficiency) |
|---|---|---|
| Glucose | Hyperglycemia | Hypoglycemia |
| Weight | Gain (central obesity) | Loss |
| Skin | Striae, easy bruising, thin skin | Hyperpigmentation (↑ ACTH/MSH) |
| Blood pressure | Hypertension | Hypotension |
| Electrolytes | Hypokalemia, sodium retention | Hyponatremia, hyperkalemia |
| Bone | Osteoporosis | - |
| Mood | Euphoria → depression | Depression, fatigue |
| Muscle | Proximal myopathy | Weakness |
| Causes | Pituitary adenoma (Cushing disease), adrenal tumor, iatrogenic | Autoimmune (most common), TB, adrenal hemorrhage |
Common Synthetic Glucocorticoids (Relative Potencies)
| Drug | Glucocorticoid Potency | Mineralocorticoid Potency | Duration |
|---|---|---|---|
| Cortisol (hydrocortisone) | 1 | 1 | Short |
| Prednisone | 4 | 0.8 | Intermediate |
| Methylprednisolone | 5 | 0.5 | Intermediate |
| Dexamethasone | 25-30 | ~0 | Long |
| Betamethasone | 25-30 | ~0 | Long |
Synthetic analogs are used clinically for anti-inflammatory, immunosuppressive, and replacement therapy. The absence of mineralocorticoid activity in dexamethasone/betamethasone makes them preferred in settings where fluid retention must be avoided.
Sources:
- Medical Physiology (Boron & Boulpaep), Ch. 50, pp. 1495-1504
- Katzung's Basic and Clinical Pharmacology, 16th Ed., Ch. 39
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Ch. 14
Physiology of Hypothalamus
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
Excellent material gathered. Now I have comprehensive content from Kandel's Principles of Neural Science and Blumenfeld's Neuroanatomy through Clinical Cases. Let me compile the full answer.
Physiology of the Hypothalamus
Overview
The hypothalamus is a small diencephalic structure (~4 g) that serves as the "homeostatic head ganglion" of the body. It lies beneath the thalamus, forming the walls and floor of the inferior portion of the third ventricle. Despite its small size, it is the central integrator of the autonomic nervous system, the endocrine system, and limbic functions. It maintains homeostasis by regulating four major systems:
- Homeostatic mechanisms - hunger, thirst, sexual desire, sleep-wake cycles
- Endocrine control - via the pituitary gland
- Autonomic control - cardiovascular, thermoregulatory, visceral
- Limbic mechanisms - emotion, stress responses (mnemonic: HEAL)
Anatomy and Location
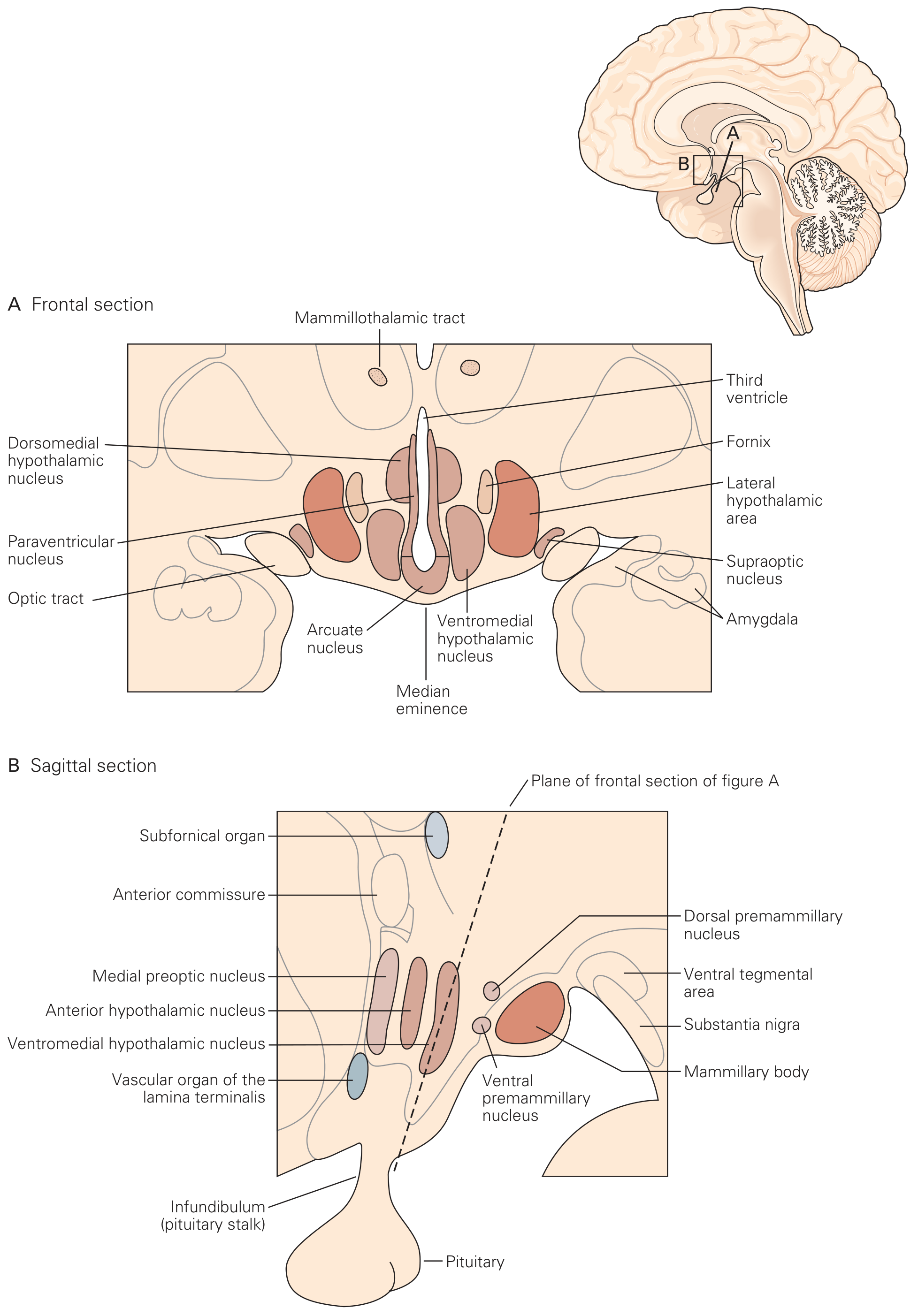
The hypothalamus is bounded:
- Anteriorly: Diagonal band of Broca
- Dorsally: Anterior commissure, bed nuclei of stria terminalis, zona incerta, thalamus
- Posteriorly: Ventral tegmental area and interpeduncular nucleus
On the ventral brain surface it includes the optic chiasm, tuber cinereum, median eminence, infundibulum (pituitary stalk), and mammillary bodies.
Zones and Nuclei
Rostrocaudal Divisions (Three Regions)
| Region | Location | Key Nuclei | Functions |
|---|---|---|---|
| Preoptic (anterior) | Above optic chiasm | Medial preoptic nucleus, suprachiasmatic nucleus, OVLT | Water balance, temperature, sleep, sexual behavior, circadian rhythms |
| Tuberal (middle) | Above pituitary | Arcuate, ventromedial, dorsomedial, paraventricular | Pituitary hormone secretion, energy balance, feeding |
| Mammillary (posterior) | Mammillary bodies | Posterior hypothalamic nucleus, mammillary nuclei | Memory (via mammillothalamic tract), arousal |
Mediolateral Divisions
| Zone | Key Structures |
|---|---|
| Periventricular zone | Thin layer adjacent to 3rd ventricle; neuroendocrine neurons (parvocellular) |
| Medial zone | Most hypothalamic nuclei; homeostatic regulation |
| Lateral zone | Lateral hypothalamic area; reward, arousal; medial forebrain bundle (MFB) runs through here |
Key Hypothalamic Nuclei and Their Functions
| Nucleus | Location | Primary Function |
|---|---|---|
| Suprachiasmatic (SCN) | Anterior, above optic chiasm | Master circadian clock; receives direct retinal input; drives sleep-wake and hormonal rhythms |
| Supraoptic (SON) | Anterior | Synthesizes ADH (vasopressin); osmoreception |
| Paraventricular (PVN) | Anterior/tuberal | Synthesizes oxytocin and ADH; also releases CRH, TRH; autonomic regulation |
| Arcuate | Tuberal, near median eminence | Releases GHRH, dopamine (inhibits prolactin); contains NPY/AgRP and POMC neurons for energy balance |
| Ventromedial (VMH) | Tuberal | Satiety center ("satiety nucleus"); lesion → hyperphagia and obesity |
| Dorsomedial (DMH) | Tuberal | Feeding behavior, circadian rhythm output |
| Lateral hypothalamic area (LHA) | Throughout | Hunger/feeding center; orexin/hypocretin neurons - wakefulness; lesion → anorexia and weight loss |
| Preoptic area (POA) | Anterior | Thermoregulation; sexual behavior |
| Posterior hypothalamus | Mammillary | Heat conservation; arousal |
| Mammillary bodies | Posterior | Memory (Papez circuit; lesion → Korsakoff amnesia) |
Six Vital Physiological Functions
1. Blood Pressure and Electrolyte Composition
- Regulates thirst, salt appetite, and drinking behavior
- Autonomic control of vasomotor tone
- Releases vasopressin (ADH) from the paraventricular nucleus in response to increased plasma osmolality or decreased blood volume
- Key sensors: OVLT (vascular organ of the lamina terminalis), subfornical organ (SFO), and median preoptic nucleus (MnPO) - circumventricular organs lacking a blood-brain barrier, allowing direct sampling of blood osmolality
2. Energy Metabolism
- Arcuate nucleus is the primary integrator:
- NPY/AgRP neurons: Orexigenic (stimulate feeding, reduce energy expenditure)
- POMC/CART neurons: Anorexigenic (suppress feeding, increase energy expenditure)
- Leptin (from adipose tissue) inhibits NPY/AgRP and activates POMC neurons - signals satiety and adequate fat stores
- Ghrelin (from stomach) activates NPY/AgRP neurons - signals hunger
- Regulates glucocorticoids, growth hormone, and TSH release to coordinate metabolism
3. Thermoregulation
- Preoptic area (POA) is the primary thermostat
- Warm-sensitive neurons in POA → activated by heat → trigger sweating and cutaneous vasodilation
- Cold signals from skin and core → activate heat-conserving responses: vasoconstriction, shivering, brown fat thermogenesis
- There is no single "set point" neuron; temperature is controlled by a distributed settling point of multiple feedback loops
4. Reproductive and Sexual Behavior
- Medial preoptic nucleus: Controls male sexual behavior
- Ventromedial and ventral premammillary nuclei: Female reproductive behavior
- GnRH pulse generator in arcuate/preoptic area: Drives pulsatile LH and FSH release from pituitary → regulates menstrual cycle and spermatogenesis
- Hypothalamic gonadostat: Suppressed in childhood by high sensitivity to sex steroid feedback; "reset" at puberty
5. Defensive Behavior (Stress Response)
- Paraventricular nucleus (PVN): Releases CRH → ACTH → cortisol (HPA axis activation)
- Anterior hypothalamic area and dorsal premammillary nucleus: Fight-or-flight responses to threats
- Coordinates autonomic (sympathetic activation) and endocrine (glucocorticoid) responses to stress
- Chronic stress and hippocampal damage can impair negative feedback of cortisol, perpetuating HPA axis hyperactivity
6. Sleep-Wake Cycle
- Suprachiasmatic nucleus (SCN): Master circadian pacemaker; synchronized by light input via the retinohypothalamic tract
- Lateral hypothalamic area (LHA): Contains orexin/hypocretin neurons that project widely to promote arousal and stabilize wakefulness
- Loss of orexin neurons → narcolepsy
- Tuberomammillary nucleus (TMN): Contains histaminergic neurons that promote wakefulness; blocked by antihistamines (causing sedation)
- Ventrolateral preoptic nucleus (VLPO): Sleep-promoting; inhibits arousal centers (histamine, orexin) via GABA and galanin - the "sleep switch"
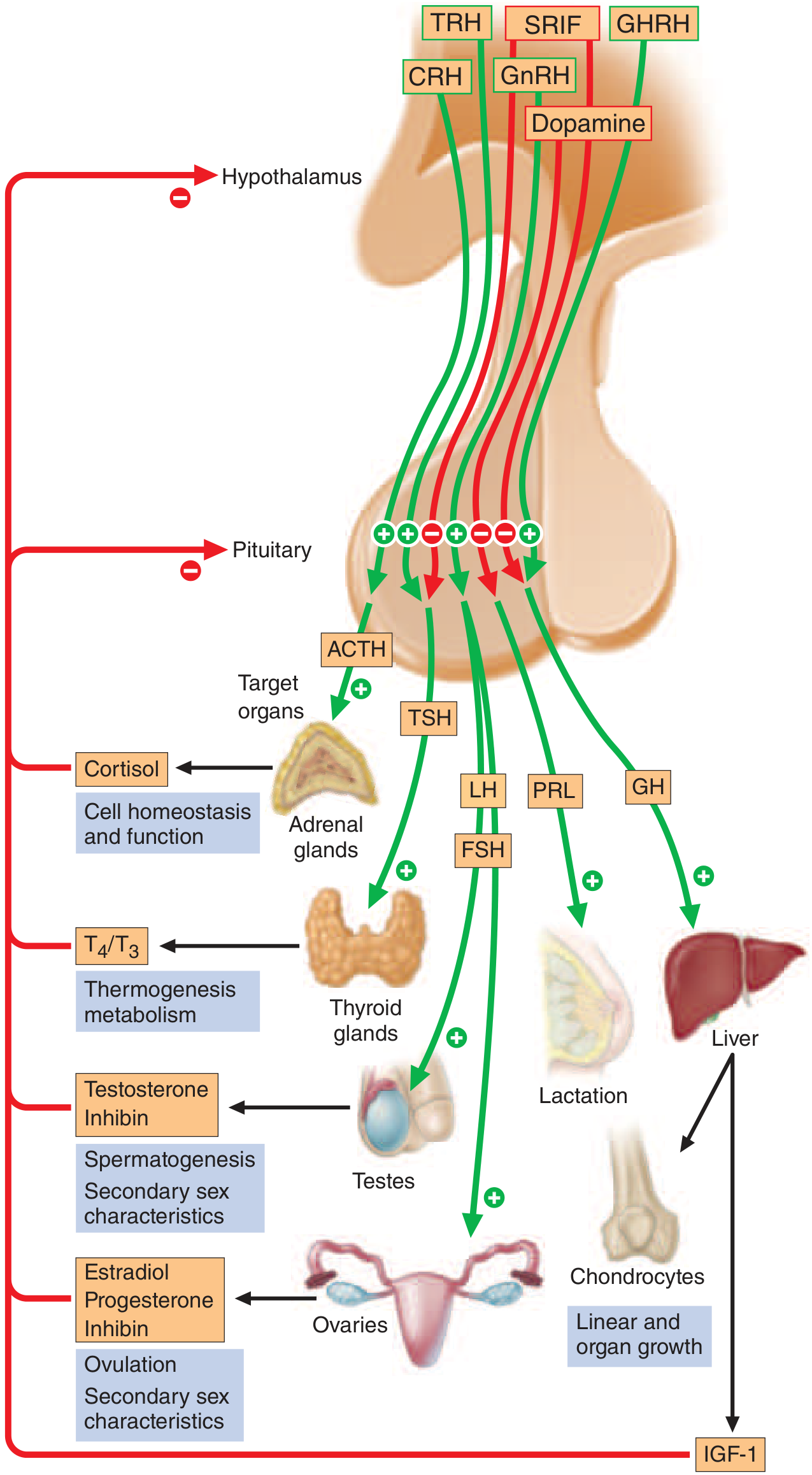
Neuroendocrine Control of the Pituitary
This is one of the hypothalamus's most critical roles.
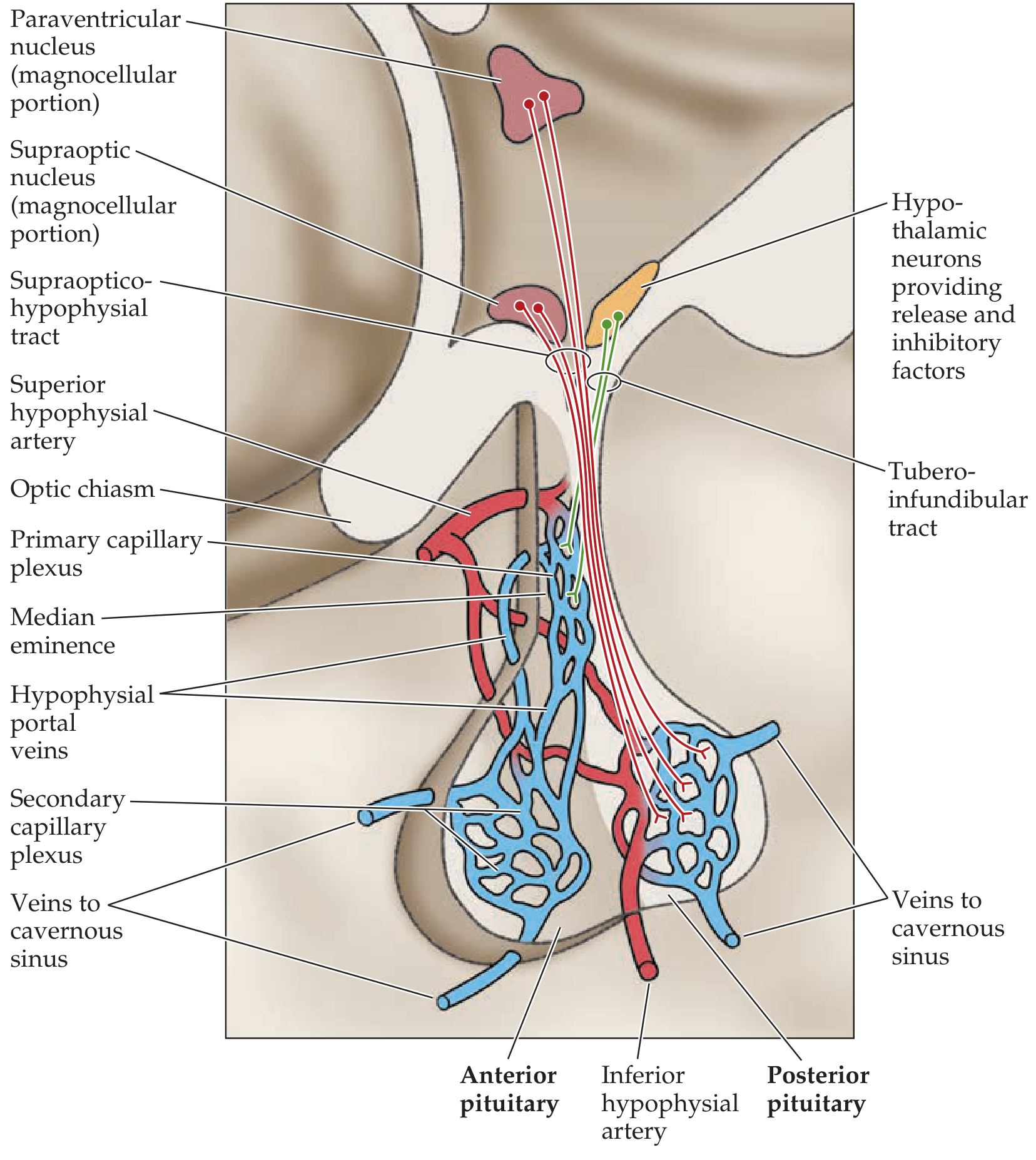
Anterior Pituitary (Adenohypophysis) - Controlled by Portal Blood
Parvocellular neurons in the hypothalamus release factors into the primary capillary plexus of the median eminence, which drain via hypophyseal portal veins to the secondary capillary plexus of the anterior pituitary. This is a unique portal system - blood flows from one capillary bed (median eminence) to another (anterior pituitary) before entering systemic circulation.
| Anterior Pituitary Hormone | Hypothalamic Releasing Factor | Hypothalamic Inhibitory Factor |
|---|---|---|
| ACTH | CRH (+ vasopressin) | - |
| TSH | TRH | Somatostatin |
| GH | GHRH | Somatostatin |
| Prolactin | PRF, TRH | Dopamine (PIF) |
| LH | GnRH | - |
| FSH | GnRH | - |
Note: Dopamine is the only non-peptide hypothalamic factor. It tonically inhibits prolactin - so hypothalamic damage or dopamine antagonists (antipsychotics) cause hyperprolactinemia.
Posterior Pituitary (Neurohypophysis) - Direct Axonal Secretion
The posterior pituitary contains axon terminals (not glandular cells) of neurons whose cell bodies lie in hypothalamic nuclei. There is no portal system here - hormones are secreted directly into fenestrated capillaries via the supraopticohypophysial tract.
| Hormone | Synthesized In | Stimuli | Actions |
|---|---|---|---|
| Vasopressin (ADH) | Mainly supraoptic nucleus (+ PVN) | ↑ plasma osmolality, ↓ blood volume, stress | Water reabsorption in renal collecting duct; vasoconstriction (V1 receptor) |
| Oxytocin | Mainly paraventricular nucleus (+ SON) | Parturition (cervical stretch), suckling | Uterine contraction, milk ejection; social bonding, trust |
Autonomic Output
The hypothalamus projects to autonomic preganglionic neurons via descending pathways:
- Sympathetic output: PVN → intermediolateral cell column of spinal cord → sympathetic ganglia → fight-or-flight (↑ HR, ↑ BP, pupil dilation, sweating, gluconeogenesis)
- Parasympathetic output: Anterior hypothalamus → dorsal motor nucleus of vagus and sacral cord → rest-and-digest
Key principle: The hypothalamus does not directly control most autonomic reflexes (e.g., micturition is mainly a brainstem/spinal reflex), but it modulates and integrates them according to whole-body homeostatic needs.
Circumventricular Organs (CVOs)
These are specialized regions adjacent to the hypothalamus that lack a full blood-brain barrier, allowing neurons to directly sense blood-borne signals:
| CVO | Location | Function |
|---|---|---|
| OVLT (vascular organ of lamina terminalis) | Anterior wall of 3rd ventricle | Osmoreception, angiotensin II sensing |
| Subfornical organ (SFO) | Dorsal 3rd ventricle | Angiotensin II sensing, thirst |
| Median eminence | Hypothalamic floor | Portal delivery of releasing factors |
| Area postrema | Brainstem | Chemoreception (vomiting center) |
Clinical Correlations
| Lesion / Condition | Nucleus/Region Affected | Key Features |
|---|---|---|
| Diabetes insipidus | Supraoptic/PVN or posterior pituitary | ADH deficiency → dilute polyuria, polydipsia |
| Kallmann syndrome | GnRH neurons (preoptic area) | GnRH deficiency → hypogonadotropic hypogonadism + anosmia |
| Craniopharyngioma | Hypothalamus/pituitary stalk | Panhypopituitarism, obesity, visual field defects |
| Narcolepsy | LHA orexin neurons (autoimmune destruction) | Sudden sleep attacks, cataplexy |
| Korsakoff amnesia | Mammillary bodies (thiamine deficiency) | Anterograde amnesia, confabulation |
| Hypothalamic obesity | VMH lesion | Hyperphagia, weight gain |
| Posterior hypothalamic lesion | Posterior hypothalamus | Poikilothermia (inability to regulate temperature) |
| Cushing disease | PVN - excess CRH → ACTH → cortisol (if pituitary adenoma) | Central obesity, hypertension, hyperglycemia |
Sources:
- Kandel et al., Principles of Neural Science, 6th Ed., Ch. 41
- Blumenfeld, Neuroanatomy through Clinical Cases, 3rd Ed., Ch. 17
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
Anterior and posterior pituitary gland physiology
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have thorough content from Harrison's Internal Medicine (22nd ed.), Kandel's Principles of Neural Science, and Katzung's Pharmacology. Let me compile the complete answer.
Anterior and Posterior Pituitary Gland Physiology
Overview
The pituitary gland (hypophysis) weighs ~600 mg and sits in the sella turcica at the base of the brain, ventral to the diaphragma sella. It has two structurally and functionally distinct lobes with entirely different embryological origins:
| Feature | Anterior Pituitary (Adenohypophysis) | Posterior Pituitary (Neurohypophysis) |
|---|---|---|
| Embryology | Rathke's pouch (oral ectoderm) | Evagination of the brain floor (neuroectoderm) |
| Cell type | Glandular epithelial cells | Axon terminals of hypothalamic neurons |
| Blood supply | Superior hypophyseal arteries (via portal system) | Inferior hypophyseal arteries |
| Control by hypothalamus | Indirect - via portal blood-borne factors | Direct - via axonal transport and release |
| Hormones | ACTH, TSH, GH, PRL, LH, FSH | ADH (vasopressin), Oxytocin |
Part I: Anterior Pituitary (Adenohypophysis)
The anterior pituitary is often called the "master gland" because, together with the hypothalamus, it orchestrates the complex regulatory functions of most other endocrine glands.
The Hypothalamo-Hypophyseal Portal System
Parvocellular neurons of the hypothalamus project axons to the median eminence (outside the blood-brain barrier), where they release releasing/inhibiting factors into the primary capillary plexus. These factors are then carried by the hypophyseal portal veins to the secondary capillary plexus of the anterior pituitary, where they bind receptors on specific pituitary cell types. This system allows high local concentrations of hypothalamic factors to reach the pituitary before dilution in the systemic circulation. Hormones are secreted in pulsatile fashion.
Five Cell Types and Their Hormones
| Cell Type | % of Cells | Transcription Factor | Hormone | Molecular Type |
|---|---|---|---|---|
| Corticotrope | ~20% | T-Pit | ACTH (from POMC) | Polypeptide, 39 aa |
| Somatotrope | ~50% | Prop-1, Pit-1 | Growth Hormone (GH) | Polypeptide, 191 aa |
| Lactotrope | ~20% | Prop-1, Pit-1 | Prolactin (PRL) | Polypeptide, 198 aa |
| Thyrotrope | ~5% | Prop-1, Pit-1, TEF | TSH | Glycoprotein (α + β subunits) |
| Gonadotrope | ~10% | SF-1, DAX-1 | LH, FSH | Glycoproteins (α + β subunits) |
LH, FSH, and TSH are all glycoproteins sharing a common α subunit - their specificity comes from unique β subunits.
Anterior Pituitary Hormones in Detail
1. ACTH (Adrenocorticotropic Hormone)
- Derived from: POMC (pro-opiomelanocortin, 266 aa precursor) - also yields β-lipotropin, β-endorphin, α-MSH, and CLIP
- Stimulated by: CRH (41 aa, from PVN), AVP, and pro-inflammatory cytokines (IL-6)
- Inhibited by: Glucocorticoids (negative feedback at pituitary and hypothalamus)
- Secretion pattern: Pulsatile with marked circadian rhythm - peaks early morning (6-8 AM), troughs at midnight; stress can override this completely
- Target: Zona fasciculata of adrenal cortex → cortisol synthesis and secretion
- Also stimulates: Adrenal androgen production (DHEA) and, in large amounts, aldosterone
2. Growth Hormone (GH)
- Structure: 191 amino acids, 22 kDa (main isoform); 5 genes in GH/PRL/hPL gene cluster
- Stimulated by: GHRH (44 aa, from arcuate nucleus), ghrelin (octanoylated gastric peptide), fasting, exercise, deep sleep (highest peaks at sleep onset), estrogen
- Inhibited by: Somatostatin (SRIF, from periventricular/preoptic area), IGF-1 (long-loop feedback), hyperglycemia (glucose load suppresses GH)
- Secretion: Pulsatile; highest levels during slow-wave sleep; declines markedly with age (~15% of pubertal levels in middle age); higher in women
- Direct actions:
- Lipolysis and fatty acid oxidation
- Anti-insulin effect (promotes insulin resistance in peripheral tissues)
- Stimulates amino acid uptake and protein synthesis in muscle
- Indirect actions (via IGF-1):
- Liver produces IGF-1 (insulin-like growth factor 1), which mediates most of the growth-promoting effects
- Stimulates chondrocyte proliferation → linear bone growth
- IGF-1 levels peak at age 16, then decline >80% across lifespan
3. Prolactin (PRL)
- Structure: 198 amino acids; weakly homologous to GH and hPL (from common ancestral gene)
- Unique regulatory feature: The only anterior pituitary hormone under predominantly tonic inhibitory control - dopamine from the arcuate nucleus tonically suppresses PRL release
- This explains why pituitary stalk section or dopamine receptor antagonists (antipsychotics, metoclopramide) cause hyperprolactinemia
- Stimulated by: Estrogen (major physiological stimulus; explains rise in pregnancy), TRH, VIP, suckling (via afferent neural pathways), stress
- Inhibited by: Dopamine (D2 receptor-mediated; basis for bromocriptine/cabergoline therapy)
- Secretion: Pulsatile; highest levels during non-REM sleep (4-6 AM); normal adult levels: 10-25 µg/L (women), 10-20 µg/L (men); t½ ~50 min; rises ~10-fold during pregnancy
- Actions:
- Initiates and maintains lactation (in conjunction with insulin, glucocorticoids, and estrogen)
- Inhibits GnRH → suppresses LH/FSH → postpartum lactational amenorrhea (inhibits ovulation)
- Stimulates mammary gland development
- In males: inhibits testosterone production and libido if elevated
4. TSH (Thyroid-Stimulating Hormone)
- Structure: Glycoprotein with common α subunit + specific TSH-β subunit; 211 amino acids total
- Stimulated by: TRH (hypothalamic tripeptide: pyroGlu-His-Pro-NH₂)
- Inhibited by: T3/T4 (primary negative regulator), dopamine, somatostatin, glucocorticoids
- Secretion pattern: Pulsatile with modest amplitude; single measurement is adequate (unlike GH)
- Actions: Binds GPCR on thyroid follicular cells → stimulates T3/T4 synthesis and secretion; promotes follicular cell hypertrophy and hyperplasia (goiter when chronically elevated)
- Clinical note: In primary hypothyroidism (thyroid failure), loss of T3/T4 feedback → markedly elevated TSH; thyrotrope hyperplasia may enlarge the pituitary visibly on MRI
5. LH and FSH (Gonadotropins)
- Structure: Both are glycoproteins sharing the common α subunit; LH has a unique β subunit (204 aa), FSH has a unique β subunit (210 aa)
- Stimulated by: GnRH (pulsatile, from scattered preoptic/arcuate neurons; also called LHRH), activins, estrogen (positive feedback at mid-cycle for LH surge); GnRH pulsatility is controlled by kisspeptin neurons
- Inhibited by: Sex steroids, inhibin (from gonads)
- Secretion: Pulsatile; LH pulses tightly track GnRH pulses; pulse frequency and amplitude vary across menstrual cycle
- Key principle: Pulsatile GnRH stimulates LH/FSH; continuous GnRH exposure causes receptor downregulation and suppresses gonadotropin release (basis for GnRH agonist therapy in prostate cancer, endometriosis)
- Actions:
- In females: FSH promotes follicular development; LH triggers ovulation and luteinization
- In males: FSH drives spermatogenesis; LH stimulates Leydig cells → testosterone production
Hypothalamic Factors - Summary Table
| Releasing Factor | Pituitary Effect | Inhibitory Factor |
|---|---|---|
| CRH | ↑ ACTH | (none specific) |
| TRH | ↑ TSH, ↑ PRL | Somatostatin |
| GHRH | ↑ GH | Somatostatin |
| GnRH | ↑ LH, ↑ FSH | (none; relies on pulse frequency) |
| PRF / TRH | ↑ PRL | Dopamine (tonic) |
Part II: Posterior Pituitary (Neurohypophysis)
The posterior pituitary is a direct extension of the brain - it contains no glandular cells, only axon terminals. Hormones are synthesized in hypothalamic nuclei, packaged into neurosecretory vesicles, and transported down the supraopticohypophyseal tract (also called the hypothalamo-hypophyseal tract) to be stored and released in the posterior pituitary.
The Two Posterior Pituitary Hormones
Both are nonapeptides (9 amino acids) with a 6-amino acid disulfide ring and a 3-amino acid tail. Their genes are structurally similar and likely arose by gene duplication.
1. Vasopressin (ADH - Antidiuretic Hormone)
- Synthesized in: Mainly supraoptic nucleus (also PVN)
- Structure: Nonapeptide; in humans, position 8 is arginine (hence "arginine vasopressin", AVP)
- Stimuli for release:
- ↑ plasma osmolality (detected by osmoreceptors in OVLT, SFO, and hypothalamus) - most sensitive stimulus (1% rise in osmolality is detectable)
- ↓ blood volume / ↓ blood pressure (detected by carotid/aortic baroreceptors and cardiac volume receptors) - less sensitive but override osmotic signals in hemorrhage
- Nausea, pain, stress, angiotensin II, nicotine
- Inhibited by: ↓ osmolality, ↑ blood volume, ethanol, ANP
- Receptors and actions:
- V1 receptors (vascular smooth muscle): Vasoconstriction via Gq → phospholipase C → IP₃ → Ca²⁺
- V2 receptors (renal collecting duct): Water reabsorption via Gs → adenylyl cyclase → cAMP → PKA → aquaporin-2 (AQP2) insertion into apical membrane
- V2-like extrarenal receptors: Stimulate release of factor VIII and von Willebrand factor
- t½: ~15 minutes
- Clinical relevance:
- Central (neurogenic) diabetes insipidus: ADH deficiency → dilute polyuria (>3 L/day), polydipsia; treated with desmopressin (DDAVP), a long-acting V2-selective synthetic analogue
- SIADH (syndrome of inappropriate ADH): Excess ADH → hyponatremia, concentrated urine
2. Oxytocin
- Synthesized in: Mainly paraventricular nucleus (also SON)
- Structure: Nonapeptide; differs from vasopressin at positions 3 and 8
- Stimuli for release:
- Cervical and vaginal stretch during labor (Ferguson reflex - positive feedback)
- Nipple stimulation / suckling (neuroendocrine reflex)
- Estrogen (sensitizes hypothalamic neurons)
- Actions:
- Uterus: Stimulates myometrial contraction during labor; uterine sensitivity to oxytocin increases near term (↑ oxytocin receptors)
- Mammary gland: Stimulates myoepithelial cell contraction → milk ejection ("let-down reflex")
- CNS effects: Promotes social bonding, trust, maternal behavior, pair bonding; reduces anxiety
- Cardiovascular: Minor vasodilatory effects at high doses
- Clinical relevance: Synthetic oxytocin (Pitocin) is used to induce or augment labor and to control postpartum hemorrhage (contracts uterine myometrium)
Feedback Control
The entire system operates on negative feedback at multiple levels:
Hypothalamus ─→ Releasing hormone ─→ Anterior pituitary ─→ Trophic hormone ─→ Target gland ─→ Peripheral hormone
↑_____________________________negative feedback___________________________________|
↑___________________negative feedback__________________________|
- Short-loop feedback: Pituitary hormones feed back to inhibit hypothalamic releasing factors
- Long-loop feedback: Peripheral hormones (cortisol, T3/T4, sex steroids, IGF-1) inhibit both pituitary and hypothalamic levels
- All pituitary axes except PRL are net stimulatory; PRL is under net tonic inhibition
Clinical Correlations
| Condition | Pathology | Key Features |
|---|---|---|
| Acromegaly | GH excess (somatotrope adenoma) | Acral enlargement, coarse features, organomegaly, IGF-1 ↑, glucose intolerance |
| Cushing disease | ACTH excess (corticotrope adenoma) | Central obesity, striae, hypertension, hyperglycemia, osteoporosis |
| Prolactinoma | PRL excess (lactotrope adenoma - most common pituitary tumor) | Amenorrhea, galactorrhea (women); hypogonadism, erectile dysfunction (men) |
| Panhypopituitarism | Loss of all anterior pituitary hormones | Adrenal insufficiency, hypothyroidism, hypogonadism, GH deficiency; may follow apoplexy or large tumor |
| Craniopharyngioma | Compression of pituitary stalk | Hyperprolactinemia (stalk effect), diabetes insipidus, visual field defects |
| Central diabetes insipidus | ADH deficiency | Dilute polyuria, polydipsia, high serum osmolality; responds to DDAVP |
| SIADH | ADH excess | Hyponatremia, concentrated urine; causes include CNS disease, drugs, malignancy |
| Sheehan syndrome | Pituitary infarction (postpartum hemorrhage) | Failure to lactate (PRL deficiency) as first sign, then progressive hypopituitarism |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed., Ch. 390 (pp. 3031-3035)
- Kandel et al., Principles of Neural Science, 6th Ed., Ch. 41
- Katzung's Basic and Clinical Pharmacology, 16th Ed., Ch. 37
Auditory pathway
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent content gathered from three authoritative sources. Now I'll compile the full comprehensive answer.
Auditory Pathway
Overview: The Relay Chain
The auditory pathway carries sound information from the cochlea to the primary auditory cortex via four major relay stations. A useful mnemonic for the sequence is:
ECOLI - Eighth nerve → Cochlear nucleus → Olivary complex → Lateral lemniscus → Inferior colliculus → (then MGN → Cortex)
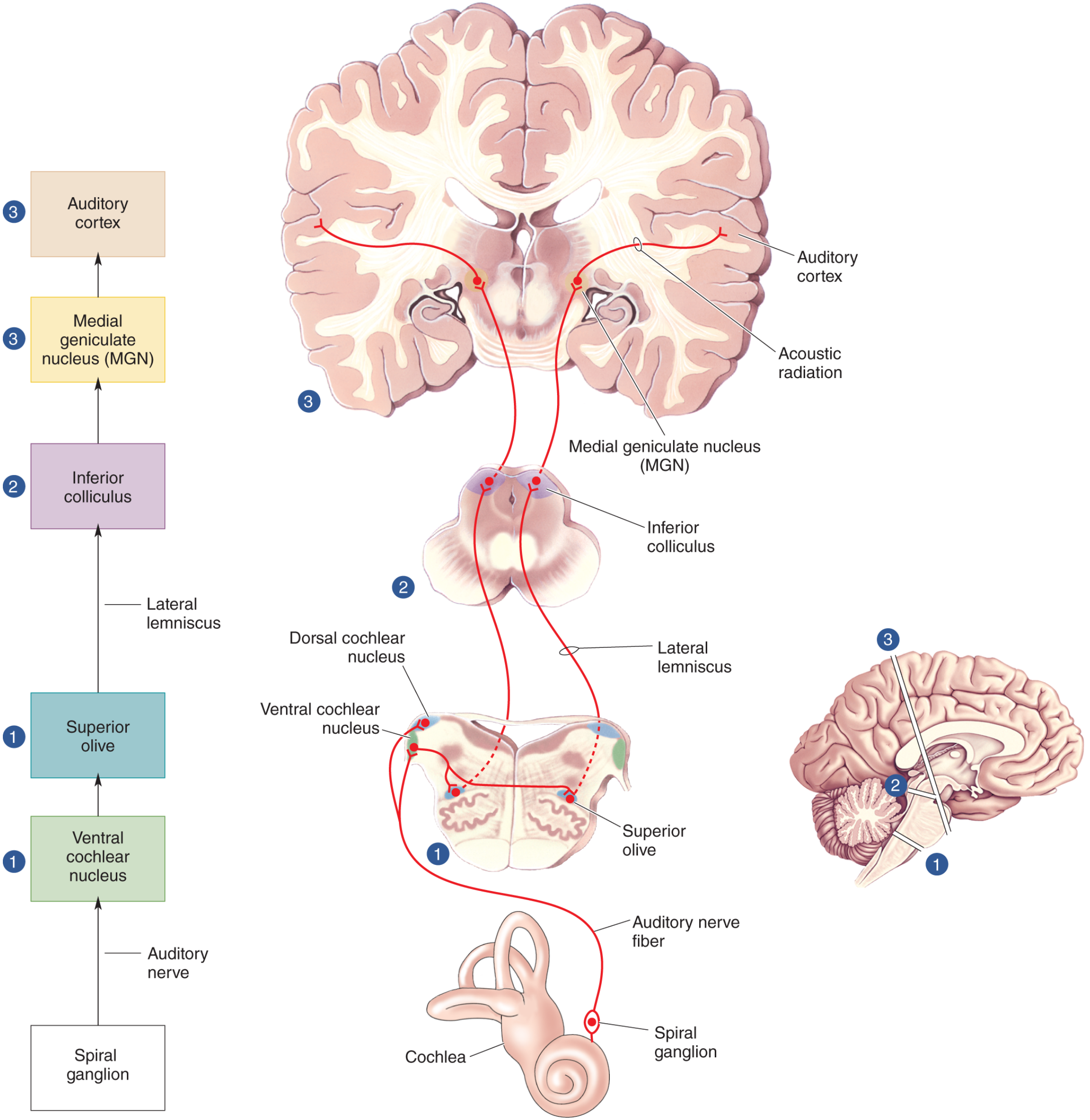
Step 1 - First-Order Neurons: Cochlea → CN VIII → Cochlear Nuclei
The Cochlea and Hair Cells
Sound waves enter the external auditory canal → vibrate the tympanic membrane → ossicles (malleus, incus, stapes) → oval window → basilar membrane of the cochlea.
The basilar membrane performs a physical frequency analysis (tonotopy):
- Apex: Wide and floppy → responds best to low frequencies
- Base: Narrow and stiff → responds best to high frequencies
Vibration deflects stereocilia on hair cells of the organ of Corti (sits on the basilar membrane, within the scala media):
- Inner hair cells (IHCs): ~3,500 total; the primary sensory receptors - 95% of afferent fibers contact IHCs; each IHC contacts ~20 spiral ganglion fibers
- Outer hair cells (OHCs): ~12,000 total; act as a cochlear amplifier - they actively contract/elongate (electromotility) to amplify basilar membrane motion by up to 100-fold, greatly improving sensitivity and frequency selectivity
When stereocilia deflect, mechanically gated K⁺ channels open (endocochlear potential drives K⁺ into hair cells) → depolarization → Ca²⁺ entry → glutamate release onto spiral ganglion dendrites.
Spiral Ganglion and CN VIII
- Cell bodies of first-order neurons lie in the spiral ganglion (housed in the canal of Rosenthal)
- Peripheral processes synapse on hair cells; central processes form the cochlear nerve (division of CN VIII)
- CN VIII enters the brainstem at the pontomedullary junction (cerebellopontine angle)
- Each spiral ganglion neuron has a characteristic frequency - fires best to one frequency, with broader responses at higher intensities
Step 2 - Second-Order Neurons: Cochlear Nuclei
The cochlear nerve bifurcates and innervates two cochlear nuclei ipsilaterally:
| Nucleus | Location | Major Projections |
|---|---|---|
| Dorsal cochlear nucleus (DCN) | Medulla (dorsal) | Fibers cross via dorsal acoustic striae → contralateral lateral lemniscus (bypasses superior olive) |
| Ventral cochlear nucleus (VCN) | Medulla (ventral) | Anteroventral and posteroventral subdivisions; projects via trapezoid body to both superior olivary complexes |
Critical clinical principle: The cochlear nuclei are the only stations in the auditory pathway that receive input from one ear only (ipsilateral). All higher auditory relay stations receive input from both ears. Therefore, a unilateral brainstem lesion above the cochlear nucleus level cannot produce monaural deafness - only lesions at or below the cochlear nucleus or cochlear nerve itself will cause single-ear deafness.
Both nuclei are organized tonotopically: dorsal portions receive high-frequency basal fibers; ventral portions receive low-frequency apical fibers. This tonotopic organization is preserved throughout the entire pathway.
Three acoustic striae carry fibers from the cochlear nuclei upward:
- Dorsal acoustic stria - from DCN
- Intermediate acoustic stria - from dorsal VCN
- Ventral acoustic stria (trapezoid body) - from VCN; major decussation; crosses in the caudal pons
Step 3 - The Superior Olivary Complex (SOC)
Located in the lower pons, the SOC is the first binaural station in the pathway - the first place where inputs from both ears converge. This convergence is the basis for sound localization.
Two mechanisms of sound localization:
A. Interaural Time Difference (ITD) - for LOW frequencies (<1500 Hz):
- Sound from one side reaches the near ear slightly before the far ear (up to 600 µsec difference)
- Medial superior olive (MSO) neurons act as coincidence detectors - they fire maximally when inputs from both ears arrive simultaneously (Jeffress model)
- Humans can discriminate differences as small as 10 µsec, achieving ~1-2° precision in horizontal localization
B. Interaural Level Difference (ILD) - for HIGH frequencies (>1500 Hz):
- The head creates an acoustic "shadow" - the far ear receives a quieter sound
- Lateral superior olive (LSO) neurons compare the loudness of sound at each ear
- Excited by the ipsilateral ear, inhibited by the contralateral ear (via the medial nucleus of the trapezoid body, MNTB)
The SOC also gives rise to the olivocochlear efferent bundle (~1,000 fibers per side), which projects back to the cochlea:
- Releases acetylcholine onto outer hair cells
- Suppresses OHC amplification - modulates gain of the cochlear amplifier (protective function, attention-related filtering)
Step 4 - Lateral Lemniscus
The lateral lemniscus is the main ascending auditory tract of the brainstem:
- Runs through the pons and midbrain tegmentum
- Contains axons from both cochlear nuclei (both direct and after relay in the SOC)
- Contains additional relay neurons: nuclei of the lateral lemniscus (NLL) (dorsal and ventral)
- The two lateral lemnisci are connected by the commissure of Probst
- All fibers converge onto the inferior colliculus
Step 5 - Third-Order Neurons: Inferior Colliculus (IC)
Located in the dorsal midbrain (tectum), the inferior colliculus is the obligatory relay for all ascending auditory information - all auditory pathways converge here.
Structure:
- Central nucleus: Strict tonotopic organization; the core auditory relay
- Pericentral nucleus: Part of the "belt" system; receives polymodal input
Functions:
- Integrates inputs from both ears (bilateral)
- Processes complex sound features (duration, frequency modulation)
- Encodes sound location in space
- Generates auditory reflexes (e.g., startle response via connections to reticular formation)
- Projects to the superior colliculus (audiovisual integration for orienting responses)
- Sends efferents to the cerebellum
The two inferior colliculi are connected by the commissure of the inferior colliculus. The central nucleus of one IC also connects to the contralateral medial geniculate nucleus via the brachium of the inferior colliculus.
Blood supply: Branches of the superior cerebellar and quadrigeminal arteries.
Step 6 - Fourth-Order Neurons: Medial Geniculate Nucleus (MGN) of Thalamus
The MGN is the thalamic auditory relay - the gateway to the cortex.
| Division | Projection | Function |
|---|---|---|
| Ventral (principal) nucleus | Heschl's gyrus (AI, Brodmann area 41) | Tonotopic; pure frequency/intensity analysis |
| Dorsal nucleus | Association auditory cortex (AII, Brodmann area 42) | Complex sound processing; polymodal |
| Medial (magnocellular) nucleus | Multiple cortical areas | Diffuse; responds to arousing novel sounds |
Important: There are no commissural connections between the two medial geniculate nuclei (unlike all other auditory relay levels). This has clinical relevance - each MGN processes predominantly contralateral ear information.
Blood supply: Thalamogeniculate arteries (branches of the posterior cerebral artery).
The MGN sends fibers as the auditory radiations (geniculocortical fibers), which travel through the posterior limb of the internal capsule and beneath the putamen to reach the cortex.
Step 7 - Auditory Cortex
Located in the superior temporal gyrus (Heschl's transverse temporal gyri), buried in the lateral sulcus (Sylvian fissure):
| Area | Brodmann | Name | Function |
|---|---|---|---|
| Primary auditory cortex (AI) | 41 | Heschl's gyrus | Tonotopic map; frequency analysis; high tones medial, low tones lateral |
| Secondary auditory cortex (AII) | 42 | Planum temporale region | Complex sound patterns, speech processing |
| Auditory association cortex | 22 | Wernicke's area (left) | Language comprehension (dominant hemisphere) |
Tonotopy in AI:
- Low tones → anterolateral
- High tones → posteromedial
- Neurons are arranged in isofrequency columns
Cortical processing:
- Like the visual system, auditory processing follows two streams:
- "What" (ventral) stream: Temporal lobe - sound identification (what is it?)
- "Where" (dorsal) stream: Parietal lobe - spatial localization (where is it?)
- Most neurons in AI respond to input from both ears, but strips of cells are excited by the contralateral ear and inhibited by the ipsilateral ear
Hemispheric specialization:
- Left Wernicke's area: Language/speech processing (dominant)
- Right auditory cortex: Melody, pitch, sound intensity, prosody
The two auditory cortices are connected through the corpus callosum.
Blood supply: Branches of the middle cerebral artery.
Summary Table: Ascending Auditory Pathway
| Level | Structure | Location | Key Feature |
|---|---|---|---|
| 1st order | Spiral ganglion → CN VIII | Cochlea / IAC | Ipsilateral; tonotopic |
| 2nd order | Dorsal + Ventral cochlear nuclei | Medulla | First synapse; ipsilateral input only |
| - | Trapezoid body | Caudal pons | Major decussation |
| - | Superior olivary complex | Lower pons | First binaural station; sound localization |
| - | Lateral lemniscus (+ NLL) | Pons/midbrain | Bilateral ascending tract |
| 3rd order | Inferior colliculus | Dorsal midbrain | Obligatory relay; all pathways converge |
| 4th order | Medial geniculate nucleus | Thalamus | Thalamic relay; no interhemispheric commissure |
| Cortex | Primary auditory cortex (AI) | Heschl's gyrus, BA 41 | Tonotopic; conscious hearing |
| Cortex | Association cortex (AII, Wernicke's) | BA 42, 22 | Language; complex sound analysis |
Bilateral Representation - Clinical Significance
Because auditory signals cross at multiple levels (trapezoid body, commissures of Probst and IC), each hemisphere receives input from both ears beyond the cochlear nucleus level. This has critical clinical implications:
- Cochlear nerve / cochlear nucleus lesion → ipsilateral deafness
- Unilateral brainstem lesion above cochlear nuclei → no monaural deafness (bilateral representation protects hearing)
- Unilateral temporal lobe lesion → subtle deficits (dichotic listening difficulty) - not frank deafness, because the opposite cortex still receives bilateral input
- Bilateral temporal lobe lesions → cortical deafness
Blood Supply Summary
| Structure | Artery |
|---|---|
| Cochlea, CN VIII, cochlear nuclei | Internal auditory artery (branch of AICA) |
| Superior olivary complex, lateral lemniscus | Circumferential branches of basilar artery |
| Inferior colliculus | Superior cerebellar + quadrigeminal arteries |
| Medial geniculate nucleus | Thalamogeniculate arteries (PCA branches) |
| Auditory cortex | Middle cerebral artery branches |
Brainstem Auditory Evoked Potentials (BAEPs / ABR)
Clinically, the auditory pathway can be evaluated non-invasively by recording brainstem auditory evoked potentials (click-evoked):
| Wave | Generator |
|---|---|
| Wave I | Distal CN VIII (cochlear nerve) |
| Wave II | Proximal CN VIII / cochlear nucleus |
| Wave III | Superior olivary complex |
| Wave IV | Lateral lemniscus / nuclei |
| Wave V | Inferior colliculus |
| Waves VI-VII | MGN / thalamocortical radiation |
Prolonged inter-peak latencies localize lesions along the pathway - useful for detecting acoustic neuroma, demyelination, and brainstem lesions.
Sources:
- Neuroscience: Exploring the Brain, 5th Ed., Ch. 11
- Ganong's Review of Medical Physiology, 26th Ed., Ch. 11
- Localization in Clinical Neurology, 8th Ed., Ch. 11 (pp. 818-821)
This is a shared conversation. Sign in to Orris to start your own chat.