Explain about DDH
"developmental dysplasia of the hip"[MeSH Terms] AND diagnosis
Developmental Dysplasia of the Hip (DDH)
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 1401
- Bailey and Love's Short Practice of Surgery 28th Ed, p. 637
Incidence
- True dislocation: ~1-2 per 1000 live births
- Neonatal instability (broader): ~20 per 1000 live births
- Ultrasound screening picks up far more cases, but many resolve spontaneously
- Left hip is more commonly affected than the right; bilateral > unilateral right involvement
Aetiology and Risk Factors
| Risk Factor | Detail |
|---|---|
| Female sex | 4-5x more common; maternal relaxin increases neonatal ligamentous laxity |
| Breech presentation | Particularly extended breech; abnormal hip flexion forces |
| Firstborn | Tight primigravid uterus restricts fetal movement |
| Family history | Risk increases to ~10% with positive family history |
| Oligohydramnios | Restricts fetal movement |
| Left hip predominance | LOA position places left hip adducted against maternal lumbosacral spine |
| Swaddling | Legs-together swaddling worsens instability |
| Associated conditions | Congenital muscular torticollis (coexistence ~8%), metatarsus adductus, talipes calcaneovalgus |
Pathology and Secondary Changes
- The capsule becomes permanently elongated
- The psoas tendon may obstruct reduction anteriorly
- The limbus acetabuli hypertrophies at the periphery
- The ligamentum teres hypertrophies and elongates
- The femoral head becomes reduced in size with posteromedial flattening
- Coxa valga and excessive anteversion develop
- The true acetabulum becomes shallow
Clinical Presentation (Age-Dependent)
Neonates (< 6 months)
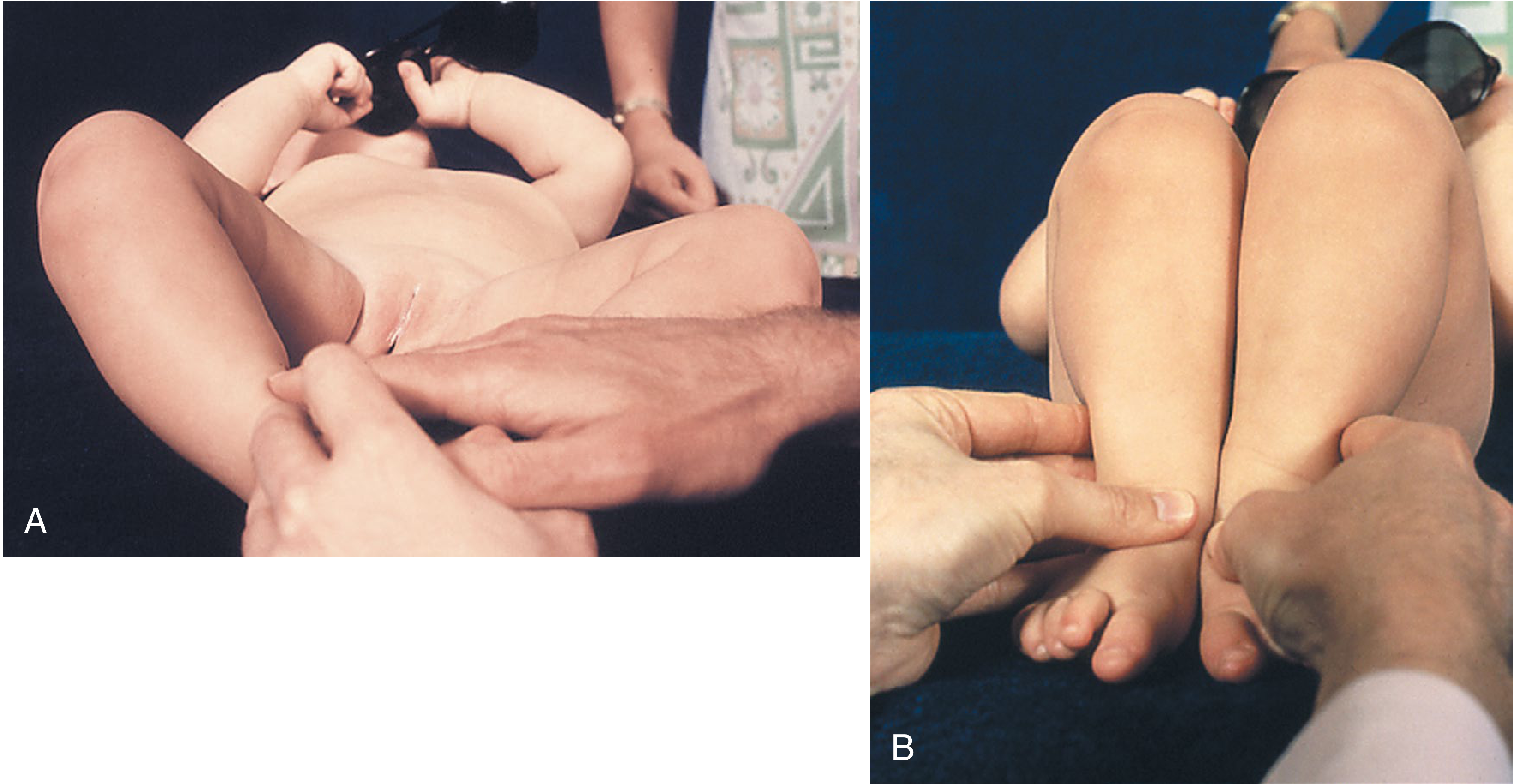
- Ortolani test: With the hip flexed and abducted, a palpable clunk is felt as the posteriorly dislocated femoral head relocates into the acetabulum - a positive sign indicates a reducible dislocation.
- Barlow test: The flexed hip is adducted with posteriorly directed force; a palpable clunk of subluxation/dislocation is felt - a positive sign indicates an unstable hip.
- Limited hip abduction (most reliable sign after early infancy)
- Asymmetric skin folds (unreliable alone)
Infants (6-18 months)
- Shortened extremity, limited passive abduction
- Galeazzi sign: Apparent femoral shortening when hips and knees flexed
- Delayed ossification on X-ray; lateral and proximal displacement of femoral head
Walking-age children
- Trendelenburg gait - waddling, lurching toward the affected side
- Difficulty abducting the hip during diaper changes
- Bilateral dislocation may appear symmetrically abnormal and be missed
Adolescents and adults
- Exercise-induced hip pain
- Pain from degenerative arthritis (late complication)
Investigations
Ultrasound (first-line in infants < 6 months)
- High-frequency linear probe; coronal view with hip flexed and abducted
- Graf classification based on alpha (α) and beta (β) angles:
- α angle (acetabular roof angle): Normal ≥ 60°
- β angle (inclination line): Normal < 55°
- Graf I = normal; II = immature/mild dysplasia; III/IV = subluxed/dislocated
- Dynamic stress views assess stability
- Preferred over X-ray in early infancy (femoral head is cartilaginous)
Radiograph (useful from ~4-6 months when ossification begins)
- Hilgenreiner line (horizontal through triradiate cartilage)
- Perkins line (vertical through lateral acetabulum)
- Femoral head should lie in the lower-inner quadrant of these intersecting lines
- Shenton's line continuity
- Acetabular index: Normal < 30° at birth, < 25° by 1 year
- Center-edge angle (reliable only after age 5)
CT/MRI
- Used for pre-operative planning or to assess reduction quality after surgery
- MRI preferred to avoid radiation in young children
Treatment (Age-Based)
Newborn - 6 months: Pavlik Harness (first-line)
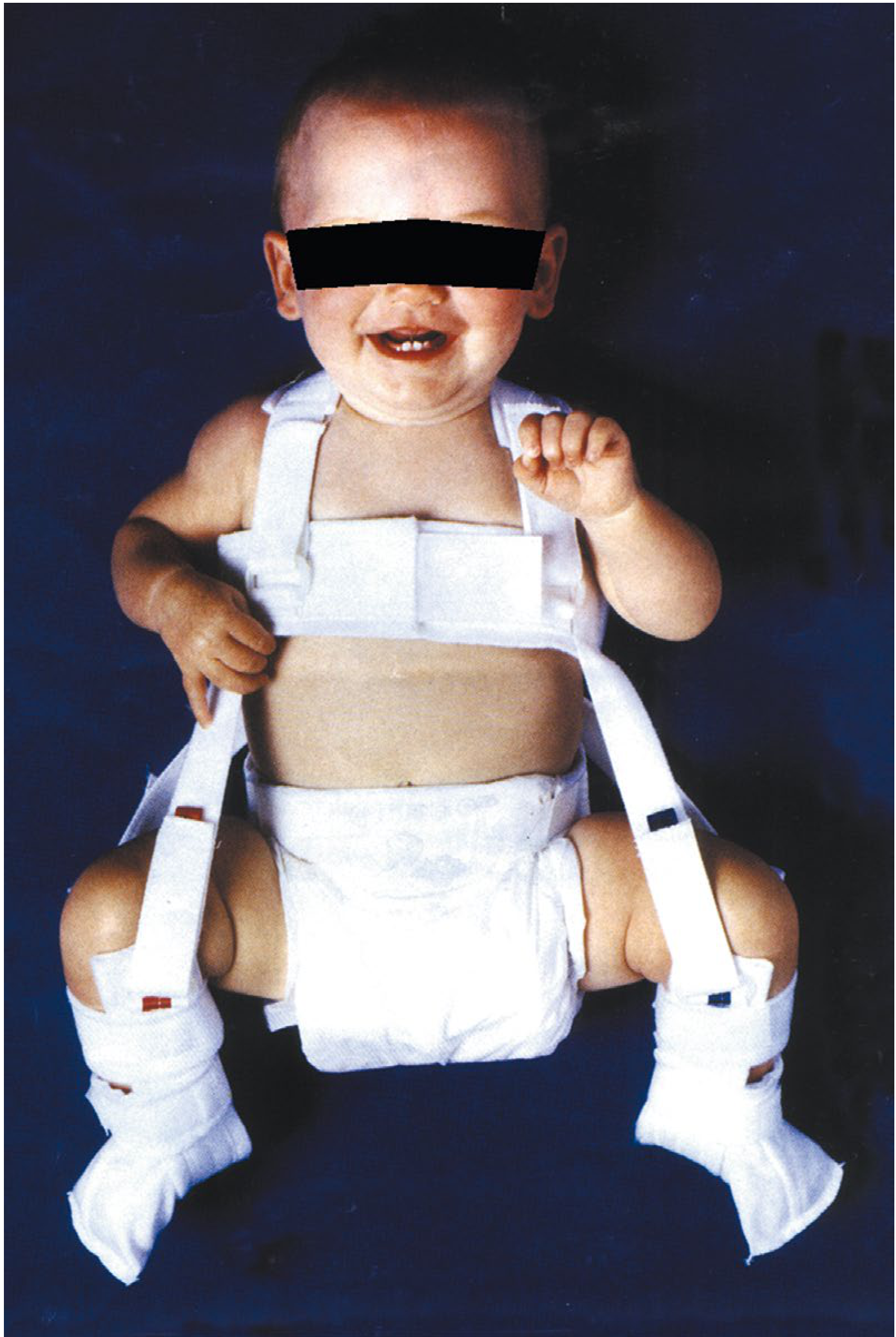
- Worn full-time (23 hours/day) initially, monitored with ultrasound every 2-4 weeks
- Success rate ~85-95% for reducible hips
- Contraindications: teratologic dislocations, fixed contractures, irreducible hips
- Complications: femoral nerve palsy (excessive flexion), osteonecrosis (excessive forced abduction)
- The Tübingen brace is an alternative with similar efficacy
Infant (6-18 months): Closed or Open Reduction
- Pavlik harness success drops sharply after crawling age
- Preoperative traction (2-4 weeks) to bring the femoral head closer to the acetabulum
- Adductor tenotomy to release contracture
- Closed reduction under general anesthesia with arthrogram confirmation, followed by hip spica cast
- Open reduction if closed reduction fails - medial or anterior approach
- Femoral shortening osteotomy may be needed for high dislocations to reduce neurovascular tension
Toddler (18-36 months) and Child (3-8 years)
- Open reduction is almost always required
- Combined with femoral osteotomy (to correct coxa valga/anteversion) and pelvic osteotomy (to redirect or augment the acetabulum)
- Common pelvic procedures: Salter osteotomy, Pemberton acetabuloplasty, Dega osteotomy
Older child/Adolescent/Adult (> 8 years)
- Surgical options more complex; outcomes less predictable
- Periacetabular osteotomy (PAO/Bernese) for symptomatic dysplasia without arthritis
- Total hip arthroplasty for end-stage osteoarthritis secondary to DDH
Complications
| Complication | Notes |
|---|---|
| Avascular necrosis (AVN) of femoral head | Most serious complication of treatment; caused by excessive abduction or forceful reduction |
| Redislocation | After conservative or surgical treatment |
| Residual acetabular dysplasia | Even after successful reduction; long-term surveillance needed |
| Leg length discrepancy | Persistent or secondary to treatment |
| Osteoarthritis | Late consequence of untreated/undertreated DDH |
Screening Guidelines
- AAP (USA): Routine clinical screening of all newborns; ultrasound for positive exam or risk factors (breech, family history)
- UK (NIPE): Hip examination at birth and 6-8 weeks; ultrasound for at-risk infants
- Universal ultrasound screening is practiced in some countries (e.g., Germany, Austria) but evidence for universal vs. selective screening remains mixed - some studies show earlier treatment and fewer surgeries with universal screening, while others show increased unnecessary referrals
Recent Evidence
Create a DDH screening and treatment decision algorithm flowchart
A detailed clinical flowchart titled "DDH Screening and Treatment Decision Algorithm". The flowchart should have a clean white background with professional medical styling. Use color-coded boxes: blue for screening/assessment steps, green for normal/conservative outcomes, orange for interventions, red for surgical options. Flow starts at top with "NEWBORN - Clinical Hip Screening (Ortolani & Barlow Tests)" box. Branch 1: "NEGATIVE exam + No risk factors" → "Routine follow-up at 6 weeks" → "Normal at 6 weeks" → "Discharge / routine care" Branch 2: "NEGATIVE exam + Risk factors present" (risk factors listed: breech, female, family history, firstborn, oligohydramnios) → "Hip Ultrasound at 6 weeks" Branch 3: "POSITIVE exam (Ortolani/Barlow)" → "Hip Ultrasound immediately or at 6 weeks" Ultrasound result branches using Graf classification: - "Graf I (α ≥ 60°) - Normal" → "No treatment, re-examine at 3 months" - "Graf IIa (α 50-59°, age < 3 months) - Physiologically immature" → "Repeat USS at 6 weeks" - "Graf IIb (α 50-59°, age > 3 months) - Dysplastic" → "Pavlik Harness" - "Graf IIc/D (α 43-49°) - Subluxed" → "Pavlik Harness" - "Graf III/IV (α < 43°) - Dislocated" → "Immediate Pavlik Harness" Pavlik Harness branch: - "Hip reduced on USS at 3-4 weeks?" - YES → "Continue harness until α ≥ 60°, then wean" - NO → "Discontinue Pavlik → Proceed to closed/open reduction" Age-based treatment column on the right side: - "Age 0-6 months: Pavlik Harness (first line)" - "Age 6-18 months: Closed Reduction + Hip Spica Cast (± adductor tenotomy, preop traction)" - "Age 18 months - 3 years: Open Reduction ± Femoral Osteotomy + Spica Cast" - "Age 3-8 years: Open Reduction + Femoral + Pelvic Osteotomy (Salter/Pemberton/Dega)" - "Age >8 years / Adult: Periacetabular Osteotomy (PAO) or Total Hip Arthroplasty" Footer warning box in red: "Complications to monitor: Avascular Necrosis (AVN), Redislocation, Residual Dysplasia" All boxes connected with clear directional arrows. Legend in corner. Professional medical textbook style.
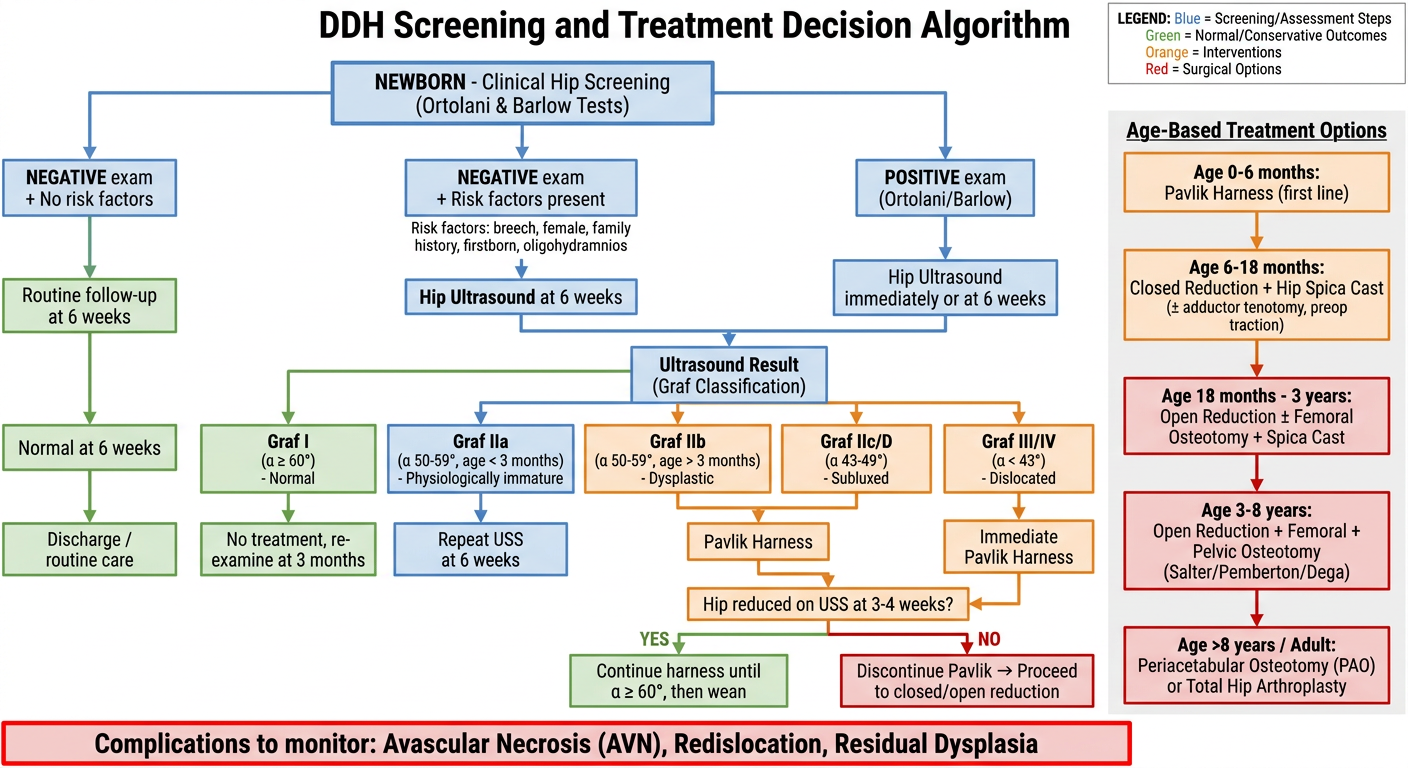
- Starting from newborn clinical examination with Ortolani and Barlow tests
- Three branches: normal exam without risk factors, normal exam with risk factors, and positive exam
- Ultrasound (Graf classification) drives the next decision point
- Graf I → routine follow-up, no treatment
- Graf IIa (< 3 months) → watchful waiting with repeat USS
- Graf IIb/IIc/D → Pavlik harness
- Graf III/IV → immediate Pavlik harness with close monitoring
- Pavlik harness response at 3-4 weeks determines continuation vs. escalation to reduction
- 0-6 months: Pavlik harness
- 6-18 months: closed reduction + hip spica cast
- 18 months - 3 years: open reduction ± femoral osteotomy
- 3-8 years: triple procedure (open reduction + femoral + pelvic osteotomy)
- > 8 years/adult: PAO or total hip arthroplasty
- Red alert box for AVN, redislocation, and residual dysplasia - the three most clinically significant risks to track throughout treatment.
Take all the references from Campbell and make a ppt with extra pictures and flow charts on Ddh
A medical anatomy diagram showing the hip joint cross-section comparing normal hip versus DDH (Developmental Dysplasia of the Hip). Left side shows normal hip: femoral head fully seated in deep acetabulum, labeled "Normal Hip - Femoral head, Acetabulum, Labrum, Ligamentum teres". Right side shows three stages of DDH: (1) Subluxation - partial displacement, (2) Dislocation - complete displacement, (3) Chronic dislocation - with secondary changes including hypertrophied limbus, elongated ligamentum teres, psoas obstruction, coxa valga. Use clean anatomical illustration style with blue and white tones, clear labels, professional medical textbook quality.
A medical education infographic showing DDH risk factors arranged as a visual wheel or mind map. Center circle reads "DDH Risk Factors". Surrounding sections in different colors: Female sex (pink, 4-5x higher risk), Breech presentation (orange, especially extended breech), Firstborn child (yellow, tight primigravid uterus), Family history (green, 10% recurrence risk), Oligohydramnios (blue, restricts fetal movement), Left hip (purple, LOA fetal position), Swaddling (red, legs-together position). Additional box: Associated conditions - congenital torticollis 8%, metatarsus adductus, talipes calcaneovalgus. Clean professional medical infographic style with icons.
A medical diagram showing the Graf Ultrasound Classification of DDH. Four labeled ultrasound diagrams side by side on white background showing coronal hip views: Graf Type I (alpha angle ≥60°, normal, deep acetabulum, femoral head well covered), Graf Type IIa/b (alpha 50-59°, mildly dysplastic, shallow acetabulum), Graf Type IIc/D (alpha 43-49°, subluxed, femoral head partially outside acetabulum), Graf Type III/IV (alpha <43°, dislocated, femoral head completely outside acetabulum). Each type has a small colored indicator: green for I, yellow for IIa, orange for IIb/IIc, red for III/IV. Alpha and beta angle lines clearly drawn. Clean medical illustration style.
Ppt
Medical anatomy cross-section diagram comparing normal hip vs DDH stages. Left panel: Normal hip with deep acetabulum, femoral head fully seated, labrum intact, labeled clearly. Right panel shows 3 stages: (1) Subluxation - partial displacement with stretched capsule, (2) Dislocation - femoral head fully out, (3) Chronic DDH - hypertrophied limbus, elongated ligamentum teres, psoas obstruction, coxa valga, shallow acetabulum. Clean medical textbook illustration, blue and cream tones, professional labels.
Medical infographic showing DDH risk factors as a colorful radial diagram. Center: "DDH Risk Factors". Six color-coded segments: Female sex (pink icon, 4-5x risk), Breech presentation (orange icon), Firstborn child (yellow icon), Family history (green, 10% risk), Oligohydramnios (blue icon), Swaddling (red icon). Bottom row: Associated conditions box listing congenital torticollis 8%, metatarsus adductus, talipes calcaneovalgus. Clean professional medical style, white background, bold icons.
Medical diagram: Graf Ultrasound Classification of DDH. Four panels showing coronal ultrasound hip views with alpha angle lines: Type I (alpha ≥60°, green, NORMAL - deep bony acetabulum), Type IIa/b (alpha 50-59°, yellow, DYSPLASTIC - shallow acetabulum), Type IIc/D (alpha 43-49°, orange, SUBLUXED - head partially displaced), Type III/IV (alpha <43°, red, DISLOCATED - head fully displaced). Baseline, acetabular roof line, and inclination line drawn on each. Color severity scale bar at bottom. Clean medical illustration, white background.
Take all the references from Campbell and make a ppt with extra pictures and flow charts on Ddh
Medical anatomy cross-section diagram comparing normal hip vs DDH stages on white background. Left panel labeled "Normal Hip": deep acetabulum, femoral head fully seated, intact labrum, ligamentum teres, clear anatomical labels. Right panel shows 3 DDH stages side by side: Stage 1 Subluxation (partial head displacement, stretched capsule), Stage 2 Dislocation (femoral head fully displaced), Stage 3 Chronic DDH (hypertrophied limbus, elongated ligamentum teres, shallow acetabulum, coxa valga). Professional medical illustration blue and cream color scheme, clean bold labels.
Medical infographic on white background: DDH Graf Ultrasound Classification. Four labeled boxes arranged left to right with color severity coding. Box 1 (green): Type I - alpha angle greater than 60 degrees, Normal hip, deep bony acetabulum, femoral head fully covered. Box 2 (yellow): Type IIa/b - alpha 50-59 degrees, Dysplastic, shallow acetabulum, physiologically immature under 3 months. Box 3 (orange): Type IIc/D - alpha 43-49 degrees, Subluxed, femoral head partially outside acetabulum. Box 4 (red): Type III/IV - alpha less than 43 degrees, Dislocated, femoral head completely outside acetabulum. Each box shows a simple line drawing of the hip cross-section with the alpha angle marked. Color bar severity scale at bottom from green to red. Clean clinical chart style.
Medical education infographic titled "DDH Risk Factors" on white background. Clean modern design with 6 colored icon boxes arranged in 2 rows of 3. Each box has an icon and text: (1) Blue - Female Sex, 4-5x more common, hormonal ligamentous laxity (2) Orange - Breech Presentation, especially extended breech, abnormal hip flexion forces (3) Yellow - Firstborn Child, tight primigravid uterus, restricted fetal movement (4) Green - Family History, 10% recurrence risk, genetic predisposition (5) Purple - Oligohydramnios, restricted fetal movement, associated postural deformities (6) Red - Leg Swaddling, adduction stress, cultural practices worsen instability. Bottom section: Associated conditions - Congenital Torticollis 8%, Metatarsus Adductus, Talipes Calcaneovalgus. Professional clean style.
andren von rosen line
Andren von Rosen line DDH radiograph measurement technique
https://radiopaedia.org/articles/paediatric-hip-abduction-in…
Andren-von Rosen Line (von Rosen View)
What It Is
The von Rosen View - Technique
| Parameter | Position |
|---|---|
| Patient position | Supine |
| Hip abduction | 45° (some sources say 30°) |
| Foot/leg rotation | 15-20° internal rotation |
| View | Anteroposterior (AP) pelvis |
How to Draw and Interpret the Line
- The line, when extended, passes through or touches the triradiate cartilage (or the lateral sourcil - the superolateral edge of the acetabulum)
- This indicates the femoral head is properly located within the acetabulum
- The line, when extended, passes above and lateral to the acetabulum - pointing toward the anterior superior iliac spine (ASIS) or toward the iliac wing rather than the acetabulum
- This indicates the femoral head is displaced superolaterally out of the socket
Significance
- Most useful when the hip is dislocated AND irreducible - because in reducible dislocations, the abduction and internal rotation positioning of the view often reduces the hip, making the image appear normal (a key limitation)
- The view is particularly helpful when the femoral head is not yet ossified (< 4-6 months), as Hilgenreiner's and Perkins' lines become less reliable in this setting
- Not widely used today compared to ultrasound (Graf method), but still relevant historically and in resource-limited settings
Relationship to Other DDH Lines
| Line/Sign | Reference Structure | What It Detects |
|---|---|---|
| Hilgenreiner's line | Horizontal line through triradiate cartilages | Vertical displacement of femoral head |
| Perkins' line | Vertical through lateral acetabular edge | Lateral displacement |
| Shenton's line | Curve from femoral neck to obturator foramen | Broken = subluxation/dislocation |
| Andren-von Rosen line | Along femoral shaft axis (on abducted-IR view) | Displacement direction - toward ilium = dislocated |
| Acetabular Index | Angle of acetabular roof to Hilgenreiner's line | Degree of acetabular dysplasia (normal < 30° neonate) |
Clinical Limitations
- Reducible hips - the abduction-IR positioning may spontaneously reduce the hip, giving a false negative
- Superseded by ultrasound - the Graf classification via US is now the gold standard in infants under 6 months
- Radiation exposure in neonates - a concern with any X-ray-based screening
- Correct positioning requires experience; poor positioning leads to unreliable results