Inj piroxicam vs inj tramadol vs inj diclofenac vs inj ketorolac in detail
injectable piroxicam vs tramadol vs diclofenac vs ketorolac comparison analgesic pharmacology
Injectable Analgesics: Piroxicam vs Tramadol vs Diclofenac vs Ketorolac - Detailed Comparison
1. DRUG CLASS & MECHANISM OF ACTION
| Drug | Class | Mechanism |
|---|---|---|
| Piroxicam | NSAID (oxicam) | Non-selective COX-1 and COX-2 inhibitor; inhibits prostaglandin synthesis; also inhibits neutrophil chemotaxis and lysosomal enzyme release |
| Tramadol | Atypical centrally-acting analgesic / weak opioid | Dual mechanism: (1) weak mu-opioid receptor (MOR) agonist; (2) inhibits reuptake of serotonin and norepinephrine, potentiating descending inhibitory pain pathways |
| Diclofenac | NSAID (phenylacetic acid derivative) | Preferential COX-2 inhibitor (mild COX-2 selectivity) + inhibits prostaglandin synthesis; also inhibits lipoxygenase pathway and thromboxane synthesis |
| Ketorolac | NSAID (pyrrolizine carboxylic acid) | Potent, non-selective COX-1 > COX-2 inhibitor; the most potent analgesic among parenteral NSAIDs; S-form is the pharmacologically active enantiomer |
2. PHARMACOKINETICS
Piroxicam (Inj)
- Onset: 15-30 min (IM)
- Half-life: ~50 hours (longest of all four - enables once-daily dosing)
- Protein binding: >99%
- Metabolism: Hepatic (CYP2C9); enterohepatic recirculation
- Excretion: Renal and fecal
- Special: Very long t½ means drug accumulation with repeated doses
Tramadol (Inj)
- Onset: 5-10 min (IV), 15-30 min (IM)
- Half-life: ~6 hours (parent drug), ~7.5 hours (active metabolite O-desmethyltramadol / M1)
- Protein binding: ~20%
- Metabolism: Hepatic (CYP2D6 to M1 - 2-4x more potent than parent)
- Excretion: Renal (~90%)
- Bioavailability (oral): 68%
- Special: Racemic mixture - (+) enantiomer = MOR agonism + serotonin reuptake inhibition; (-) enantiomer = norepinephrine reuptake inhibition + α2 agonism
Diclofenac (Inj)
- Onset: ~15-30 min (IM)
- Half-life: ~1-2 hours (short, but tissue t½ is longer - synovial fluid)
- Protein binding: >99%
- Metabolism: Hepatic (CYP2C9 and CYP3A4)
- Excretion: Renal (~65%) and biliary/fecal (~35%)
- Special: Despite short plasma t½, sustained drug levels in synovial fluid explain prolonged clinical effect (6-8 h dosing interval)
Ketorolac (Inj)
- Onset: 30 min (IM), 15-30 min (IV); peak analgesic effect at 2-3 hours
- Half-life: 5-6 hours
- Protein binding: ~99%
- Metabolism: Partial hepatic; ~90% excreted by kidney, 60% unchanged
- Routes available: IV, IM, intranasal, oral, ophthalmic
- Special: Linear pharmacokinetics; bioavailability of IM and oral equals IV bolus
3. DOSAGE (Injectable)
| Drug | Standard Adult Dose | Max Daily Dose | Duration Limit |
|---|---|---|---|
| Piroxicam | 20 mg IM (single dose or once daily) | 20 mg/day | Usually 1-2 days IM; not for prolonged IM use |
| Tramadol | 50-100 mg IM/IV every 4-6 hours | 400 mg/day | Can be used longer term (both acute and chronic) |
| Diclofenac | 75 mg IM once or twice daily | 150 mg/day (IM) | 2 days IM (switch to oral after) |
| Ketorolac | 30-60 mg IM (initial), 15-30 mg IV; then 15-30 mg every 6-8 h | 120 mg/day | Maximum 5 days total |
4. INDICATIONS
| Drug | Primary Indications |
|---|---|
| Piroxicam | Musculoskeletal pain (arthritis, acute gout), mild-to-moderate acute pain, renal colic |
| Tramadol | Moderate-to-severe acute and chronic pain, post-operative pain, neuropathic pain, cancer pain |
| Diclofenac | Musculoskeletal pain, renal/biliary colic, post-operative pain, acute gout, dysmenorrhea, migraine |
| Ketorolac | Moderate-to-severe acute pain requiring "opioid-level" analgesia (post-operative pain, renal colic, trauma); not for chronic pain |
5. ANALGESIC POTENCY
- Ketorolac = strongest analgesic among the NSAIDs; comparable to morphine 10 mg IM for post-operative pain in multiple trials; superior to opioids in some surgical pain models (Cochrane review: 65% pain reduction at 4 h vs 36% for opioids)
- Tramadol = moderate-to-strong centrally acting; less potent than full opioid agonists (10-fold weaker MOR binding vs morphine)
- Diclofenac = moderate analgesic with good anti-inflammatory effect; widely used for inflammatory and musculoskeletal pain
- Piroxicam = moderate analgesic; more valued for anti-inflammatory properties due to very long half-life; not ideal for acute breakthrough pain
6. ADVERSE EFFECTS
Piroxicam
- Highest GI risk among all four (long t½ = prolonged COX-1 inhibition in gut mucosa)
- Peptic ulceration, GI bleeding
- Renal impairment, fluid retention, hypertension
- Photosensitivity (notable - unique among this group)
- Injection site reactions (dermatitis reported)
- Platelet dysfunction (prolonged bleeding time)
- Hepatotoxicity (rare)
Tramadol
- Nausea, vomiting (most common, especially initial doses)
- Dizziness, vertigo, sedation, dry mouth
- Constipation (less severe than full opioids)
- Serotonin syndrome (risk with SSRIs, SNRIs, MAOIs, TCAs, triptans)
- Seizures (dose-related; lower threshold with co-administration of SSRIs, SNRIs, TCAs, neuroleptics)
- Respiratory depression (rare; much less than full opioids)
- Sweating, angioedema
- Dependence/abuse potential (lower than opioids, but recognized)
- Enhanced anticoagulant effect (warfarin)
- No significant anti-inflammatory or antipyretic activity
Diclofenac
- GI: dyspepsia, ulcers, GI bleeding (lower risk than ketorolac or piroxicam)
- Hepatotoxicity - highest among NSAIDs (liver transaminase elevation in ~15%; rare serious hepatitis)
- Cardiovascular: increased CV risk (MI, stroke) with chronic use; highest CV risk among NSAIDs in some meta-analyses
- Renal impairment, fluid retention, edema
- Platelet dysfunction (less vs aspirin/ketorolac)
- Injection site pain (IM can be painful)
- Hypersensitivity reactions
Ketorolac
- Somnolence (6%), dizziness (7%), headache (17%)
- GI pain (13%), dyspepsia (12%), nausea (12%)
- Renal toxicity - most significant concern, especially >5 days use
- Serious GI events (ulceration, perforation, bleeding) - risk increases beyond 5 days
- Bleeding risk (platelet inhibition - COX-1 mediated thromboxane inhibition)
- Pain at injection site (2%)
- Hypersensitivity
- Contraindicated in: renal failure, pre-operative CABG, obstetric analgesia, combination with probenecid (triples AUC, doubles t½)
7. CONTRAINDICATIONS
| Contraindication | Piroxicam | Tramadol | Diclofenac | Ketorolac |
|---|---|---|---|---|
| Renal failure | Yes | Caution (reduce dose) | Yes | Absolute CI |
| Hepatic failure | Yes | Yes (reduce dose) | Yes (especially) | Yes |
| GI ulcer/bleeding | Yes | No | Yes | Yes |
| Asthma (aspirin-sensitive) | Yes | No | Yes | Yes |
| Pregnancy (3rd trimester) | Yes | Caution | Yes | Yes (also CI peripartum) |
| MAO inhibitors | No | Yes - absolute CI | No | No |
| Epilepsy | No | Relative CI (lowers seizure threshold) | No | No |
| Perioperative CABG | Yes | No | Yes | Yes - absolute CI |
| Probenecid | No | No | No | Yes - absolute CI |
8. DRUG INTERACTIONS
Piroxicam
- Other NSAIDs, anticoagulants (increased bleeding)
- Lithium (increased lithium levels)
- Antihypertensives (reduced efficacy)
- Methotrexate (increased toxicity)
Tramadol
- MAO inhibitors - serotonin syndrome, potentially fatal
- SSRIs/SNRIs - serotonin syndrome, seizures
- TCAs - serotonin syndrome
- CNS depressants - additive sedation/respiratory depression
- Warfarin - enhanced anticoagulant effect
- CYP2D6 inhibitors (fluoxetine, paroxetine) - reduce M1 formation, reduce analgesia
- Triptans - serotonin syndrome
Diclofenac
- Anticoagulants (increased bleeding risk)
- Lithium, methotrexate (toxicity)
- Cyclosporine (nephrotoxicity)
- CYP2C9 inducers/inhibitors (alter diclofenac levels)
- Antihypertensives (reduced efficacy)
Ketorolac
- Probenecid - triples ketorolac AUC - absolutely contraindicated
- Other NSAIDs (additive toxicity)
- Anticoagulants (heparin, warfarin) - seriously increased bleeding
- ACE inhibitors/ARBs (acute kidney injury)
- Diuretics (reduced efficacy + renal risk)
9. USE IN SPECIAL POPULATIONS
| Population | Piroxicam | Tramadol | Diclofenac | Ketorolac |
|---|---|---|---|---|
| Elderly | Avoid (long t½, accumulation) | Use lower doses (start 25 mg) | Use with caution | Halve the dose; max 60 mg/day |
| Renal impairment | Avoid | Reduce interval | Avoid | Absolute CI if severe |
| Hepatic impairment | Caution | Reduce dose | Avoid / use with extreme caution | Use caution |
| Pregnancy | Avoid (1st/3rd trimester) | Avoid (neonatal withdrawal) | Avoid 3rd trimester | CI (peripartum, ductus arteriosus) |
| Pediatric | Not recommended | Not for <12 years (risk of seizure) | Not well established parenterally | 2-16 years: single IM/IV dose only |
10. CLINICAL USE COMPARISON SUMMARY
| Feature | Piroxicam | Tramadol | Diclofenac | Ketorolac |
|---|---|---|---|---|
| Duration of use | Short IM course | Acute or chronic | Short IM course (≤2 days) | Maximum 5 days |
| Anti-inflammatory effect | Strong | None | Strong | Moderate |
| Ceiling effect | Yes (NSAID) | No ceiling for opioid component | Yes (NSAID) | Yes (NSAID) |
| Respiratory depression | No | Low risk (vs full opioids) | No | No |
| Addiction potential | None | Low but present | None | None |
| GI risk | High (long t½) | Low | Moderate | High (≥5 days) |
| CV risk | Moderate | Low | High (long-term) | Moderate |
| Renal risk | Moderate | Low | Moderate | High |
| Hepatic risk | Low | Low-moderate | High | Low-moderate |
| Controlled substance | No | Yes (Schedule IV in many countries) | No | No |
| Best for | Inflammatory MSK pain, arthritis flare | Moderate-severe acute/chronic pain | Renal/biliary colic, MSK pain, dysmenorrhea | Post-operative pain, acute severe pain requiring "opioid-level" analgesia |
| Avoid when | Long-term use, elderly, GI disease | MAOIs, seizure disorder, SSRI use | Liver disease, CV disease | >5 days, renal failure, CABG |
11. KEY CLINICAL PEARLS
-
Ketorolac is the only NSAID injectable that is considered equivalent to opioids for acute post-operative pain - but use is strictly limited to 5 days; beyond this, GI and renal toxicity risk rises sharply. - Goodman & Gilman's Pharmacological Basis of Therapeutics
-
Tramadol is the only agent among these four that carries risk of serotonin syndrome and seizures. It requires CYP2D6 for conversion to its active M1 metabolite; poor CYP2D6 metabolizers (some populations) may have reduced analgesic response. - Katzung's Basic and Clinical Pharmacology, 16th Ed
-
Diclofenac carries the highest hepatotoxic risk of the group - transaminase elevations occur in ~15% of patients; frank hepatitis is rare but documented. Its mild COX-2 preference means lower platelet effect compared to ketorolac or piroxicam.
-
Piroxicam's 50-hour half-life is a double-edged sword: convenient for once-daily dosing in oral/chronic use, but in the injectable form, a single IM dose can produce effects lasting 24+ hours. This also means accumulation and prolonged GI/renal toxicity in elderly or renally impaired patients.
-
For renal colic, diclofenac 75 mg IM is the most well-studied and widely recommended NSAID; ketorolac 30 mg IM is a comparable alternative.
-
For post-operative multimodal analgesia, ketorolac is the preferred NSAID injection; it is opioid-sparing and reduces total opioid consumption. Cochrane review evidence shows single-injection ketorolac superior to opioids at 4 h (65% vs 36% achieving ≥50% pain reduction).
Create a clinical decision flowchart: when to choose which analgesic based on indication and patient factors
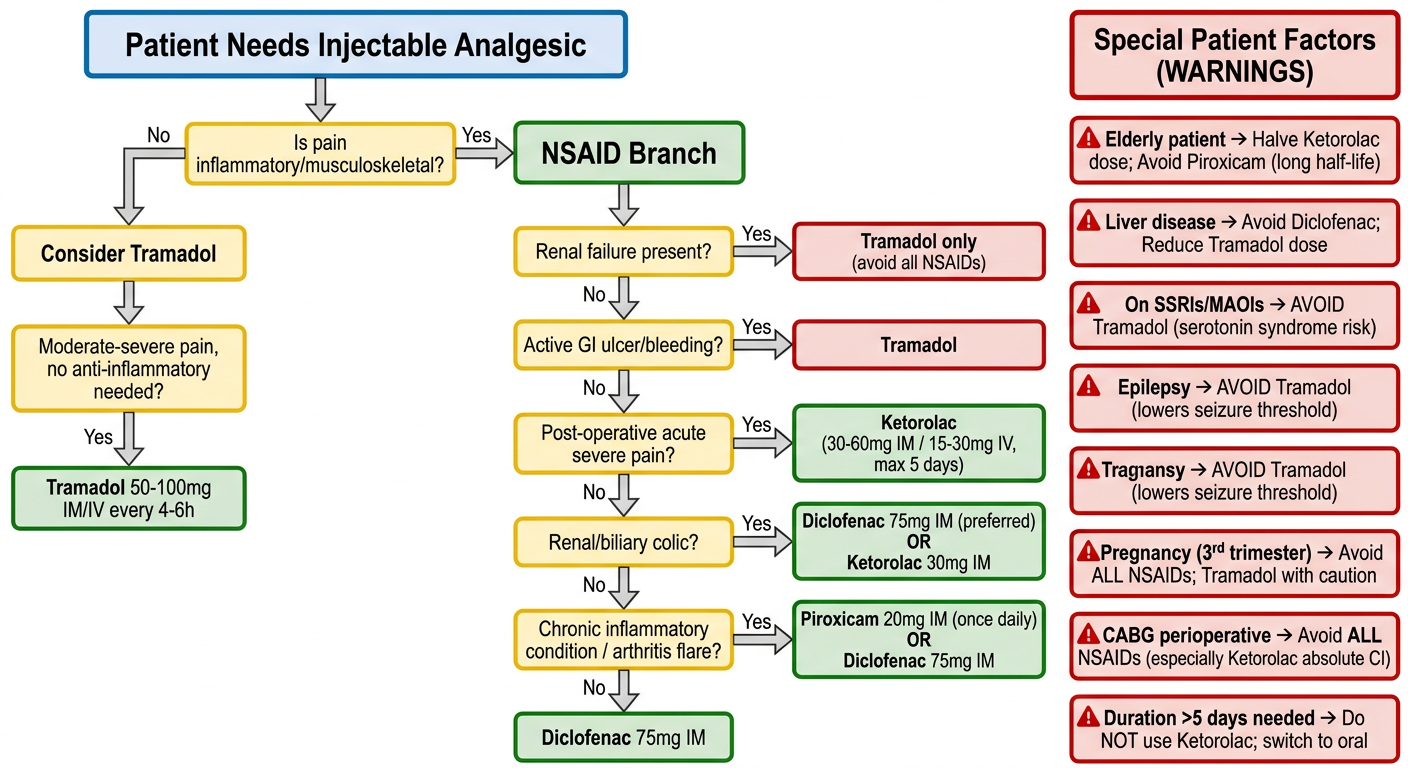
A detailed clinical decision flowchart for choosing between injectable analgesics: Piroxicam, Tramadol, Diclofenac, and Ketorolac. The flowchart starts at the top with "Patient Needs Injectable Analgesic" and branches based on clinical questions. Branch 1: Is pain inflammatory/musculoskeletal? Yes → Go to NSAID branch. No → Consider Tramadol. NSAID Branch asks: Renal failure present? Yes → Tramadol only (avoid all NSAIDs). No → Continue. Next NSAID question: Active GI ulcer/bleeding? Yes → Tramadol. No → Continue. Next: Post-operative acute severe pain? Yes → Ketorolac (30-60mg IM / 15-30mg IV, max 5 days). No → Continue. Next: Renal/biliary colic? Yes → Diclofenac 75mg IM (preferred) OR Ketorolac 30mg IM. No → Continue. Next: Chronic inflammatory condition / arthritis flare? Yes → Piroxicam 20mg IM (once daily) OR Diclofenac 75mg IM. No → Diclofenac 75mg IM. Tramadol Branch: Moderate-severe pain, no anti-inflammatory needed? → Tramadol 50-100mg IM/IV every 4-6h. Special patient factors boxes with red warning labels: - Elderly patient → Halve Ketorolac dose; Avoid Piroxicam (long half-life) - Liver disease → Avoid Diclofenac; Reduce Tramadol dose - On SSRIs/MAOIs → AVOID Tramadol (serotonin syndrome risk) - Epilepsy → AVOID Tramadol (lowers seizure threshold) - Pregnancy (3rd trimester) → Avoid ALL NSAIDs; Tramadol with caution - CABG perioperative → Avoid ALL NSAIDs (especially Ketorolac absolute CI) - Duration >5 days needed → Do NOT use Ketorolac; switch to oral Color coding: Green boxes for safe/preferred choices, Yellow for caution, Red for contraindications. Clean medical diagram style with clear arrows, professional typography, white background.
Decision Algorithm: Choosing the Right Injectable Analgesic
Step 1 - Screen for Universal Contraindications First
- Renal failure → Use Tramadol only (all NSAIDs contraindicated)
- Active GI ulcer/bleeding → Use Tramadol only
- Perioperative CABG → Use Tramadol only (NSAIDs absolutely contraindicated)
- On MAO inhibitors → Avoid Tramadol (fatal serotonin syndrome) → Use NSAID if suitable, or seek specialist input
- Active seizure disorder → Avoid Tramadol (lowers seizure threshold)
Step 2 - Match Indication to Drug
| Clinical Situation | First Choice | Alternative |
|---|---|---|
| Post-operative acute severe pain | Ketorolac 30-60 mg IM / 15-30 mg IV | Tramadol 100 mg IM |
| Renal / biliary colic | Diclofenac 75 mg IM | Ketorolac 30 mg IM |
| Musculoskeletal / joint pain (acute) | Diclofenac 75 mg IM | Piroxicam 20 mg IM |
| Arthritis flare / inflammatory pain | Piroxicam 20 mg IM (long-acting) | Diclofenac 75 mg IM |
| Dysmenorrhea / migraine | Diclofenac 75 mg IM | Ketorolac 30 mg IM |
| Moderate-severe pain, no inflammation | Tramadol 100 mg IM/IV | - |
| Neuropathic pain component | Tramadol (only one with central action) | - |
| Chronic pain (long-term management) | Tramadol | Oral NSAIDs (not parenteral) |
Step 3 - Apply Patient Factor Adjustments
| Patient Factor | Adjustment |
|---|---|
| Age >65 years | Halve Ketorolac dose; avoid Piroxicam (accumulation risk); start Tramadol at 25-50 mg |
| Weight <50 kg | Halve Ketorolac dose |
| Liver disease | Avoid Diclofenac; reduce Tramadol interval; Ketorolac with caution |
| On SSRIs / SNRIs / TCAs | Tramadol risk of serotonin syndrome - use NSAID instead if suitable |
| Epilepsy | Avoid Tramadol; prefer NSAID |
| 3rd trimester pregnancy | Avoid all NSAIDs (ductus arteriosus); Tramadol with caution (neonatal withdrawal) |
| Asthma (aspirin-sensitive) | Avoid all NSAIDs; use Tramadol |
| Cardiovascular disease (chronic) | Avoid Diclofenac long-term; Ketorolac short-term acceptable; Tramadol preferred |
| Need >5 days of analgesia | Never use Ketorolac; switch to oral or use Tramadol |
| On Probenecid | Ketorolac absolutely contraindicated (triples AUC) |
| CYP2D6 poor metabolizer | Tramadol may have reduced efficacy (impaired M1 conversion) |
Quick One-Line Rules
- Ketorolac = best NSAID for acute severe pain, but clock starts ticking at dose 1 (5-day hard limit)
- Diclofenac = go-to for colic and musculoskeletal pain, but watch the liver
- Piroxicam = good for inflammatory/arthritic flares where once-daily IM is convenient; not for acute breakthrough pain
- Tramadol = the only option when all NSAIDs are contraindicated; also the only one with central/neuropathic action