Old mi patient with angioplasty developed sudden shortness of breath
Reading File
search_medical_text
sudden shortness of breath after angioplasty post MI complications dyspnea
search_medical_text
acute pulmonary edema heart failure post myocardial infarction management
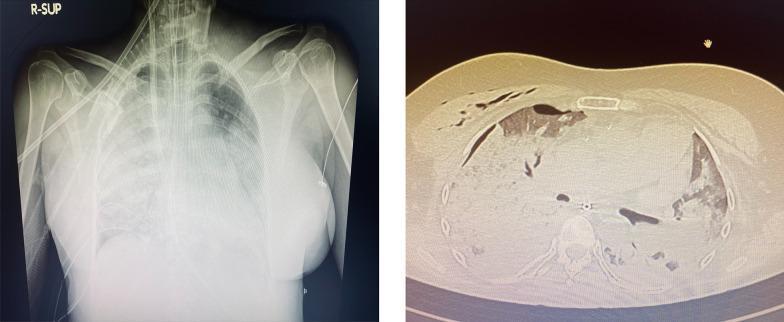
search_medical_image
post MI complications chest X-ray pulmonary edema
GradeResponse
GradeResponse
GradeResponse
Here is a structured clinical approach to this presentation:
Sudden Dyspnea in an Old MI Patient Post-Angioplasty
Key Differentials to Consider
This is a high-acuity presentation. The differential must be approached systematically — cardiac causes dominate given the background.
🔴 Cardiac (Most Likely)
| Cause | Mechanism | Key Features |
|---|---|---|
| Acute LV Failure / Pulmonary Edema | Ischemia, restenosis, or stunned myocardium | Orthopnea, pink frothy sputum, crackles, S3, elevated JVP |
| In-stent Restenosis / Re-occlusion | Recurrent ischemia triggering acute decompensation | Chest pain (may be absent in elderly/diabetics), new ECG changes |
| Ventricular Septal Rupture (VSR) | Mechanical complication of MI | Harsh pansystolic murmur at left sternal border, acute hemodynamic collapse |
| Papillary Muscle Rupture / Acute MR | Ischemic papillary muscle necrosis | Acute pulmonary edema, new loud murmur, hypotension |
| Cardiogenic Shock | Extensive LV dysfunction | Hypotension, cold clammy extremities, oliguria |
| Pericardial Effusion / Tamponade | Post-MI (Dressler's), procedure-related | Beck's triad: hypotension, JVD, muffled heart sounds |
| Arrhythmia (VT/AF) | Ischemic scar re-entry | Palpitations, hemodynamic instability |
According to Harrison's Principles of Internal Medicine (p. 8287), mechanical complications of acute MI — including VSR, papillary muscle/chordal rupture causing severe MR, and ventricular free wall rupture — are important causes of acute cardiogenic pulmonary edema and shock.
🟡 Pulmonary
| Cause | Key Features |
|---|---|
| Pulmonary Embolism | Post-procedure immobility, DVT risk; pleuritic chest pain, tachycardia, hypoxia |
| Pneumothorax | If recent vascular access (subclavian/jugular); unilateral absent breath sounds |
| Pleural Effusion | Accumulation from heart failure or Dressler's syndrome |
🟠 Other
- Contrast-induced pulmonary edema (rare, non-cardiogenic, from ionic contrast)
- Dressler's Syndrome (weeks post-MI): fever, pleuritis, pericarditis
- Anxiety / Hyperventilation (diagnosis of exclusion)
Immediate Assessment
ABC + Vitals → O₂ Saturation, HR, BP (both arms), RR
Rapid Bedside Evaluation
- ECG — new ST changes, arrhythmia, Q waves
- Chest X-Ray — pulmonary vascular congestion, Kerley B lines, cardiomegaly, effusion, pneumothorax
- Bedside Echo (POCUS) — LV function, wall motion abnormalities, effusion, IVC, valvular pathology
- Labs: Troponin (serial), BNP/NT-proBNP, ABG, CBC, BMP, D-dimer (if PE suspected), coagulation profile
- SpO₂ monitoring + IV access
Management Algorithm
Step 1: Stabilize
- Sit patient upright (reduces preload)
- Supplemental O₂ → target SpO₂ >94%
- If severe respiratory failure: NIV (CPAP/BiPAP) → reduces intubation need in acute pulmonary edema
- If cardiogenic shock: avoid aggressive diuresis; prepare for vasopressors + urgent revascularization
Step 2: Treat the Underlying Cause
If Acute LV Failure / Pulmonary Edema:
- IV Furosemide 40–80 mg (or double home dose)
- IV Nitrates (GTN infusion) if SBP >90 mmHg — rapid preload and afterload reduction
- Morphine (use cautiously — may cause respiratory depression)
- Inotropes (Dobutamine) if low output state
If Re-occlusion / In-stent Restenosis:
- Urgent cardiology consult → repeat coronary angiography ± PCI
- Ensure dual antiplatelet therapy compliance
- IV heparin if thrombus suspected
If Mechanical Complication (VSR / Acute MR):
- ICU level care immediately
- IABP (Intra-aortic Balloon Pump) for hemodynamic support
- Emergency surgical repair is definitive treatment
If PE suspected:
- CTPA to confirm
- Anticoagulation: LMWH / UFH → thrombolysis if massive PE with hemodynamic instability
If Tamponade:
- Emergency pericardiocentesis
Red Flag Signs Requiring Immediate ICU Transfer
- SpO₂ <90% despite O₂
- SBP <90 mmHg
- New loud cardiac murmur
- Altered consciousness
- Worsening despite initial therapy
Bottom line: In an elderly post-MI patient who has had angioplasty, sudden dyspnea must be treated as a cardiac emergency until proven otherwise. The most common causes are acute LV failure/pulmonary edema (from re-ischemia or restenosis) and mechanical complications of MI. Simultaneous stabilization and rapid workup (ECG, echo, CXR, troponin, BNP) are the priority.
This is a shared conversation. Sign in to Orris to start your own chat.