Old mi patient with angioplasty developed sudden shortness of breath
Reading File
search_medical_text
sudden shortness of breath after angioplasty PCI complications
search_medical_text
post MI heart failure pulmonary edema acute dyspnea management
search_medical_image
post MI complications pulmonary edema chest X-ray
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive clinical approach to this presentation:
Sudden Dyspnea in a Post-MI Patient After Angioplasty
Immediate Priority: Life-Threatening Differentials First
This is a medical emergency until proven otherwise. The key differentials must be worked through systematically.
Differential Diagnosis
1. Acute Heart Failure / Cardiogenic Pulmonary Edema (Most Common)
- Post-MI LV dysfunction (systolic or diastolic) is the leading cause
- Elevated LVEDP → pulmonary venous congestion → alveolar flooding
- Clue: BNP/NT-proBNP markedly elevated; CXR with bilateral perihilar opacities, Kerley B lines
- Can occur even after successful PCI if significant myocardium was lost
2. Re-occlusion / Stent Thrombosis (Urgent)
- Acute in-stent thrombosis (especially if anti-platelet therapy was missed/inadequate)
- Leads to recurrent ischemia → acute LV failure → pulmonary edema
- Clue: New ST changes on ECG, chest pain, rising troponin
3. Mechanical Complications of MI
| Complication | Timing | Features |
|---|---|---|
| Papillary muscle rupture (acute MR) | 2–7 days | Sudden pulmonary edema, new harsh systolic murmur |
| VSD (ventricular septal defect) | 3–5 days | Biventricular failure, new holosystolic murmur at sternal border |
| Free wall rupture | 1–5 days | Sudden hemodynamic collapse, tamponade |
| LV aneurysm | Weeks later | Progressive HF, persistent ST elevation |
4. Pulmonary Embolism
- Post-procedural immobility is a risk factor
- Clue: Tachycardia, pleuritic chest pain, hypoxia disproportionate to CXR findings, RV strain on ECG (S1Q3T3)
5. Pericardial Effusion / Tamponade
- Can follow PCI if coronary perforation occurred
- Clue: Hypotension, muffled heart sounds, JVD (Beck's triad), electrical alternans on ECG
6. Pneumothorax
- If central venous access was obtained during the procedure
- Clue: Decreased breath sounds unilaterally, tracheal deviation (tension)
7. Contrast-Induced Pulmonary Edema / Allergic Reaction
- Rare; from iodinated contrast used during catheterization
Immediate Workup
| Investigation | Purpose |
|---|---|
| ECG | ST changes (re-occlusion, STEMI), RV strain (PE), arrhythmia |
| CXR | Pulmonary edema pattern, pneumothorax, pleural effusion |
| ABG / SpO2 | Degree of hypoxia, ventilatory status |
| Bedside Echo (POCUS) | LV/RV function, wall motion, pericardial effusion, valvular lesion, septal defect |
| BNP/NT-proBNP | Differentiates cardiac from non-cardiac cause |
| Troponin (serial) | Rising = re-infarction or stent thrombosis |
| CBC, BMP, Coags | Baseline, electrolytes, renal function |
| D-dimer ± CTPA | If PE suspected |
Initial Stabilization
- Oxygen — titrate to SpO2 >94%; escalate to NIV (CPAP/BiPAP) early in cardiogenic pulmonary edema
- IV access + monitoring — continuous ECG, pulse oximetry, BP
- Upright positioning
- IV Furosemide — 40–80 mg IV if cardiogenic pulmonary edema suspected (reduces preload)
- Nitrates — IV nitroglycerin for afterload/preload reduction if SBP >90 mmHg
- Do NOT delay echo — critical for identifying mechanical complications
If Stent Thrombosis/Re-occlusion Suspected:
- Emergency repeat coronary angiography + PCI
- Ensure dual antiplatelet therapy (aspirin + P2Y12 inhibitor) is on board
- Consider GP IIb/IIIa inhibitor or anticoagulation per cath lab protocol
If Mechanical Complication (VSD/Papillary Rupture):
- Urgent cardiac surgery consultation
- IABP (intra-aortic balloon pump) as bridge to surgery
- Avoid vasodilators in free wall rupture/tamponade
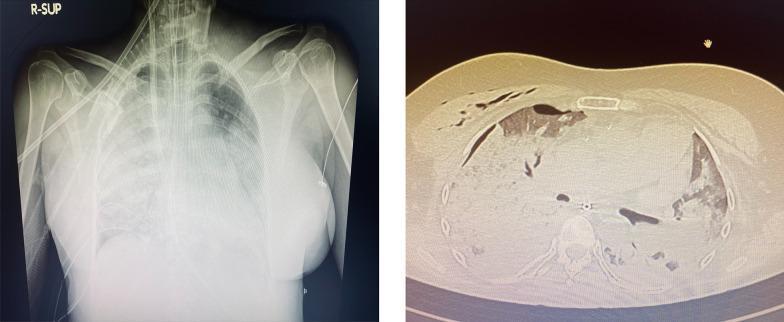
Key Imaging
Post-cardiac surgery / post-PCI pulmonary complications on imaging — bilateral opacities consistent with pulmonary edema:
Bottom Line
Acute dyspnea in a post-MI post-angioplasty patient = emergency echo + ECG NOW.The most common cause is cardiogenic pulmonary edema from LV dysfunction, but stent thrombosis and mechanical MI complications (papillary rupture, VSD) must be excluded urgently — they are rapidly fatal without surgical intervention.
(Harrison's Principles of Internal Medicine, 21st Ed., pp. 7616, 8301)
This is a shared conversation. Sign in to Orris to start your own chat.