Laboratory diagnosis of myocardial infarction pathology
Reading File
Finding Sources
Finding Sources
Searching PubMed
"myocardial infarction" AND "cardiac biomarkers" AND "diagnosis"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I now have extensive, high-quality content from multiple authoritative textbooks. Let me compose the comprehensive answer.
Laboratory Diagnosis of Myocardial Infarction
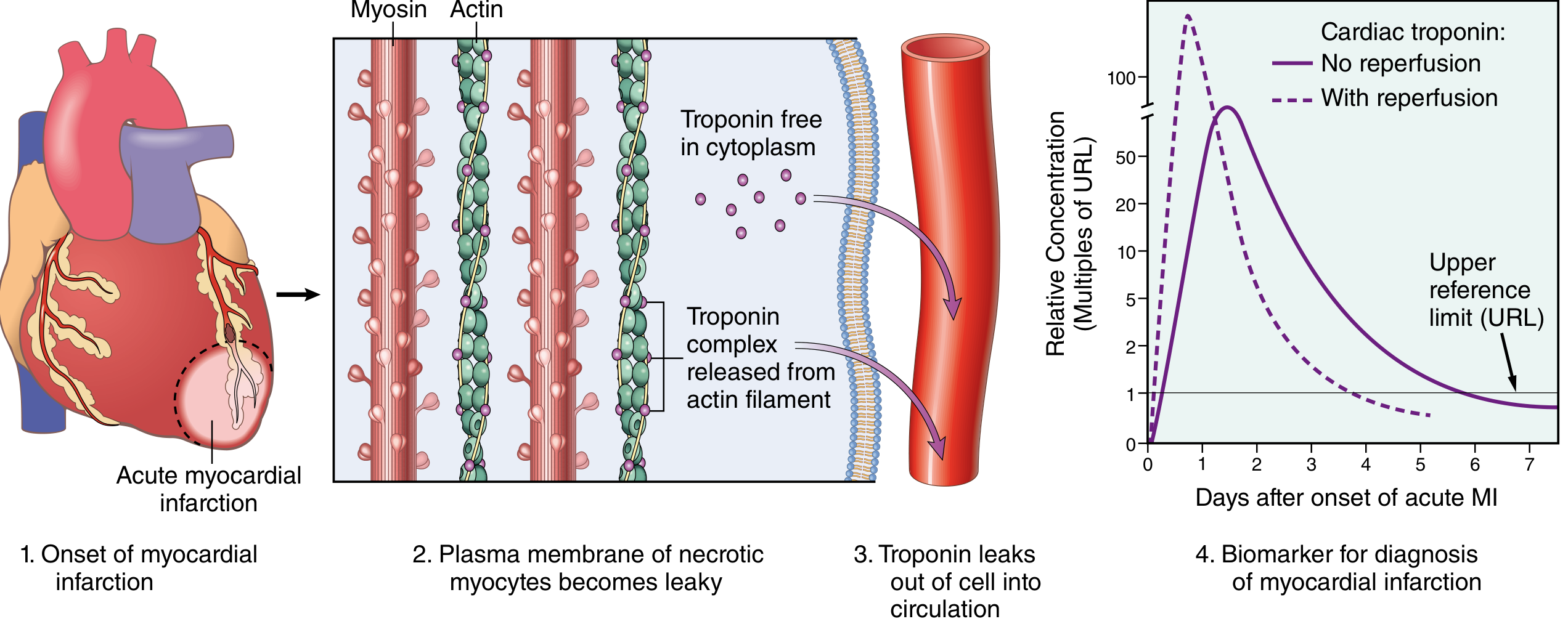
MI is diagnosed by the combination of clinical symptoms, characteristic ECG changes, and - most importantly - laboratory detection of myocardial proteins that leak into the plasma when cardiomyocyte membranes are disrupted.
The Core Principle
When myocardial cells undergo ischemic necrosis, their plasma membranes become leaky and release normally intracellular proteins into the circulation. Measuring these proteins - and critically, their rise and fall over time - is the biochemical cornerstone of MI diagnosis.
Universal Diagnostic Criteria (Fourth Universal Definition of MI)
The diagnosis of acute MI requires a rise and/or fall of cardiac biomarkers (preferably troponin), with at least one value above the 99th percentile of the upper reference limit (URL), combined with at least one of:
- Symptoms of myocardial ischemia
- New ischemic ECG changes (new ST changes, new LBBB)
- Development of pathologic Q waves
- Imaging evidence of new loss of viable myocardium or new regional wall motion abnormality
- Identification of a coronary thrombus on angiography
For special settings, modified thresholds apply:
- PCI-related MI (Type 4a): biomarkers >3x the 99th percentile URL
- CABG-related MI (Type 5): biomarkers >5x the 99th percentile URL
- (Symptom to Diagnosis, 4th Ed., Table 9-6)
Biomarkers in Detail
1. Cardiac Troponins (cTnI and cTnT) - Gold Standard
Troponins are regulatory proteins of the sarcomere complex. Both troponin I (TnI) and troponin T (TnT) have cardiac-specific isoforms not expressed in adult skeletal muscle, giving them near-absolute myocardial tissue specificity.
| Parameter | Value |
|---|---|
| Appears in blood | 2-4 hours after MI onset |
| Peaks | ~48 hours |
| Returns to normal | 7-10 days (TnI), up to 14 days (TnT) |
| With reperfusion | Earlier, higher peak due to rapid washout |
Key advantage: Because troponin levels remain elevated for 7-10 days, an MI can be diagnosed long after CK-MB has already returned to normal (e.g., late-presenting patients).
- (Robbins & Kumar Basic Pathology, p. 359)
"Troponin leak" (low-level elevation) can occur without MI in:
- Congestive heart failure (acute and chronic)
- Pulmonary embolism / severe pulmonary hypertension
- Renal failure
- Sepsis, critically ill states
- Myocarditis, pericarditis
- Hypertension, hypertrophic cardiomyopathy
- Aortic valve disease
- Acute neurological events (CVA, subarachnoid hemorrhage)
- Rhabdomyolysis, drug toxicity (adriamycin, 5-FU, herceptin)
- Hypothyroidism, amyloidosis
- Burns (>30% BSA)
- (Tietz Textbook of Laboratory Medicine, 7th ed., Box 48.1)
These elevations do not follow the typical rise-fall-rise kinetic pattern of MI, so serial measurements at 0h, 3h, and 6h are used to differentiate them.
2. High-Sensitivity Cardiac Troponin (hs-cTn) Assays
Modern hs-cTn assays detect concentrations below the 99th percentile URL in healthy individuals, allowing:
- Detection of MI within 1-2 hours of presentation
- Rapid rule-out protocols (0h/1h or 0h/2h algorithms): a very low baseline hs-cTn with minimal absolute delta change at 1-2 hours effectively excludes MI
- Improved risk stratification and secondary/primary prevention work-up
- (Tietz Textbook of Laboratory Medicine, 7th ed., pp. 1768-1769)
3. CK-MB (Creatine Kinase MB Isoform)
CK exists as three isoenzymes: MM (skeletal muscle), BB (brain), and MB (cardiac muscle). CK-MB makes up ~20% of total CK in myocardium, but is also present in small amounts in skeletal muscle - giving it lower specificity than troponin.
| Parameter | Value |
|---|---|
| Appears in blood | 2-4 hours after MI |
| Peaks | 24-48 hours |
| Returns to normal | ~72 hours (3 days) |
CK-MB is no longer recommended as the primary biomarker for initial MI diagnosis because it lacks the specificity of troponin. It is still used for:
- Re-infarction detection: Because CK-MB normalizes within 72 hours, a new rise in CK-MB after return to normal strongly suggests re-infarction (troponin would still be elevated from the first event and harder to interpret)
- Monitoring infarct size
- (Washington Manual of Medical Therapeutics; Robbins & Kumar Basic Pathology, p. 359)
4. Myoglobin
Myoglobin is a small heme-containing protein in both cardiac and skeletal muscle.
| Parameter | Value |
|---|---|
| Appears in blood | 1-3 hours (earliest of all markers) |
| Peaks | ~6-9 hours |
| Returns to normal | 24-36 hours |
Advantage: Earliest marker - useful for very early rule-out.
Disadvantage: Not cardiac-specific (also released from skeletal muscle injury), so it has low specificity. Largely replaced by hs-cTn in modern practice.
5. Lactate Dehydrogenase (LDH) - Historical
LDH (specifically the LDH-1 isoform, predominantly cardiac) was used historically when patients presented late. It rises after 24 hours, peaks at 3-6 days, and remains elevated for up to 14 days. It has been largely abandoned in favor of the extended troponin window.
Comparative Kinetics Summary
| Biomarker | Rise | Peak | Normalize | Cardiac Specificity |
|---|---|---|---|---|
| hs-cTnI/T | 1-2 h | 24-48 h | 7-14 days | Very high |
| cTnI/T (conventional) | 2-4 h | 48 h | 7-10 days | Very high |
| CK-MB | 2-4 h | 24-48 h | ~72 h | Moderate |
| Myoglobin | 1-3 h | 6-9 h | 24-36 h | Low |
| LDH | 24 h | 3-6 days | 14 days | Low (historical) |
Types of MI - Classification Relevant to Lab Interpretation
| Type | Definition | Lab Interpretation |
|---|---|---|
| Type 1 | Spontaneous MI due to atherothrombotic plaque rupture | Classic rise/fall of troponin |
| Type 2 | Supply-demand mismatch (e.g., anemia, arrhythmia, spasm) | Elevated troponin with rising/falling pattern; no plaque rupture |
| Type 3 | Sudden cardiac death before biomarkers drawn | Post-mortem/ECG diagnosis |
| Type 4a | Post-PCI (>3x URL) | Threshold-based |
| Type 5 | Post-CABG (>5x URL) | Threshold-based |
(Symptom to Diagnosis, 4th Ed.)
STEMI vs NSTEMI - Lab Role
- STEMI: Diagnosis and initiation of reperfusion therapy is based on ECG criteria alone - labs confirm but do not delay treatment.
- NSTEMI: The diagnosis depends on biomarkers (elevated troponin without ST elevation), making the lab result essential to distinguishing NSTEMI from unstable angina (UA), which has no biomarker elevation.
(Robbins & Kumar Basic Pathology, p. 359; Tietz, 7th ed.)
Other Lab Investigations (Ancillary)
Beyond biomarkers, the following support the workup:
- CBC: May show leukocytosis (inflammatory response to necrosis), anemia
- BMP/Electrolytes: Hypokalemia/hypomagnesemia predispose to arrhythmias
- Glucose/HbA1c: Hyperglycemia is a poor prognostic sign
- Lipid panel (fasting): Risk stratification; LDL target-setting for therapy
- BNP/NT-proBNP: Elevated in pump failure complicating MI; reflect hemodynamic stress and assist in diagnosing concomitant heart failure
- Coagulation studies: Relevant before thrombolytic or PCI therapy
- Renal function: Important before contrast for angiography; also affects drug dosing
Key Practical Points
- Serial sampling is mandatory - a single troponin value cannot distinguish acute MI from chronic elevation. The rise-and-fall kinetic pattern is diagnostic.
- hs-cTn allows 0h/1h or 0h/2h rapid rule-out/rule-in algorithms in the ED, dramatically cutting time to diagnosis.
- No biomarker is 100% specific for ischemic MI - clinical context and ECG always accompany lab results.
- About 25% of MIs are "silent" (particularly in diabetics due to autonomic neuropathy), where lab tests may be the only clue.
- Reperfusion affects kinetics: Successful reperfusion (thrombolysis, PCI) causes an earlier, higher, sharper peak (washout effect) - this "reperfusion peak" can be used to monitor treatment effectiveness.
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, 10th ed. (pp. 516-517)
- Robbins & Kumar Basic Pathology (pp. 358-360)
- Tietz Textbook of Laboratory Medicine, 7th ed. (Chapter 48: Cardiac Function, pp. 1768-1776)
- Symptom to Diagnosis: An Evidence-Based Guide, 4th ed. (Table 9-6)
- Washington Manual of Medical Therapeutics
Recent evidence (2025-2026): A 2026 systematic review (PMID 41500560) on biomarkers in Type 2 MI further supports troponin-based approaches but highlights that the prognostic value of specific biomarkers in Type 2 MI remains an active area of investigation.
AST/SGOT means what in diagnosis of MI
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
I have sufficient context. The textbook library doesn't have a dedicated passage on AST/SGOT in MI (it's been fully replaced and isn't covered in detail in modern editions), so I'll answer from well-established knowledge supplemented by what the textbooks do say about the historical enzyme era.
AST / SGOT in the Diagnosis of MI
What is AST/SGOT?
AST (Aspartate Aminotransferase) = SGOT (Serum Glutamic-Oxaloacetic Transaminase) - these are two names for exactly the same enzyme. "SGOT" is the older name; "AST" is the current standard name.
Historical Role in MI Diagnosis
AST was the very first serum enzyme used to diagnose MI, introduced in 1954 by LaMue and Wroblewski, predating CK-MB and troponin by decades. At the time it was a major advance because it gave the first biochemical proof that myocardial necrosis had occurred.
Kinetics of AST in MI:
| Parameter | Value |
|---|---|
| Rises above normal | 6-8 hours after onset |
| Peaks | 24-48 hours |
| Returns to normal | 3-4 days (72-96 hours) |
The pattern was useful in its day - a rise and fall over 3-4 days was consistent with acute MI.
Why AST Was Abandoned
AST has very poor cardiac specificity - it is present in large quantities in many other tissues:
- Liver (hepatocytes - most prominently)
- Skeletal muscle
- Red blood cells
- Kidney
- Brain
- Lung
- Pancreas
This means AST rises in many non-cardiac conditions that can coexist with or mimic MI:
- Hepatitis, liver disease, congestive hepatopathy (liver congestion in right heart failure)
- Skeletal muscle injury, intramuscular injections
- Hemolysis
- Pulmonary embolism
- Pancreatitis
- Vigorous exercise
A patient with acute MI and concomitant liver congestion (cardiogenic shock) would have an ambiguous AST elevation - is it from the heart or the liver? This is exactly the problem.
The Enzyme "Ladder" - Historical Context
Before troponin, clinicians used a combination of enzymes timed sequentially to establish MI:
| Enzyme | Rise | Peak | Normalize | Specificity |
|---|---|---|---|---|
| Myoglobin | 1-3 h | 6-9 h | 24 h | Very low |
| CK-MB | 2-4 h | 24-48 h | 72 h | Moderate |
| AST/SGOT | 6-8 h | 24-48 h | 3-4 days | Very low |
| LDH (LDH-1) | 24 h | 3-6 days | 14 days | Low |
AST was the "middle" marker in this ladder. When all three (CK, AST, LDH) followed a consistent temporal rise-and-fall pattern together, clinicians were more confident.
Current Status: Completely Obsolete for MI Diagnosis
AST/SGOT is no longer recommended and not used in the diagnosis of MI. It was abandoned when cardiac-specific troponins became available in the 1990s, and its use has been explicitly dropped from all current guidelines (ACC/AHA, ESC).
Today, AST elevation in the context of MI is interpreted differently:
- In MI, a high AST usually reflects congestive hepatopathy (liver congestion from low cardiac output/right heart failure) rather than myocardial damage itself
- An elevated AST with an elevated ALT ratio (AST:ALT >2) in an MI patient suggests hepatic ischemia or "shock liver"
What AST Is Used For Today
AST remains important - just not for the heart. It is used to:
- Diagnose and monitor liver disease (hepatitis, cirrhosis, NAFLD)
- Detect drug-induced hepatotoxicity (statins, which MI patients take)
- Monitor skeletal muscle disease
- As part of the AST:ALT ratio (DeRitis ratio) in distinguishing alcoholic from non-alcoholic liver disease
Bottom Line
AST/SGOT was historically significant as the first biochemical marker of MI (1954), but its lack of cardiac tissue specificity made it unreliable. It is now completely obsolete for MI diagnosis and has been fully replaced by cardiac troponins (cTnI/cTnT). In modern practice, an elevated AST in an MI patient is most likely reflecting secondary liver injury from poor cardiac output, not myocardial necrosis.
- Tietz Textbook of Laboratory Medicine, 7th ed. (Cardiac Function chapter)
- Robbins & Kumar Basic Pathology (Clinical Features of MI)
GCTs in seminoma means??
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is the complete answer:
GCTs in the Context of Seminoma
GCT = Germ Cell Tumor
Seminoma is a specific type of GCT - it sits within the broader GCT category of testicular tumors. Understanding GCTs as a whole is necessary to understand where seminoma fits.
What Are GCTs?
Germ cell tumors are neoplasms derived from primordial germ cells (the cells that normally give rise to sperm). They account for ~95% of all testicular tumors and are the most common malignancy in males aged 15-45 years.

WHO 2022 Classification of Testicular GCTs (Table 21.6)
GCTs are divided into two major groups based on whether they arise from a precursor lesion called germ cell neoplasia in situ (GCNIS):
Group 1: GCTs Derived from GCNIS (the main group)
Pure (single histologic type):
- Seminoma ← the most common single-type GCT
Nonseminomatous GCTs (NSGCTs):
- Embryonal carcinoma
- Yolk sac tumor (postpubertal type)
- Choriocarcinoma
- Teratoma (postpubertal type)
- Teratoma with somatic-type malignancy
- Mixed GCT (more than one histologic type combined)
Group 2: GCTs NOT Related to GCNIS
- Spermatocytic tumor
- Teratoma (prepubertal type)
- Yolk sac tumor (prepubertal type)
(Robbins, Cotran & Kumar - Pathologic Basis of Disease, 2022 WHO Classification, Table 21.6)
The Key Division: Seminoma vs. Nonseminomatous GCT
This is the most clinically important distinction because it directly guides treatment:
| Feature | Seminoma | Nonseminomatous GCT (NSGCT) |
|---|---|---|
| Radiosensitivity | Highly radiosensitive | Radioresistant |
| Chemosensitivity | Cisplatin-based (very responsive) | Cisplatin-based |
| Serum markers | AFP normal; may have mild hCG rise | AFP and/or hCG often elevated |
| Prognosis | Generally better | More aggressive |
| Age | Slightly older (30s) | Slightly younger (20s) |
Seminoma Specifically - Morphology
Gross: Lobulated, homogeneous, cream-colored tumor without hemorrhage or necrosis (unlike NSGCTs which are heterogeneous).
Microscopic (classic features):
- Large cells with clear cytoplasm (due to glycogen content), well-defined cell borders, and centrally placed nuclei with prominent nucleoli - resembling primordial germ cells
- Cells arranged in lobules separated by fibrous septa
- Lymphocytic infiltrate in the stroma (characteristic)
- Granulomatous reaction (syncytiotrophoblastic giant cells may be present in ~15% - these produce hCG and account for the mild hCG elevation sometimes seen)
- Isochromosome 12p is invariably present
Pathogenesis of GCTs (Shared by Seminoma and NSGCTs)
The common pathway:
- Environmental triggers (cryptorchidism, pesticides, estrogen exposure in utero) act on a primordial germ cell
- Acquired genetic/epigenetic modifications cause arrested differentiation
- KIT receptor mutations promote growth → germ cell neoplasia in situ (GCNIS) develops
- At puberty, hormonal stimulation + isochromosome 12p acquisition drives progression to invasive GCT
- GCNIS can differentiate toward seminoma (retaining germ cell features) or toward pluripotent cells → NSGCTs
Key genetic facts:
- Isochromosome 12p - found in virtually ALL invasive GCTs regardless of type (diagnostic marker)
- KIT mutations - particularly important in seminomas
- Transcription factors OCT3/4 and NANOG are expressed in GCNIS and seminoma (markers of undifferentiated/pluripotent state)
Risk Factors for GCTs
- Cryptorchidism - most important (~10% of GCTs associated; risk is 10x normal)
- Family history (risk 4x in fathers/sons, 8-10x in brothers)
- Klinefelter syndrome - strongly associated with mediastinal GCTs
- European descent (highest rates in Northern Europe and New Zealand)
- Testicular dysgenesis syndrome (cryptorchidism + hypospadias + poor sperm quality)
Tumor Markers Used in GCT Diagnosis
| Marker | Seminoma | NSGCT |
|---|---|---|
| AFP (alpha-fetoprotein) | Never elevated (if AFP is raised, it's not pure seminoma) | Elevated in yolk sac tumor, embryonal carcinoma |
| hCG | Mildly elevated in ~15% (from syncytiotrophoblastic cells) | Elevated in choriocarcinoma, mixed GCTs |
| LDH | Elevated (correlates with tumor bulk) | Elevated |
| PLAP (placental alkaline phosphatase) | Positive | Variable |
Important exam point: If a patient has a testicular tumor histologically diagnosed as "seminoma" but AFP is elevated, it must be reclassified as a mixed GCT (with a NSGCT component), because pure seminoma never produces AFP.
Summary
GCT = Germ Cell Tumor - the overarching category of which seminoma is the most common pure type. The GCT classification is not just academic; it determines:
- Whether the tumor will respond to radiotherapy (only seminomas do)
- Which tumor markers to follow
- Staging and chemotherapy protocols
- Prognosis (good/intermediate/poor risk by IGCCCG classification)
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease, 10th ed. (Chapter 21, pp. 896-903)
This is a shared conversation. Sign in to Orris to start your own chat.