Rxplian atrial fibrillation
Reading File
Finding Sources
Searching the Web
atrial fibrillation pathophysiology classification management 2024
Searching PubMed
"atrial fibrillation"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have enough comprehensive information to write a thorough answer on atrial fibrillation.
Atrial Fibrillation (AF)
Atrial fibrillation is the most common sustained cardiac arrhythmia. It is characterized by chaotic, uncoordinated electrical activity in the atria, resulting in loss of effective atrial contraction and an irregularly irregular ventricular response.
Epidemiology
- Affects approximately 1% of the population over 60 years and 5% of those 69 years and older
- Prevalence rises sharply with age - about 12% at age ≥75 and 18% at age ≥85
- One-third of all AF patients are ≥80 years old
- Strong associations with hypertension, heart failure, ischemic heart disease, obesity, obstructive sleep apnea, and valvular disease
(Braunwald's Heart Disease, p. 1265; Rosen's Emergency Medicine, p. 1340)
Pathophysiology
AF arises from two interacting mechanisms:
1. Focal triggers - Most commonly, rapid firing ectopic foci located in the sleeves of the pulmonary veins discharge at high rates (300-600 impulses/min) and initiate the arrhythmia. Atrial premature complexes from pulmonary vein sleeves are the dominant trigger.
2. Sustaining substrate - Multiple re-entry circuits ("multiple wavelets") perpetuate the arrhythmia. The substrate is created by atrial fibrosis, structural remodeling, inflammation, and electrical heterogeneity.
Key contributors to the substrate:
- Age-related atrial fibrosis - progressive scarring creates conduction inhomogeneity
- Hypertension with LV hypertrophy - elevated LA pressure causes LA dilation and fibrosis
- Obesity and epicardial fat - adipocyte infiltration, profibrotic and proinflammatory effects
- Obstructive sleep apnea - hypoxia, autonomic surges, and hypertension all contribute
- AF begets AF - electrical and structural remodeling from ongoing AF perpetuates itself (tachycardia-induced remodeling)
Hemodynamic consequences:
- Loss of atrial "kick" reduces cardiac output (particularly in HFpEF patients who depend on late diastolic filling)
- Rapid ventricular rate reduces diastolic filling time and stroke volume
- Stasis in the left atrial appendage promotes thrombus formation
(Braunwald's Heart Disease, p. 1266-1268)
Classification
| Type | Definition |
|---|---|
| Paroxysmal | Terminates spontaneously within 7 days |
| Persistent | Lasts more than 7 days; requires cardioversion to terminate |
| Long-standing persistent | Continuous AF lasting more than 12 months |
| Permanent | Persistent AF where no further attempts to restore sinus rhythm are planned |
A 2024 ESC staging system also classifies patients by disease progression:
- Stage 1 - at risk (risk factors present, no AF yet)
- Stage 2 - pre-AF (subclinical AF or atrial changes detected)
- Stage 3 - clinical AF (symptomatic or diagnosed)
- Stage 4 - permanent AF
(Braunwald's Heart Disease, p. 1270; Miller's Anesthesia, p. 384)
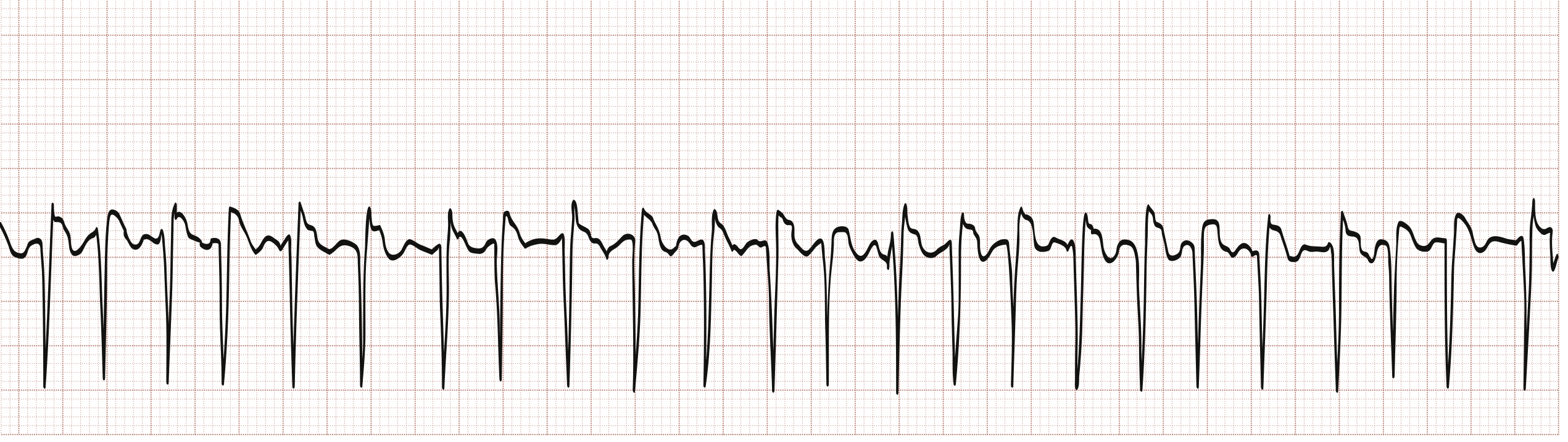
ECG Features
The hallmark ECG findings are:
- Absent P waves - replaced by irregular fibrillatory (f) waves at 300-600/min, variable in amplitude, shape, and timing
- Irregularly irregular RR intervals - the defining feature (no two R-R intervals are equal)
- Ventricular rate - typically 100-160 bpm when untreated; can appear "regular" at very rapid rates (>170 bpm)
- f waves are best seen in lead V1 and inferior leads; they can be coarse or very fine (occasionally imperceptible)
Warning sign: A ventricular rate exceeding 200 bpm in AF strongly suggests an accessory pathway (Wolff-Parkinson-White syndrome) and changes management significantly.
(Braunwald's Heart Disease, p. 1265-1266)
Causes and Precipitants
Cardiac:
- Hypertension (most common overall cause)
- Ischemic heart disease / ACS
- Mitral valve disease (especially mitral stenosis)
- Heart failure (HFrEF, HFpEF, HFmrEF)
- Hypertrophic cardiomyopathy
- Dilated cardiomyopathy
- Constrictive pericarditis, amyloidosis
- Pulmonary hypertension
Non-cardiac:
- Hyperthyroidism
- Obesity and obstructive sleep apnea
- Alcohol ("holiday heart")
- Post-cardiac/thoracic surgery
- Sepsis or critical illness
- WPW syndrome (tachycardia-induced AF)
Clinical Features
Symptoms range from none (25% are asymptomatic - often elderly patients) to severely disabling:
- Palpitations - most common complaint in younger patients; less prominent in elderly
- Fatigue and effort intolerance - often incorrectly attributed to aging
- Dyspnea - worsened by loss of atrial contribution + rapid rate
- Lightheadedness, chest discomfort
- Polyuria - from release of atrial natriuretic peptide
- Syncope - from long sinus pause at AF termination (sick sinus syndrome) or severe hemodynamic compromise
- Acute pulmonary edema - particularly in HFpEF patients with stiff LV
- Stroke - may be the first presentation; AF causes a 5-fold increase in stroke risk
(Braunwald's Heart Disease, p. 1269-1270)
Stroke Risk Stratification - CHA₂DS₂-VASc Score
Used to determine who needs anticoagulation:
| Risk Factor | Points |
|---|---|
| Congestive heart failure | 1 |
| Hypertension | 1 |
| Age 75+ | 2 |
| Diabetes mellitus | 1 |
| Stroke/TIA/thromboembolism (prior) | 2 |
| Vascular disease (prior MI, PAD, aortic plaque) | 1 |
| Age 65-74 | 1 |
| Sex category (female) | 1 |
- Score ≥2 (men) or ≥3 (women): anticoagulation recommended
- All patients ≥75 years have a score of ≥2 by age alone and are candidates for anticoagulation
- Note: The 2024 ESC guidelines removed the sex-based point (now called CHA₂DS₂-VA score)
Management
1. Rate Control
Goals: 60-80 bpm at rest; 90-115 bpm during moderate exercise.
First-line agents:
- Beta-blockers (metoprolol, atenolol, carvedilol) - preferred in heart failure and post-MI
- Non-dihydropyridine calcium channel blockers (diltiazem, verapamil) - avoid in HFrEF
- Digoxin - less effective during exercise; useful in heart failure or sedentary patients; often combined with a beta-blocker or CCB
2. Rhythm Control
Restoring and maintaining sinus rhythm - considered especially when:
- Symptoms persist despite adequate rate control
- First presentation in younger patients
- HF with AF as a likely contributor
- Patient preference
Pharmacologic cardioversion:
- Flecainide, propafenone (class IC) - safe in structurally normal hearts
- Amiodarone - most effective but significant long-term toxicity
- Ibutilide (IV) - for acute cardioversion
Electrical cardioversion (DC cardioversion):
- Synchronized DC shock for acute hemodynamic instability or elective rhythm restoration
- If AF >48 hours duration: anticoagulate for ≥3 weeks before cardioversion OR perform TEE to exclude LA thrombus
Catheter ablation (pulmonary vein isolation - PVI):
- Targets and electrically isolates pulmonary vein triggers
- Now a first-line option for paroxysmal AF per 2024 ESC guidelines
- Superior to antiarrhythmic drugs for maintaining sinus rhythm
- Especially beneficial in HFrEF - randomized trials show reduced mortality and hospitalization
3. Anticoagulation (Stroke Prevention)
DOACs (preferred over warfarin in non-valvular AF):
- Dabigatran (direct thrombin inhibitor)
- Rivaroxaban, Apixaban, Edoxaban (factor Xa inhibitors)
- No dietary restrictions, no INR monitoring required
- Similar or better stroke prevention with similar or less bleeding vs. warfarin
Warfarin: Target INR 2.0-3.0 (2.0-2.5 in elderly); still preferred in valvular AF (rheumatic mitral stenosis) where DOACs are contraindicated
SGLT2 inhibitors (2024 ESC update): Recommended in AF + heart failure regardless of ejection fraction to reduce HF hospitalization and cardiovascular death
4. Bleeding Risk - HAS-BLED Score
Factors include hypertension, renal/liver dysfunction, prior stroke, prior bleeding, labile INR, elderly age (>65), and drugs/alcohol. Bleeding risk should be weighed against stroke risk - a high HAS-BLED score should prompt correction of modifiable bleeding risks, not automatic withholding of anticoagulation.
5. Non-Pharmacologic Approaches
- AV node ablation + pacemaker - for rate control when drugs fail
- Surgical MAZE procedure - creates lines of block in the atria; often performed concomitantly with valve surgery; highly effective for maintaining sinus rhythm
- Left atrial appendage closure/ligation (e.g., WATCHMAN device) - for patients with high stroke risk who cannot tolerate anticoagulation; 2024 ESC recommends surgical LAA closure as an adjunct to anticoagulation during AF ablation surgery
6. Risk Factor Modification (2024 ESC AF-CARE Framework)
The 2024 ESC guidelines updated the management pathway to AF-CARE:
- C - Comorbidities and cardiovascular risk factor management (weight loss, BP control, sleep apnea treatment, exercise)
- A - Avoid stroke (anticoagulation)
- R - Rate and rhythm control
- E - Evaluation (dynamic, ongoing reassessment)
(Braunwald's Heart Disease, p. 1275-1283; 2024 ESC AF Guidelines)
Special Situations
AF + WPW Syndrome
- Do NOT use AV nodal blockers (digoxin, verapamil, diltiazem, adenosine) - they can accelerate conduction over the accessory pathway causing VF
- Treat with procainamide or DC cardioversion
AF + Mitral Stenosis
- Very high embolic risk - combination of MS + AF carries risk similar to prosthetic valves
- Use warfarin (NOT DOACs) regardless of CHA₂DS₂-VASc score
- Even transient AF (<30 seconds) significantly increases thromboembolic risk
Postoperative AF
- Common after cardiac and thoracic surgery; often self-limiting
- Rate control and anticoagulation per standard guidelines
Pregnancy
- AF is rare but serious; treatment options are limited
- Beta-blockers and digoxin are preferred for rate control
- Heparin (not warfarin) for anticoagulation in the first trimester and near delivery
Recent Evidence
A 2025 meta-analysis (PMID: 39918465) in JACC found that in AF patients with stable coronary disease, anticoagulation alone (without antiplatelet therapy) is safer and sufficient for most patients, supporting the move away from combination antithrombotic therapy.
A 2026 network meta-analysis (PMID: 42135825) confirmed a dose-dependent relationship between alcohol consumption and AF risk, reinforcing alcohol reduction as a key modifiable risk factor.
Summary Table
| Aspect | Key Points |
|---|---|
| Mechanism | Focal triggers (PV ectopy) + re-entry substrate (atrial fibrosis) |
| ECG | Absent P waves, fibrillatory baseline, irregularly irregular RR |
| Classification | Paroxysmal → Persistent → Long-standing persistent → Permanent |
| Stroke risk | CHA₂DS₂-VASc score; 5x increased risk |
| Rate control | Beta-blockers, CCBs, digoxin |
| Rhythm control | DC cardioversion, antiarrhythmics, catheter ablation (PVI) |
| Anticoagulation | DOACs preferred; warfarin for valvular AF |
| 2024 Updates | CHA₂DS₂-VA (sex removed), AF-CARE framework, ablation as first-line for paroxysmal AF, SGLT2i in AF+HF |
This is a shared conversation. Sign in to Orris to start your own chat.