Pancreatic pseudocode information. For n MBBB S student . Final year level knowledge both practical and theory
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pancreatic pseudocyst" management
Pancreatic pseudocyst information. For n MBBS student . Final year level knowledge both practical and theory
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pancreatic pseudocyst" management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from multiple major surgical and gastroenterology textbooks. Let me compile the complete final-year MBBS-level answer.
Pancreatic Pseudocyst - Final Year MBBS Complete Guide
1. DEFINITION
A pancreatic pseudocyst is a localized collection of pancreatic fluid enclosed by a wall of fibrous or granulation tissue, which:
- Lacks an epithelial lining (hence "pseudo" - distinguishing it from a true cyst)
- Contains amylase-rich fluid with pancreatic enzymes
- Has no solid/necrotic debris (if debris is present, it is called Walled-Off Necrosis, WON - not a pseudocyst)
- Takes at least 4 weeks to mature and develop a proper capsule
Key exam point: A pseudocyst develops ONLY after interstitial edematous pancreatitis (not necrotizing). If it follows necrosis and persists >4 weeks, it is WON.
(Current Surgical Therapy 14e; Sleisenger & Fordtran's GI & Liver Disease)
2. REVISED ATLANTA CLASSIFICATION (2012) - MUST KNOW
| Pancreatitis Type | <4 weeks | >4 weeks |
|---|---|---|
| Interstitial Edematous | Acute Pancreatic Fluid Collection (APFC) | Pancreatic Pseudocyst |
| Necrotizing | Acute Necrotic Collection (ANC) | Walled-Off Necrosis (WON) |
- The term "pancreatic abscess" is now obsolete (dropped from Atlanta 2012)
- The term "infected pseudocyst" is also discouraged
3. EPIDEMIOLOGY
- Occurs in 5-15% of patients after acute pancreatitis
- More common after chronic pancreatitis (20-40% of cases)
- Most common pancreatic cystic lesion overall
- Located most often in the lesser sac, around the body/tail of pancreas
- Can also be found in: pelvis, scrotum, mediastinum, thorax (rare)
(Current Surgical Therapy 14e)
4. ETIOLOGY / CAUSES
| Cause | Notes |
|---|---|
| Acute pancreatitis | Most common; 10-15% develop pseudocyst |
| Chronic pancreatitis | 20-40%; due to duct calcification/obstruction |
| Blunt abdominal trauma | Duct injury over vertebral column - pseudocyst forms at neck/body |
| Iatrogenic | Post-ERCP, post-surgery |
5. PATHOGENESIS
- Injury/inflammation → disruption of main pancreatic duct or its branches
- Extravasation of enzyme-rich pancreatic juice into peripancreatic tissue
- Intense inflammatory reaction in peritoneum, retroperitoneum, and serosa of adjacent organs
- Granulation tissue and fibrosis form around the collection → capsule matures over 4-6 weeks
- If duct-pseudocyst communication persists → cyst enlarges (can reach 20-30 cm)
Contents: Watery, clear fluid rich in amylase and pancreatic enzymes. May become:
- Xanthochromic (with hemorrhage)
- Purulent (with infection)
(Maingot's Abdominal Operations)
6. D'EGIDIO CLASSIFICATION (Key for Exam + Management)
| Type | Setting | Pancreatic Duct | Duct Communication | Preferred Treatment |
|---|---|---|---|---|
| Type I | Acute pancreatitis | Normal | No | Percutaneous drainage |
| Type II | Acute or chronic pancreatitis | Abnormal (no stricture) | 50% | Internal drainage or resection |
| Type III | Chronic pancreatitis | Abnormal (stricture present) | Yes | Internal drainage + duct decompression |
(Maingot's Abdominal Operations)
7. CLINICAL FEATURES
Suspect pseudocyst when:
- Patient with acute pancreatitis fails to recover after 1 week, OR
- Initial improvement followed by clinical deterioration
Symptoms:
- Epigastric pain/discomfort (most common)
- Anorexia, nausea, vomiting
- Early satiety
- Low-grade fever
- Back pain
- Palpable epigastric mass (in large pseudocysts)
Signs:
- Epigastric mass - smooth, rounded, non-tender (usually)
- Mild jaundice (if bile duct compressed)
- Serum amylase: fails to normalize or shows a secondary rise (2-4x normal) in ~50% of patients
8. INVESTIGATIONS
CT Scan (Investigation of Choice)
- Contrast-Enhanced CT (CECT): accuracy approaching 100%
- Appears as: rounded, well-defined, low-attenuation, fluid-filled structure within or adjacent to the pancreas
- Non-operator dependent; useful for planning therapy
- Shows size, location, relation to adjacent structures
CT scan of pancreatic pseudocyst (P) in the lesser sac; S = stomach:
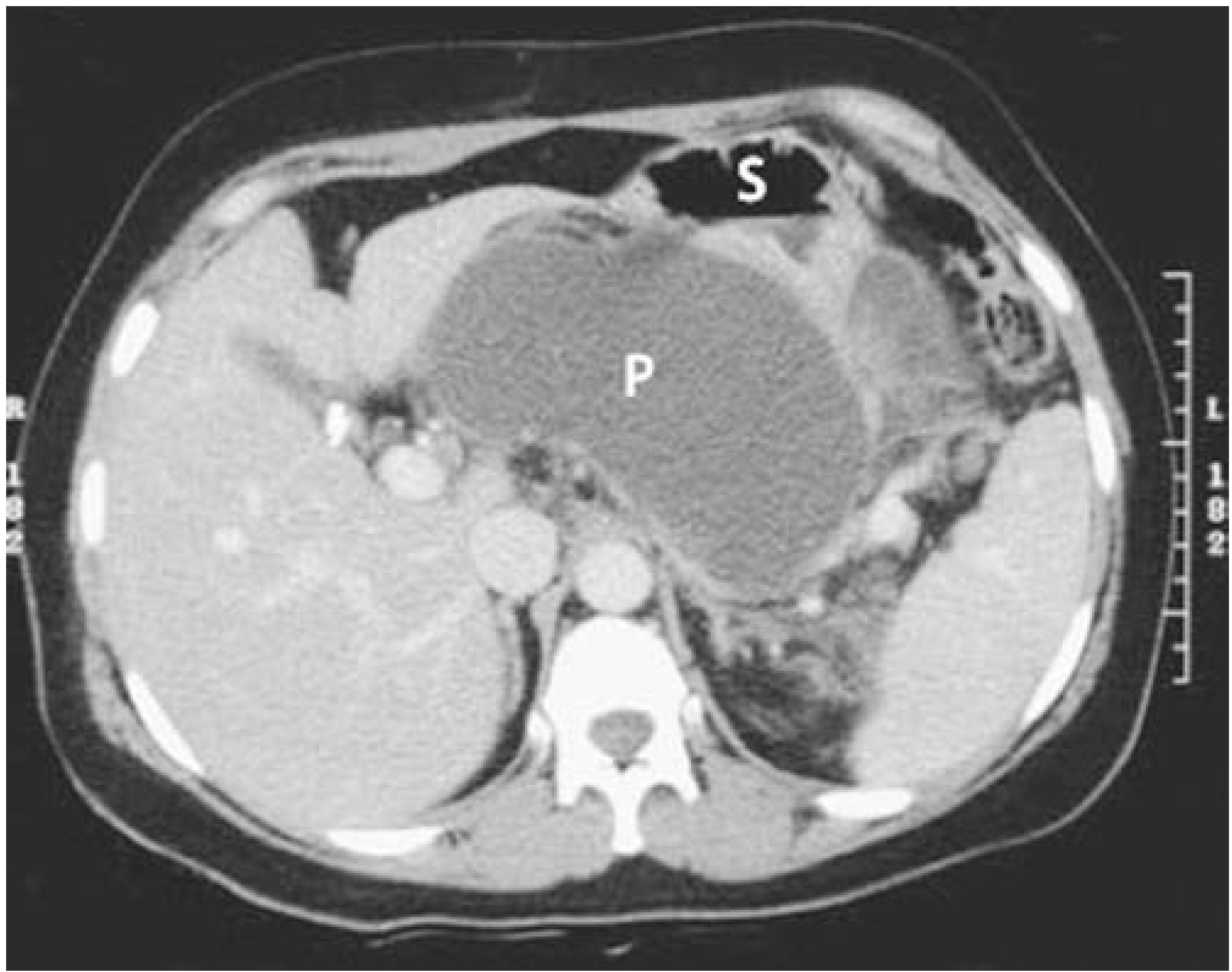
(Maingot's Abdominal Operations)
Ultrasound (USG)
- Good for detection; can show extent of fluid
- Limited by: bowel gas, patient habitus, operator skill
- Better than CT for solid tissue content within collection
- Used to guide FNA
Endoscopic Ultrasound (EUS)
- Better delineates internal septation than CT
- Useful to distinguish pseudocyst from cystic neoplasm
- Used for drainage guidance
MRCP/MRI
- Now preferred over ERCP for ductal anatomy
- Shows communication between pseudocyst and pancreatic duct
ERCP
- Historically used; now reserved for therapy (transpapillary drainage)
- Risk of introducing infection
Cyst Fluid Analysis (FNA via EUS)
- High amylase → pseudocyst (vs. cystic neoplasm)
- Low CEA, CA19-9 → favors pseudocyst
- Low or absent mucin → rules out mucinous neoplasms (IPMN, MCN)
9. COMPLICATIONS (RRHM - Remember: Rupture, Rupture into GI, Hemorrhage, Mass effect)
Complications occur in approximately 10% of cases.
| Complication | Details |
|---|---|
| Infection | Up to 25% of cases; presents with sepsis; requires drainage |
| Hemorrhage | Most dangerous (~20% mortality); erosion of splenic, gastroduodenal, or middle colic vessels; pseudoaneurysm formation due to elastase action on vessel wall; treat with angioembolization first, then surgery |
| Rupture | Into GI tract (→ cystoenteric fistula or self-resolution); into peritoneum (→ pancreatic ascites, chemical peritonitis); into pleural cavity (→ pancreatic pleural effusion / pancreaticopleural fistula) |
| Mass effect | If >6 cm: gastric outlet obstruction, duodenal obstruction, biliary obstruction, venous thrombosis (portal/splenic/SMV) → portal hypertension/varices |
10. MANAGEMENT
Step 1: Watchful Waiting (Conservative)
- Up to 90% of acute peripancreatic fluid collections resolve spontaneously
- Asymptomatic pseudocysts: observe for at least 6 weeks
- Indications for intervention: symptomatic, enlarging, infected, or complicated pseudocyst
Step 2: Drainage (Three Routes)
A. Endoscopic Drainage (Now First-Line)
-
Endoscopic Transmural Drainage (cystogastrostomy/cystoduodenostomy)
- EUS-guided placement of stents through stomach or duodenum wall into the pseudocyst
- Requires pseudocyst to be within 1 cm of the gastric/duodenal wall
- Lumen-apposing metal stents (LAMS) now used - superior to plastic stents (2026 meta-analysis [PMID: 41276442])
- Preferred approach for most pseudocysts today
-
Transpapillary Drainage (via ERCP)
- Wire passed through papilla, through pancreatic duct, into communicating pseudocyst
- Best for pseudocysts that communicate with the main duct
- Cannot be done if downstream ductal obstruction is present
B. Percutaneous Drainage
- CT or ultrasound-guided catheter drainage
- Risk: external pancreatic fistula (especially if ductal communication exists)
- Preferred for: infected pseudocysts, Type I (no ductal communication), critically ill patients
- Contraindication: do NOT drain externally if downstream ductal obstruction unrelieved - high fistula risk
C. Surgical Drainage (Internal)
Indications: failed endoscopic/percutaneous drainage, concurrent surgical pathology, inability to safely access endoscopically.
Three surgical options:
- Cystogastrostomy - posterior cystogastrostomy; pseudocyst drained into posterior wall of stomach (most common for pseudocysts in lesser sac/posterior to stomach)
- Cystojejunostomy (Roux-en-Y) - best for: large pseudocysts, multiple pseudocysts, pseudocysts near duodenum
- Cystoduodenostomy - for pseudocysts in head region closely adherent to duodenum
Resection (distal pancreatectomy) - for pseudocysts in the pancreatic tail or with mid-pancreatic duct disruption.
Critical rule from Maingot's: Never drain a pseudocyst externally if there is unrelieved downstream ductal obstruction - high risk of persistent external fistula.
11. PSEUDOCYST vs. OTHER PANCREATIC CYSTS (Exam Favourite)
| Feature | Pseudocyst | Serous Cystadenoma | Mucinous Cystic Neoplasm (MCN) | IPMN |
|---|---|---|---|---|
| Epithelial lining | None | Yes | Yes | Yes |
| Fluid amylase | High | Low | Low | May be high |
| CEA in fluid | Low | Low | High | Variable |
| Malignant potential | None | Very low | Yes | Yes |
| History of pancreatitis | Usually yes | No | No | No |
| Communication with duct | Sometimes | No | No | Yes (by definition) |
12. SURGERY-SPECIFIC: KEY PRACTICAL POINTS
- Minimum maturity before surgery: 6 weeks (for a defined, thick wall suitable for anastomosis)
- EUS-guided drainage is the dominant approach today; metallic stents outperform plastic stents (2026 meta-analysis, [PMID: 41276442])
- For hemorrhage complication: angioembolization first, then surgery if embolization fails
- Infected pseudocyst: drain first (percutaneous/endoscopic), treat infection, then address duct anatomy
- Pancreatic ascites: diagnosed by very high ascitic fluid amylase; treat with octreotide ± ERCP/stenting ± surgery
13. HIGH-YIELD EXAM SUMMARY
| Point | Fact |
|---|---|
| Pseudocyst = | Fluid collection without epithelial lining, forms after 4 weeks |
| Most common cause | Acute pancreatitis (alcohol, gallstones) |
| Investigation of choice | CECT abdomen |
| Spontaneous resolution | Up to 90% of APFCs resolve; most asymptomatic pseudocysts resolve |
| Size for intervention | Symptomatic, enlarging, or complicated - NOT size alone |
| Internal drainage preferred over external | Avoids fistula |
| No. 1 current drainage method | EUS-guided endoscopic transmural drainage |
| Hemorrhage complication | Pseudoaneurysm → angioembolization first |
| Rupture into peritoneum | Pancreatic ascites + chemical peritonitis |
| Rupture into chest | Pancreaticopleural fistula → massive pleural effusion |
| Minimum time to operate | 6 weeks (for wall maturity) |
| WON vs Pseudocyst | WON has debris/necrosis; pseudocyst is pure fluid |
Sources:
- Maingot's Abdominal Operations (Pancreatic Pseudocyst chapter)
- Current Surgical Therapy 14e (Management of Pancreatic Pseudocyst)
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease
- Schwartz's Principles of Surgery 11e
- Mulholland & Greenfield's Surgery 7e
- Recent 2026 meta-analysis on metallic vs plastic stents: [Chen H et al., HPB 2026, PMID: 41276442]
Also as a medical student what history taking and general and systemic examination should we do
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is the complete, structured clinical approach guide for a final year MBBS student:
Pancreatic Pseudocyst - History Taking & Clinical Examination
HOW TO APPROACH THIS CASE AS AN MBBS STUDENT
When you see a patient suspected of having a pancreatic pseudocyst, think of it as a two-part story: the underlying pancreatic disease (usually pancreatitis) and the pseudocyst itself as a complication. Your history and examination must address both.
PART 1: HISTORY TAKING
A. Chief Complaint
The patient typically presents with one or more of:
- Epigastric pain / upper abdominal pain
- Abdominal lump / swelling
- Nausea and vomiting
- Failure to recover after an episode of acute pancreatitis
B. History of Present Illness (HPI)
1. Pain - SOCRATES
| Feature | What to Ask | What to Expect |
|---|---|---|
| Site | "Where exactly is the pain?" | Epigastric (central upper abdomen) |
| Onset | "When did it start? Sudden or gradual?" | Gradual, developing days-weeks after pancreatitis |
| Character | "Is it dull, burning, or sharp?" | Dull, aching, constant |
| Radiation | "Does it go anywhere?" | May radiate to the back (band-like) |
| Associated symptoms | See below | Nausea, vomiting, fever |
| Timing | "Is it there all the time or does it come and go?" | Usually persistent |
| Exacerbating/Relieving factors | "Does eating make it worse?" | Worse with food; leaning forward may relieve |
| Severity | "Rate 1-10" | Moderate; less severe than acute pancreatitis |
2. Associated Symptoms - Ask Specifically About:
GI symptoms:
- Nausea and vomiting
- Anorexia (loss of appetite)
- Early satiety ("Do you feel full after eating only a little?") - suggests gastric compression
- Vomiting of blood (hematemesis) or black/tarry stools (melena) - suggests hemorrhagic complication
- Change in bowel habits, pale/greasy stools (steatorrhea) - suggests exocrine insufficiency
Constitutional:
- Fever - suggests infection of the pseudocyst
- Weight loss - important; also raises suspicion for malignancy
Obstructive symptoms:
- Jaundice, dark urine, pale stools - suggests bile duct compression by the pseudocyst
- Pruritus (itching)
Respiratory:
- Breathlessness, pleuritic chest pain - suggests pancreaticopleural fistula or pleural effusion (rare but important)
C. Past Medical History
Ask specifically about:
- Previous episodes of pancreatitis - "Have you ever been told you had pancreatitis before?"
- If yes: How many times? Were you hospitalized? Was it treated?
- Gallstones - "Have you ever been told you have stones in your gallbladder?"
- Biliary pancreatitis is a leading cause
- Chronic pancreatitis - "Do you have a long-standing problem with your pancreas?"
- Abdominal trauma - "Have you had any injury to your abdomen - road accident, sports, fall?" (trauma is a classic cause, especially in young patients)
- Diabetes mellitus - new-onset diabetes may suggest pancreatic endocrine insufficiency
- Hyperlipidaemia (raised triglycerides) - a recognized cause of pancreatitis
- Peptic ulcer disease / GERD - for differential diagnosis
- Any previous abdominal surgery or ERCP (iatrogenic cause)
- Pancreatic malignancy - previous cancer, weight loss
D. Drug History
Ask about:
- Steroids (prednisolone) - drug-induced pancreatitis
- Azathioprine, 6-mercaptopurine - pancreatitis
- Thiazide diuretics, furosemide - pancreatitis
- Tetracyclines, sulfonamides, valproate - pancreatitis
- NSAIDs - ulcer risk; differential
- Anticoagulants - bleeding risk relevant to hemorrhagic complications
- Any new medications started recently
E. Family History
- Hereditary pancreatitis (autosomal dominant, PRSS1 mutation) - ask if family members have had pancreatitis
- Cystic fibrosis (in young patients) - associated with pancreatic disease
- Pancreatic cancer (for differential)
F. Social History - THE MOST IMPORTANT PART
Alcohol history (always ask carefully and sensitively):
- "Do you drink alcohol?" → "How much per week?" → "For how long?"
- Quantify in units per week (1 unit = 10 mL pure alcohol)
- Chronic heavy alcohol use is the single most common cause of chronic pancreatitis and pseudocysts
- Use CAGE questionnaire if alcoholism suspected:
- Cut down? Annoyed by criticism? Guilty? Eye-opener drink?
Smoking:
- Independent risk factor for chronic pancreatitis
Diet:
- High fat diet → gallstones
Occupation and stress level
Travel history (for infections)
(Rosen's Emergency Medicine; Maingot's Abdominal Operations)
PART 2: GENERAL EXAMINATION
Begin systematically from the end of the bed before touching the patient.
On General Inspection (from the end of the bed):
- Does the patient look well or unwell?
- Body habitus: cachexia/weight loss suggests chronic pancreatitis or malignancy
- Distress: pain, guarding posture (leaning forward - classic pancreatic pain relief posture)
- Jaundice: yellowish discoloration of skin/sclera (bile duct compression)
- Pallor: anemia from chronic disease or hemorrhage
- Signs of chronic liver disease (if alcohol-related): spider naevi, palmar erythema, leukonychia, parotid enlargement, gynecomastia, dupuytren's contracture, loss of body hair
Vital Signs (Always Record):
| Parameter | What it Tells You |
|---|---|
| Temperature | Fever → infected pseudocyst |
| Pulse rate | Tachycardia → sepsis, hemorrhage, pain |
| Blood pressure | Hypotension → hemorrhage, septic shock |
| Respiratory rate | Tachypnoea → pain, pleural effusion, sepsis |
| SpO2 | Low → pleural effusion, ARDS |
| BMI / weight | Malnutrition in chronic disease |
Hands and Upper Limbs:
- Palmar erythema - chronic liver disease (alcohol)
- Leukonychia (white nails) - hypoalbuminemia
- Clubbing - not typical of pancreatitis; if present, consider malignancy/IBD
- Dupuytren's contracture - alcoholism
- Peripheral edema - hypoalbuminemia
- Asterixis (liver flap) - hepatic encephalopathy if liver disease co-exists
- Jaundice in nail beds/palms
Head, Face, and Neck:
- Scleral icterus (jaundice): look at the sclera in good light - earliest sign of jaundice
- Conjunctival pallor: anemia
- Parotid enlargement: alcoholism
- Xanthelasma: hyperlipidemia (a cause of pancreatitis)
- Lymphadenopathy: cervical/supraclavicular (Virchow's node - left supraclavicular - if malignancy)
- JVP: elevated in pericardial effusion (rare pancreatic complication)
Chest:
- Respiratory: dull percussion + reduced breath sounds at left base → left-sided pleural effusion (common in pancreatitis and pancreatic pseudocyst via pancreaticopleural fistula)
- Spider naevi on chest/upper trunk → chronic liver disease
PART 3: ABDOMINAL EXAMINATION
This is the core of your clinical examination for this condition.
1. INSPECTION (Patient lying flat, abdomen exposed from nipples to groin)
Look for:
- Abdominal distension: generalized (ascites from ruptured pseudocyst) or localized (epigastric mass)
- Visible peristalsis: gastric outlet obstruction by large pseudocyst
- Skin changes:
- Grey Turner's sign: bluish-black discoloration of the flanks → retroperitoneal hemorrhage in severe pancreatitis
- Cullen's sign: periumbilical bruising → intraperitoneal hemorrhage
- (Both are rare but examiner favorites - indicate hemorrhagic pancreatitis or ruptured pseudocyst with bleeding)
- Scars: previous surgery (cholecystectomy scar = gallstone history; midline scar = previous pancreatitis surgery)
- Dilated veins: caput medusae → portal hypertension (splenic/portal vein thrombosis complicating pseudocyst)
- Striae: weight gain, Cushing's
- Jaundice of skin
2. PALPATION
Superficial palpation (with warm hands, patient relaxed, knees bent):
- Look at the patient's face for pain
- Note areas of tenderness: epigastric tenderness most common
- Guarding: involuntary muscle contraction over tender area
- Rigidity: board-like abdomen → rupture into peritoneum (peritonitis)
Deep palpation:
- Epigastric mass: the hallmark finding of a large pseudocyst
- Location: epigastric / central upper abdomen
- Character: smooth, rounded, non-tender (if uncomplicated), firm, well-defined
- May be fluctuant (fluid-filled)
- Moves with respiration (superficial masses don't)
- Bowel gas resonant on percussion over it (rare - usually dull)
- Hepatomegaly: alcoholic liver disease or biliary obstruction
- Splenomegaly: splenic vein thrombosis (portal hypertension complicating pseudocyst)
Key examination note:
A large pancreatic pseudocyst in the lesser sac may present as a smooth, rounded, non-pulsatile epigastric mass that is continuous with the stomach anteriorly - you cannot "get above it" easily.
3. PERCUSSION
- Epigastric mass: usually dull to percussion
- Shifting dullness + fluid thrill: look for ascites (pancreatic ascites from ruptured pseudocyst)
- Left lower zone: dullness → left pleural effusion
- Liver dullness: reduced in cirrhosis; increased in hepatomegaly
4. AUSCULTATION
- Bowel sounds: diminished/absent → ileus (severe pancreatitis); high-pitched/tinkling → obstruction
- Bruits: vascular bruits in epigastrium → pseudoaneurysm (rare but important)
5. Special Tests to Mention in Examination
| Test | How | Significance |
|---|---|---|
| Grey Turner's sign | Look at flanks for bruising | Retroperitoneal bleed (hemorrhagic pancreatitis) |
| Cullen's sign | Look at periumbilical area for bruising | Intraperitoneal bleed |
| Fluid thrill | One hand on flank, flick opposite flank, other hand on center | Ascites |
| Shifting dullness | Percuss from center to flanks with patient supine then lateral | Ascites |
6. Complete the Examination
Always mention at the end of your MBBS bedside examination:
- Rectal examination: melaena? (GI bleed from erosion)
- Groin: hernias? lymph nodes?
- Respiratory exam: pleural effusion (left side more common in pancreatitis)
- Nutrition assessment: muscle wasting, BMI
SUMMARY: QUICK CLINICAL PICTURE TO REMEMBER
PATIENT PROFILE:
Middle-aged male (most common)
History of chronic alcohol use OR gallstones
Previous episode(s) of acute pancreatitis
Now presents 4-6 weeks later with:
- Persistent or worsening epigastric pain
- Nausea, anorexia, early satiety
- Low-grade fever
- Failure of serum amylase to normalize
ON EXAMINATION:
- May look cachectic (chronic pancreatitis)
- Scleral icterus (if bile duct compressed)
- Signs of alcoholism (palmar erythema, dupuytren's)
- Epigastric smooth rounded mass (the pseudocyst)
- Left basal dullness (pleural effusion if complicated)
- Rarely: Grey Turner's / Cullen's sign (hemorrhage)
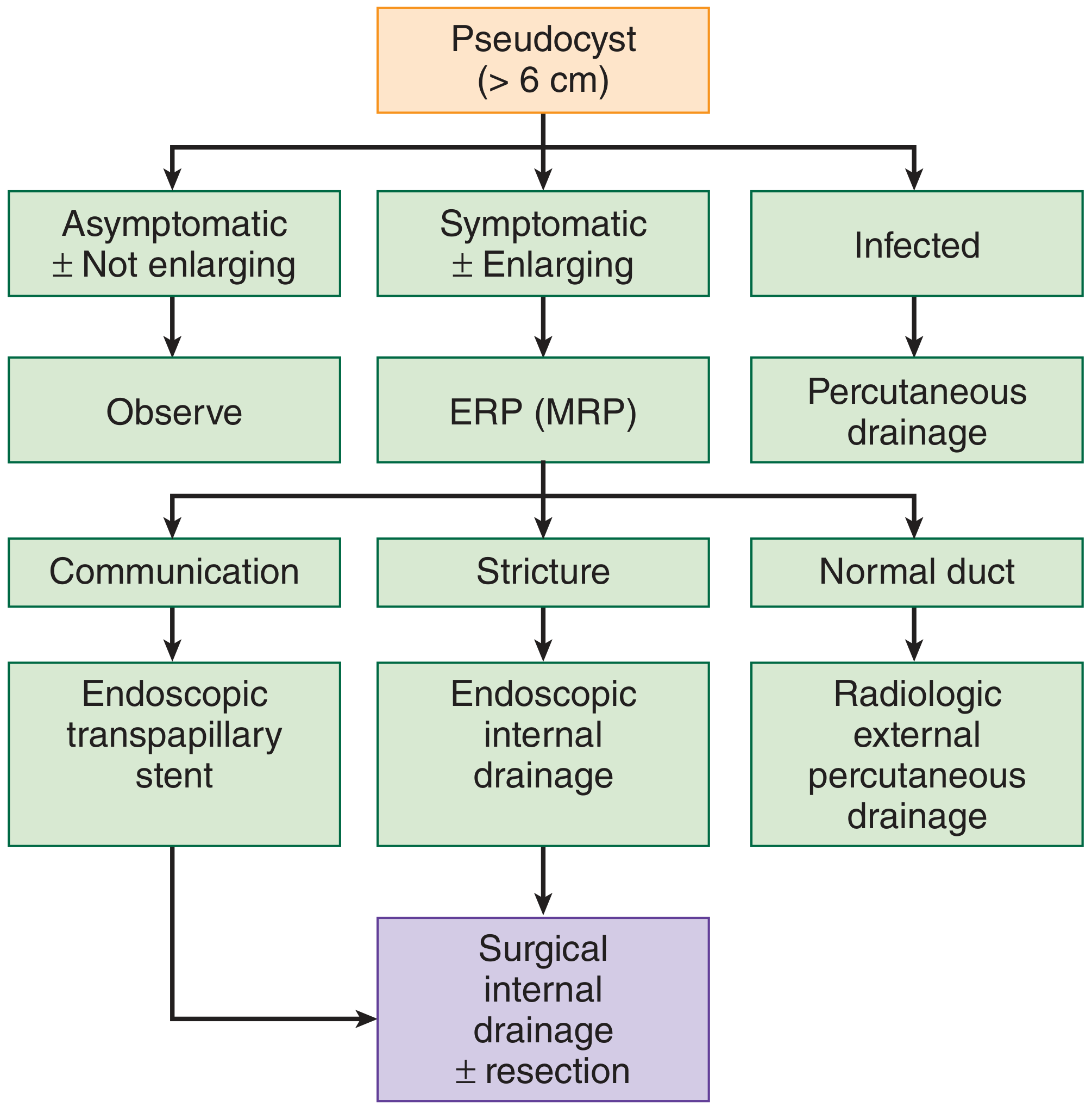
DIAGNOSTIC ALGORITHM (from Maingot's Abdominal Operations)
Sources:
- Maingot's Abdominal Operations (Diagnosis & Management of Pancreatic Pseudocyst)
- Rosen's Emergency Medicine (Chronic Pancreatitis - Clinical Features)
- Current Surgical Therapy 14e (Management of Pancreatic Pseudocyst)
- Sleisenger & Fordtran's GI & Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.