Kluver bucy syndrome
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Kluver-Bucy syndrome"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer.
Klüver-Bucy Syndrome
Historical Background
Klüver-Bucy syndrome was first described in 1939 by Heinrich Klüver and Paul Bucy at the University of Chicago, following their observation that bilateral temporal lobectomy in rhesus monkeys produced a striking cluster of behavioral abnormalities. Their work coincided with Papez's proposal of an emotion circuit in the brain, and together these findings laid the groundwork for understanding the limbic system's role in emotion and behavior.
- Neuroscience: Exploring the Brain, 5th Ed., p. 1672
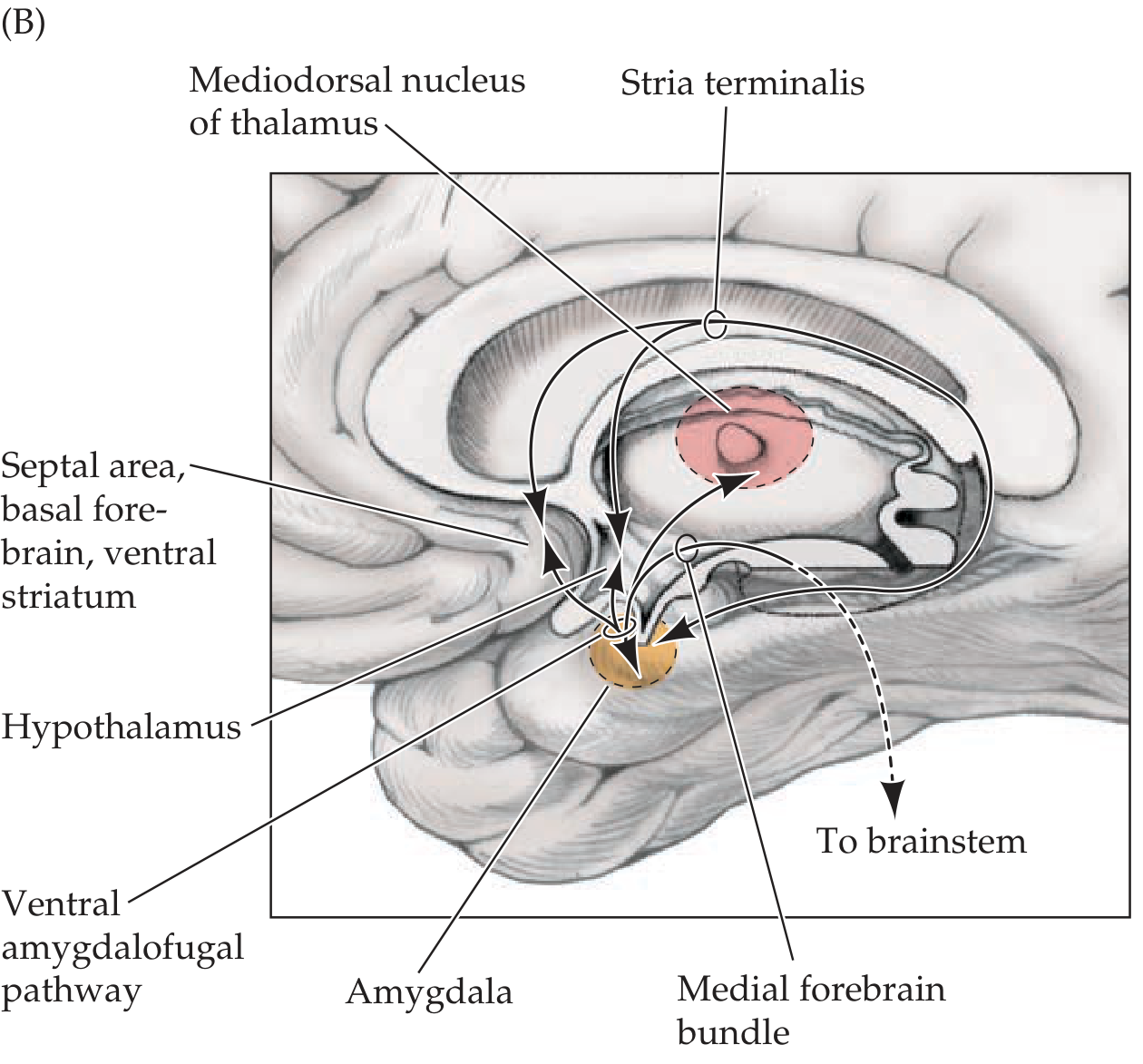
Anatomy
The syndrome arises from bilateral damage to the anterior temporal lobes, particularly the amygdala and adjacent temporal structures. Key anatomical points:
- Bilateral ventral temporal lobe resections (not lateral or unilateral) are required to produce the full syndrome
- Bilateral resection of the lateral amygdala produces both loss of fear and hypersexuality
- The amygdala's role: it normally attaches emotional significance to visual and other sensory percepts via connections with limbic and association cortex
- Disrupted connections run between vision, memory, and limbic structures - so visual percepts lose their ordinary associations and emotional valence
- The uncinate fasciculus and the ventral amygdalofugal pathway are key disrupted tracts
- Neuroanatomy through Clinical Cases, 3rd Ed., p. 876
Clinical Features (the "5 H's + 2" mnemonic)
From Localization in Clinical Neurology, 8e, the features of bilateral anterior temporal tip lesions are:
| Feature | Description |
|---|---|
| Visual agnosia | Objects seen but not recognized; poor visual recognition despite intact visual perception - "psychic blindness" |
| Oral-exploratory behavior | Compulsive licking, biting, placing objects in the mouth to identify them; indiscriminate mouthing of objects |
| Tameness / Placidity | Loss of fear and aggression; the amygdala normally mediates fear responses; animals approach predators without fear |
| Hypersexuality | Markedly increased and often indiscriminate sexual behavior and interest |
| Hyperphagia / Altered dietary habits | Excessive eating, changes in food preferences |
| Hypermetamorphosis | Compulsive urge to attend to and react to every visual stimulus in the environment; inability to ignore any stimulus |
| Hypomotility (in some descriptions) | Decreased spontaneous activity |
Additional features in humans: memory loss, language deficits (aphasia), prosopagnosia, and flattened emotions.
- Bradley and Daroff's Neurology in Clinical Practice, p. 130
- Kaplan & Sadock's Synopsis of Psychiatry, p. 1439
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
Animal vs. Human Presentation
| Animals (monkeys) | Humans | |
|---|---|---|
| Presentation | Complete syndrome after full bilateral temporal lobectomy | Usually partial syndrome only |
| Notable behavior | Even after being attacked by a snake, the monkey returns to examine it | Visual agnosia + memory loss + behavioral changes predominate |
| Fear | Abolished | Reduced but rarely completely absent |
| Additional deficits | - | Aphasia, amnesia more prominent |
Human cases are rare. The syndrome is "observed only rarely in humans" and full expression requires complete bilateral temporal damage.
- Neuroanatomy through Clinical Cases, 3rd Ed.
Causes in Humans
Bilateral temporal damage can result from:
- Herpes simplex encephalitis (classic and most common cause)
- Surgical bilateral temporal lobectomy
- Neurodegenerative diseases - Pick disease (frontotemporal dementia), Alzheimer's disease
- Head trauma with bitemporal injury
- CNS tumors in the temporal region
- Bradley and Daroff's Neurology, p. 130
Differential Diagnosis
Klüver-Bucy syndrome must be distinguished from:
-
Kleine-Levin syndrome (periodic hypersomnia + hyperphagia, adolescent males)
-
Bulimia nervosa (when hyperphagia and altered eating are prominent)
-
CNS tumors and epileptic-equivalent seizures
-
Kaplan & Sadock's Synopsis of Psychiatry, p. 1439
Pathophysiology
The core mechanism is a disconnection between the visual association cortex and the limbic system. Normally, visual percepts are processed by the temporal cortex and "tagged" with emotional and memory significance via the amygdala. When the amygdala and surrounding temporal cortex are bilaterally ablated:
- Visual input arrives but carries no emotional or associative meaning (visual agnosia, psychic blindness)
- Fear conditioning is abolished (tameness)
- Oral exploration substitutes for failed visual identification
- Hypersexuality results from disinhibition of sexual responses (lateral amygdala)
- Hypermetamorphosis reflects loss of filtering of environmental stimuli - described in Kaplan & Sadock's Comprehensive Textbook as "an increased level of attention to individual items in the environment" from bilateral anterior temporal damage
Treatment
Treatment is "difficult and often unsatisfactory" (Lanska, 2018, as cited in Bradley and Daroff's Neurology). Management is focused on:
- Treating the underlying cause (e.g., antiviral therapy for HSV encephalitis)
- Behavioral management for hypersexuality and oral tendencies
- Carbamazepine and other mood-stabilizing agents have been used anecdotally with variable success
Key exam point: Klüver-Bucy syndrome = bilateral anterior temporal lobe lesion + the triad of visual agnosia + oral exploratory behavior + hypersexuality + tameness. The amygdala is the critical structure, especially for the fear and aggression components.
Gerstmann syndrome
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have everything needed for a thorough answer.
Gerstmann Syndrome
Overview
Gerstmann syndrome is a neurological tetrad resulting from a lesion of the dominant (left) inferior parietal lobule, particularly the angular gyrus (Brodmann area 39) or its subjacent white matter. It was described by Josef Gerstmann in the early 20th century.
The Classic Tetrad (FAAD)
All four features must be present together for the full syndrome:
| Feature | Description |
|---|---|
| Finger agnosia | Inability to name or identify individual fingers on either hand (e.g., cannot identify the index finger or ring finger when asked) |
| Agraphia (Dysgraphia) | Inability or difficulty in writing, in the absence of motor weakness or paralysis |
| Acalculia (Dyscalculia) | Impairment of arithmetic calculation ability |
| Right-Left disorientation | Inability to distinguish right from left on own body or on the examiner's body |
Key memory aid: "FAAD" - Finger agnosia, Agraphia, Acalculia, Disorientation (right-left)
- Adams and Victor's Principles of Neurology, 12th Ed., p. 107
- Neuroanatomy through Clinical Cases, 3rd Ed.
Anatomical Localization
The lesion is in the dominant (left) inferior parietal lobule, specifically:
- Angular gyrus (Brodmann area 39) - the primary site
- Subjacent white matter of the left hemisphere
- Located below the interparietal sulcus
- Supplied by the angular branch of the middle cerebral artery (inferior division)
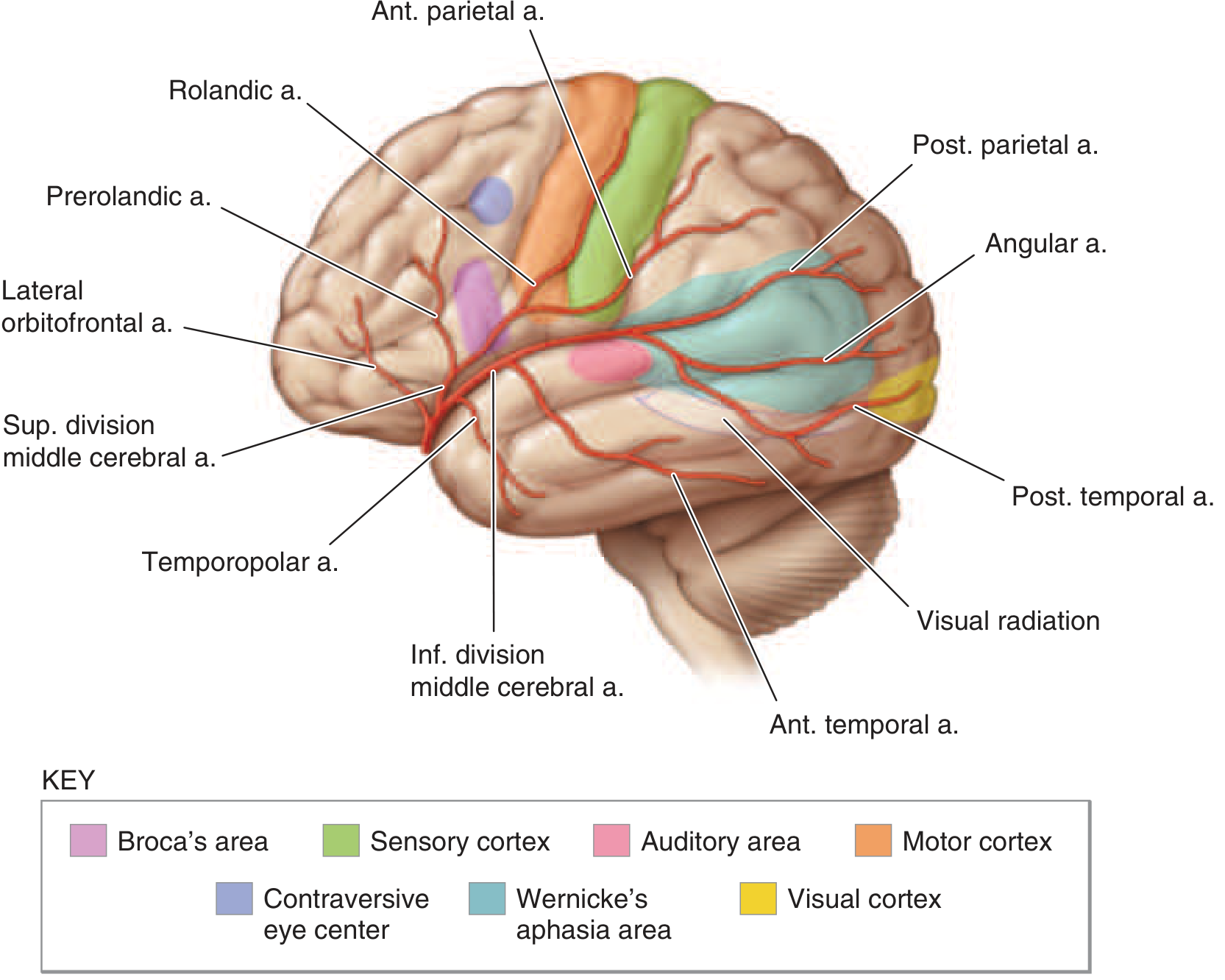
The angular gyrus sits at the junction of the temporal, parietal, and occipital lobes - a convergence zone for multimodal sensory integration. This explains why a single lesion here can produce deficits spanning language, spatial processing, and body schema.
- Harrison's Principles of Internal Medicine, 22nd Ed.
Key Diagnostic Point
Each of the four features, in isolation, has little specific localizing value and can be seen in many brain disorders. However, when all four occur together in the absence of global confusion or diffuse brain disease, the syndrome is strongly localizing to the dominant inferior parietal lobule.
Before diagnosing, it is important to confirm:
-
The finger naming deficit is not part of a generalized anomia
-
The patient is not globally aphasic (which would make all four features non-specific)
-
Harrison's Principles of Internal Medicine, 22nd Ed.
Associated Features
Gerstmann syndrome rarely occurs in isolation. Commonly associated deficits include:
- Alexia (reading impairment) - especially alexia with agraphia (central alexia)
- Aphasia (anomic or Wernicke's type) - from adjacent cortical involvement
- Contralateral visual field defect - lower quadrantanopia or homonymous hemianopia (involvement of optic radiations below)
- Constructional apraxia
- Ideomotor apraxia
"Gerstmann syndrome can occur as a relatively pure syndrome, but it is more often accompanied by other deficits localizing to the dominant inferior parietal lobule." - Neuroanatomy through Clinical Cases, 3rd Ed.
Etiology / Causes
The most common cause is stroke - specifically occlusion of the inferior division of the MCA or its angular branch. Other causes include:
- Ischemic stroke - MCA inferior division or angular artery occlusion (most common)
- Tumors - involving the left inferior parietal region
- Trauma - parietal cortex injury
- Abscess or infection
- Neurodegenerative disease - as part of posterior cortical atrophy or Alzheimer's disease affecting the parietal lobe
Pathophysiology / Controversy
There is an ongoing debate about whether the four features share a common underlying deficit or simply co-occur because of the proximity of their neural substrates:
-
Unitary hypothesis: Adams and Victor favor a single underlying defect in spatial orientation - of fingers, body sides, and numbers - explaining why all four features cluster together.
-
Localization-only hypothesis: Benton argued that they occur together no more often than other combinations of parietal deficits (constructional apraxia, alexia, visual memory loss) - suggesting co-occurrence is purely anatomical.
-
Functional imaging: Rusconi et al. could not identify a shared cortical substrate in healthy subjects, casting doubt on a unitary mechanism.
-
Adams and Victor's Principles of Neurology, 12th Ed.
Gerstmann Syndrome in MCA Stroke
In the context of dominant hemisphere MCA inferior division occlusion, Gerstmann syndrome appears alongside:
- Central aphasia (Wernicke-type)
- Word deafness, anomia, jargon speech
- Sensory agraphia, acalculia, alexia, finger agnosia, right-left confusion
"Central aphasia, word deafness, anomia, jargon speech, sensory agraphia, acalculia, alexia, finger agnosia, right-left confusion (the last four comprise the Gerstmann syndrome): central, suprasylvian speech area and parietooccipital cortex of the dominant hemisphere."
- Harrison's Principles of Internal Medicine, 22nd Ed.
Developmental Gerstmann Syndrome
A developmental form occurs in children and is not caused by an acquired lesion:
-
Presents with right-left disorientation, finger agnosia, dysgraphia, dyscalculia, and sometimes constructional apraxia
-
Occurs in approximately 2% of school-aged children
-
Children have generally normal IQ
-
~25% have comorbid ADHD, ~20% have dyslexia
-
Also called "specific learning disorder with impairment in mathematics" under DSM-5
-
Imaging shows parietal and frontal abnormalities, with weaker activation in the intraparietal sulcus (IPS)
-
Bradley and Daroff's Neurology in Clinical Practice, p. 1901
Comparison: Gerstmann vs. Klüver-Bucy
| Feature | Gerstmann Syndrome | Klüver-Bucy Syndrome |
|---|---|---|
| Lobe | Dominant parietal (inferior) | Bilateral temporal (anterior) |
| Key structure | Angular gyrus | Amygdala + temporal cortex |
| Laterality | Unilateral (dominant) | Bilateral |
| Core features | Finger agnosia, agraphia, acalculia, R-L disorientation | Visual agnosia, oral exploration, hypersexuality, tameness |
Key exam point: Gerstmann syndrome = dominant (left) angular gyrus lesion + tetrad of Finger agnosia + Agraphia + Acalculia + Right-Left disorientation. The full tetrad is strongly localizing; any single feature alone is not.
This is a shared conversation. Sign in to Orris to start your own chat.