Ectopic kidney with transverse vaginal septum to be worried?
Reading File
Finding Sources
Finding Sources
Searching the Web
ectopic kidney transverse vaginal septum association Mayer-Rokitansky urogenital anomalies
Reading File
Reading File
Searching PubMed
"ectopic kidney" AND "vaginal septum" OR "mullerian anomaly"
Loading Image
Finding Sources
I now have all the information needed for a thorough answer. Here is the full clinical picture:
Ectopic Kidney + Transverse Vaginal Septum: Should You Be Worried?
Yes - this combination is clinically significant and warrants a systematic workup. These two anomalies co-occurring are not coincidental; they share a common embryological origin and together they hint at a broader urogenital malformation spectrum that needs active investigation.
Why They Co-Occur: The Embryological Link
Both the urinary and genital tracts develop from closely related mesodermal structures during weeks 4-8 of embryogenesis:
- The kidney ascends from the pelvis as the metanephric blastema, guided by the ureteric bud (derived from the mesonephric/Wolffian duct).
- The vagina forms from fusion and canalization of the Mullerian (paramesonephric) ducts with the urogenital sinus.
Because the Mullerian and Wolffian ducts develop in parallel and share the same mesodermal ridge, an insult during this window disrupts both systems simultaneously. This is the basis of the MURCS association (Mullerian duct aplasia, Renal aplasia, Cervicothoracic Somite anomalies).
"The incidence of genital anomalies in the patient with ectopia is about 15%."
In MRKH syndrome (atypical form), renal anomalies including ectopic kidneys are seen in 40-60% of patients.
What the Transverse Vaginal Septum Tells You
The transverse vaginal septum (TVS) arises from failed fusion or canalization of the urogenital sinus and Mullerian ducts - a purely Mullerian problem. Its incidence is approximately 1 in 70,000 females.
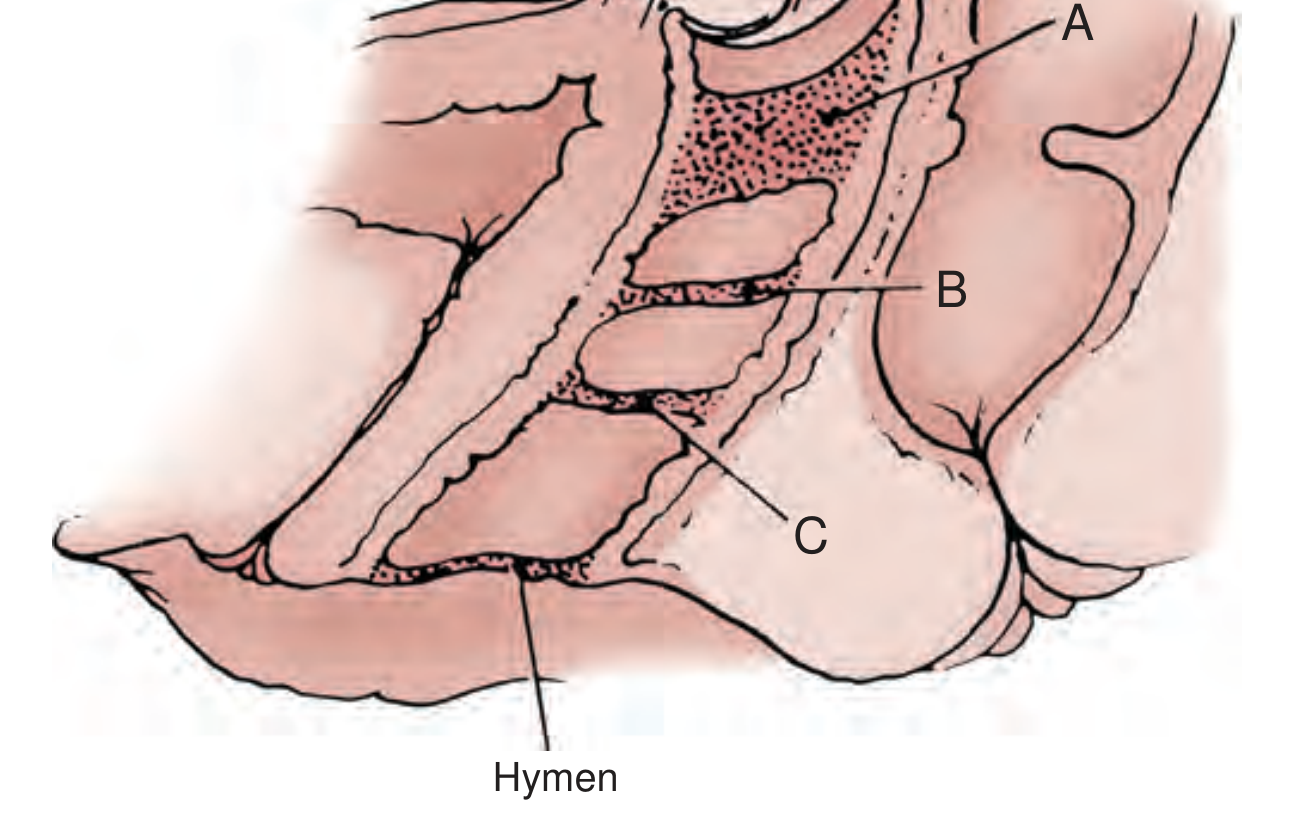
Transverse vaginal septum locations - Campbell-Walsh-Wein Urology
- 46% upper vagina, 40% middle, 14% lower third
- Usually < 1 cm thick; may have small eccentric perforation
- Even a perforated septum can cause significant obstruction and ascending infection
The TVS, when co-existing with an ectopic kidney, strongly flags a shared embryological defect and makes MURCS/MRKH spectrum the primary concern.
Key Concerns in This Clinical Combination
1. Obstructive Uropathy Risk
The ectopic kidney is at risk for:
- Hydronephrosis - from UPJ or UVJ obstruction, or malrotation-related kinking
- Vesicoureteral reflux (VUR) in 30-50% of ectopic kidneys (Campbell-Walsh)
- Recurrent UTIs due to urinary stasis
2. Outflow Tract Obstruction
A complete or near-complete TVS causes:
- Hematocolpos / hematometra - accumulation of menstrual blood, presenting as cyclic pelvic pain + primary amenorrhea
- Endometriosis from retrograde menstrual flow through the fallopian tubes if diagnosis is delayed (Deligeoroglou et al.)
- Ascending pelvic infection (pyocolpos) - a 2025 case report described TVS complicated by pyocolpos, VUR, and ectopic ureter with renal loss, emphasizing the need for a high index of suspicion
3. Associated Anomalies to Screen For (MURCS/MRKH Spectrum)
Finding both anomalies mandates systematic screening:
| System | Anomaly to Look For |
|---|---|
| Renal/urinary | Contralateral renal agenesis, VUR, ureteral duplication, UPJ obstruction |
| Uterus/cervix | Uterine agenesis, bicornuate/unicornuate uterus, cervical atresia |
| Spine | Scoliosis, Klippel-Feil anomaly, vertebral segmentation defects |
| Hearing | Sensorineural hearing loss (stapedial ankylosis) |
| Cardiac | Valve defects |
Workup Recommended
Imaging:
- MRI pelvis + abdomen - gold standard; defines septum thickness and level, uterine morphology, cervix presence (critical to differentiate high septum from cervical atresia - errors here cause significant morbidity), and renal position/morphology
- Renal ultrasound (DMSA scan) if ectopic kidney function is uncertain
- Voiding cystourethrogram (VCUG) if VUR is suspected
Clinical:
- Detailed pubertal and menstrual history (primary amenorrhea? cyclic pain?)
- Spine X-ray (scoliosis screening)
- Audiogram
Treatment of the TVS
Per Campbell-Walsh Urology:
- If hematocolpos pain is manageable, suppress endometrial activity with GnRH agonist or continuous OCP first - this dilates the lower vaginal segment and eases surgical repair
- Definitive treatment: surgical excision of the septum with Z-plasty or mucosal edge approximation
- Balloon-assisted division under ultrasound guidance is described for high/thick septa
Bottom Line
The co-occurrence of ectopic kidney and transverse vaginal septum is not coincidental and represents a marker of a broader urogenital malformation likely within the MURCS/MRKH spectrum. The immediate clinical concerns are:
- TVS causing outflow obstruction - diagnose and treat before endometriosis and pyocolpos develop
- Ectopic kidney with VUR or hydronephrosis - monitor renal function and screen for reflux
- Systematic screening for associated Mullerian, renal, skeletal, and cardiac anomalies
A multidisciplinary team (urology, gynecology, radiology, genetics) approach is strongly recommended.
Sources: Campbell-Walsh-Wein Urology, 12th ed.; PMC12166996 (2025 case report); MRKH + ectopic kidney MRI case; MURCS literature
This is a shared conversation. Sign in to Orris to start your own chat.