Fentanyl
Reading File
Finding Sources
Finding Sources
Searching PubMed
fentanyl opioid analgesic pharmacology
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive textbook content. Here is the full evidence-based overview:
Fentanyl
Classification & Chemistry
Fentanyl is a fully synthetic opioid of the phenylpiperidine class, chemically related to meperidine. It is a pure mu-opioid receptor (MOR) agonist with 80-100 times the analgesic potency of morphine. Sufentanil is approximately 10x more potent than fentanyl (~1000x vs. morphine). It has no intrinsic anxiolytic or amnestic properties.
- Lippincott Pharmacology, p. 718
- Roberts & Hedges' Clinical Procedures in Emergency Medicine
Pharmacokinetics (ADME)
| Parameter | Detail |
|---|---|
| Lipid solubility | Highly lipophilic; rapidly crosses the blood-brain barrier |
| Plasma t½ equilibration (plasma → CSF) | ~5 minutes |
| Onset (IV) | <30 seconds; peak effect 2-5 minutes |
| Duration (single dose) | 20-40 minutes |
| Protein binding | ~80% (plasma proteins); ~40% taken up by RBCs |
| Distribution | 3-compartment model; ~75% first-pass pulmonary uptake |
| Metabolism | Hepatic CYP3A4/5 → norfentanyl (inactive) via N-dealkylation; detectable in urine up to 48 h |
| Elimination t½ | 3-4 hours (single dose); significantly prolonged with large doses or prolonged infusions |
| Context-sensitive half-time | Increases rapidly with infusion duration; longer than alfentanil and sufentanil |
With prolonged infusions or large doses, drug accumulates in muscle and fat; redistribution back into plasma extends its duration toward the elimination half-life.
- Miller's Anesthesia 10e, p. 2803
- Goodman & Gilman's, ADME section
Mechanism of Action
Fentanyl is a full agonist at mu-opioid receptors (MOR) in the CNS and peripheral tissues. MOR activation:
- Inhibits adenylyl cyclase (decreases cAMP)
- Opens inward-rectifying K+ channels (hyperpolarization)
- Closes voltage-gated Ca2+ channels
- Net effect: decreased neuronal excitability and reduced neurotransmitter release
This produces analgesia, sedation, euphoria, respiratory depression, and antitussive effects.
Pharmacodynamics & Clinical Effects
CNS
- Potent analgesia; C50 for analgesia = 1-2 ng/mL
- t½ke0 for analgesic effect = 10-20 minutes (longer than EEG effect, t½ke0 ~6.5 min)
- Sedation and dose-dependent respiratory depression
- Does NOT cause amnesia at standard doses
Cardiovascular
- Decreases heart rate via vagal activation
- Modest decrease in blood pressure
- Does NOT release histamine - minimal myocardial depression
- This makes it preferred for cardiac surgery and hemodynamically unstable patients
Respiratory
- Dose-dependent respiratory depression; apnea precedes loss of consciousness
- Rapid IV injection (especially >5 mcg/kg bolus) can cause wooden chest / chest wall rigidity - diaphragm, chest wall, and upper airway rigidity impairing ventilation (more common in pediatric patients and with high doses)
- Delayed respiratory depression possible via enterohepatic circulation
Other
-
Nausea/vomiting: rare (advantage over morphine and meperidine)
-
Nasal pruritus: a commonly observed reaction
-
No histamine release
-
Goodman & Gilman's, p. 256-258
-
Roberts & Hedges', p. 728
Routes of Administration
| Route | Formulation / Use |
|---|---|
| IV | Most common; anesthesia, procedural sedation, ICU |
| Epidural / Intrathecal | Combined with local anesthetics for labor or postoperative pain |
| Transdermal patch | Chronic severe pain; onset delayed ≥12 h; offset prolonged; reservoir created in skin; changed every 48-72 h |
| Buccal tablet (Fentora) | Breakthrough cancer pain in opioid-tolerant patients; 100-800 mcg |
| Lozenge (Actiq) | Oral transmucosal; 200-1600 mcg; onset rapid via buccal mucosa |
| Intranasal | Breakthrough pain |
| Iontophoretic transdermal | Patient-controlled delivery |
- Lippincott Pharmacology, p. 718-719
- Barash's Clinical Anesthesia 9e, p. 1555
Clinical Uses
-
Anesthesia - intraoperative analgesia; dampens cardiovascular responses to laryngoscopy, intubation, skin incision; reduces inhalational agent and propofol requirements by ~50% at 1.5-3 mcg/kg IV. Should be given 5-10 min before anticipated noxious stimulus given the t½ke0.
-
Procedural sedation and analgesia (PSA) - preferred opioid in the ED; rapid onset, brief duration, hemodynamic stability, no histamine release. Often combined with midazolam or propofol. Fully reversible with naloxone.
-
Chronic pain - transdermal patch. Contraindicated in opioid-naive patients and for acute/postoperative pain.
-
Breakthrough cancer pain - transmucosal formulations (Actiq lozenge, Fentora buccal tab). Only for opioid-tolerant patients (defined as ≥60 mg oral morphine equivalent/day).
-
Cardiac surgery - high-dose fentanyl (5-75 mcg/kg) provides primary anesthesia with minimal cardiovascular depression.
-
Labor analgesia - IV or epidural in doses of 50-100 mcg/h; no significant neonatal effects on Apgar scores at these doses.
- Roberts & Hedges', Miller's Anesthesia 10e, Goodman & Gilman's
Dosing (Selected)
Adults:
- Procedural sedation: 1-2 mcg/kg IV (titrated)
- Anesthesia supplement: 1.5-3 mcg/kg IV; repeat dosing based on surgical duration
- High-dose cardiac anesthesia: 5-75 mcg/kg
Pediatrics (Harriet Lane Handbook, 23rd ed.):
- Neonates/young infants: 1-4 mcg/kg/dose IV Q2-4 h PRN (max 100 mcg/dose); continuous infusion 1-5 mcg/kg/hr
- Older infants/children: 1-2 mcg/kg/dose IV/IM Q30-60 min PRN (max 100 mcg/dose); infusion 1-3 mcg/kg/hr
Drug Interactions
- CYP3A4 inhibitors (e.g., azole antifungals, macrolides, ritonavir): increase fentanyl plasma levels and risk of toxicity
- CYP3A4 inducers (e.g., rifampin, carbamazepine): reduce fentanyl efficacy
- CNS depressants (benzodiazepines, alcohol, neuroleptics): enhanced sedation and respiratory depression - significantly increased apnea/hypoxia risk
- MAOIs: potentially severe hypotension and CNS excitation
- Propofol: co-administration reduces requirements of both drugs synergistically
Reversal & Overdose
- Fully reversible with naloxone (opioid antagonist)
- Chest wall rigidity: reverse with naloxone, positive pressure ventilation; if refractory, neuromuscular blocking agents (depolarizing or nondepolarizing) - ensure patient is not awake/aware when paralyzed
- Standard resuscitation: airway management, oxygen, IV naloxone 0.04-0.4 mg IV (titrate to avoid precipitating acute withdrawal in opioid-tolerant patients)
Key Contraindications
- Transdermal patch: opioid-naive patients, acute/postoperative pain (dangerous due to delayed onset and inability to titrate)
- Transbuccal/transmucosal forms: only for patients consuming ≥60 mg oral morphine equivalent/day
- Children <2 years: transdermal patch safety not established
Comparison to Related Opioids
| Drug | Potency vs. Morphine | Onset | Notes |
|---|---|---|---|
| Fentanyl | 100x | Very fast | Standard reference in this class |
| Sufentanil | 1000x | Very fast | Used in cardiac/complex cases |
| Alfentanil | ~10x | Fastest (low pKa) | Shortest context-sensitive t½ |
| Remifentanil | ~100x | 1-1.5 min | Metabolized by plasma esterases; ultra-short acting |
| Morphine | 1x (reference) | Slower (~15 min) | Releases histamine |
Sources: Lippincott Illustrated Reviews: Pharmacology; Miller's Anesthesia 10e; Goodman & Gilman's Pharmacological Basis of Therapeutics; Barash's Clinical Anesthesia 9e; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Harriet Lane Handbook 23e.
Remifentanyl
Finding Sources
Finding Sources
Searching PubMed
remifentanil pharmacology clinical use
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is the comprehensive evidence-based overview:
Remifentanil
Classification & Key Distinguishing Feature
Remifentanil is the first and only ultra-short-acting opioid in clinical use. It is a full mu-opioid receptor (MOR) agonist of the phenylpiperidine class - chemically related to fentanyl but structurally unique because of its methyl ester side chain, which renders it susceptible to rapid hydrolysis by nonspecific plasma and tissue esterases.
This single structural feature makes its pharmacokinetics unlike every other available opioid.
- Miller's Anesthesia 10e, p. 2805
Pharmacokinetics
Metabolism - The Defining Feature
| Feature | Detail |
|---|---|
| Metabolizing enzymes | Nonspecific plasma and tissue esterases (blood and RBCs) |
| NOT metabolized by | Liver (CYP450), pseudocholinesterase |
| Primary metabolite | GI90291 (carboxylic acid) - 0.001 to 0.003x (0.1-0.3%) the potency of remifentanil; renally excreted |
| Minor pathway | N-dealkylation to GI94219 |
| Hepatic/renal failure | Does NOT appreciably alter pharmacokinetics - no dose adjustment needed |
| Pseudocholinesterase deficiency | No effect on remifentanil metabolism (unlike succinylcholine) |
- Miller's Anesthesia 10e; Morgan & Mikhail's Clinical Anesthesiology 7e, p. 354
Key Kinetic Parameters
| Parameter | Remifentanil | vs. Fentanyl |
|---|---|---|
| Onset | 1-1.5 min | ~2-5 min |
| t½ke0 (effect-site equilibration) | 1-1.5 min | 4-5 min |
| Elimination t½ | 8-20 min | 3-4 h |
| Context-sensitive half-time | ~3-5 min (constant, regardless of infusion duration) | Increases sharply with infusion duration |
| Plasma protein binding | ~70% (mainly α1-acid glycoprotein) | ~80% |
| pKa | 7.07 | - |
| Recovery of respiratory function | 3-5 min after stopping infusion | Prolonged |
| Full recovery from all effects | Within 15 min | Hours (long infusions) |
- Barash's Clinical Anesthesia 9e, p. 2523; Goodman & Gilman's
Context-Insensitive Half-Life - The Clinical Advantage
The graph below illustrates the defining pharmacokinetic superiority of remifentanil: its time to 50% plasma concentration drop remains flat (~3 min) regardless of how long the infusion runs, while fentanyl's increases sharply after even short infusions.
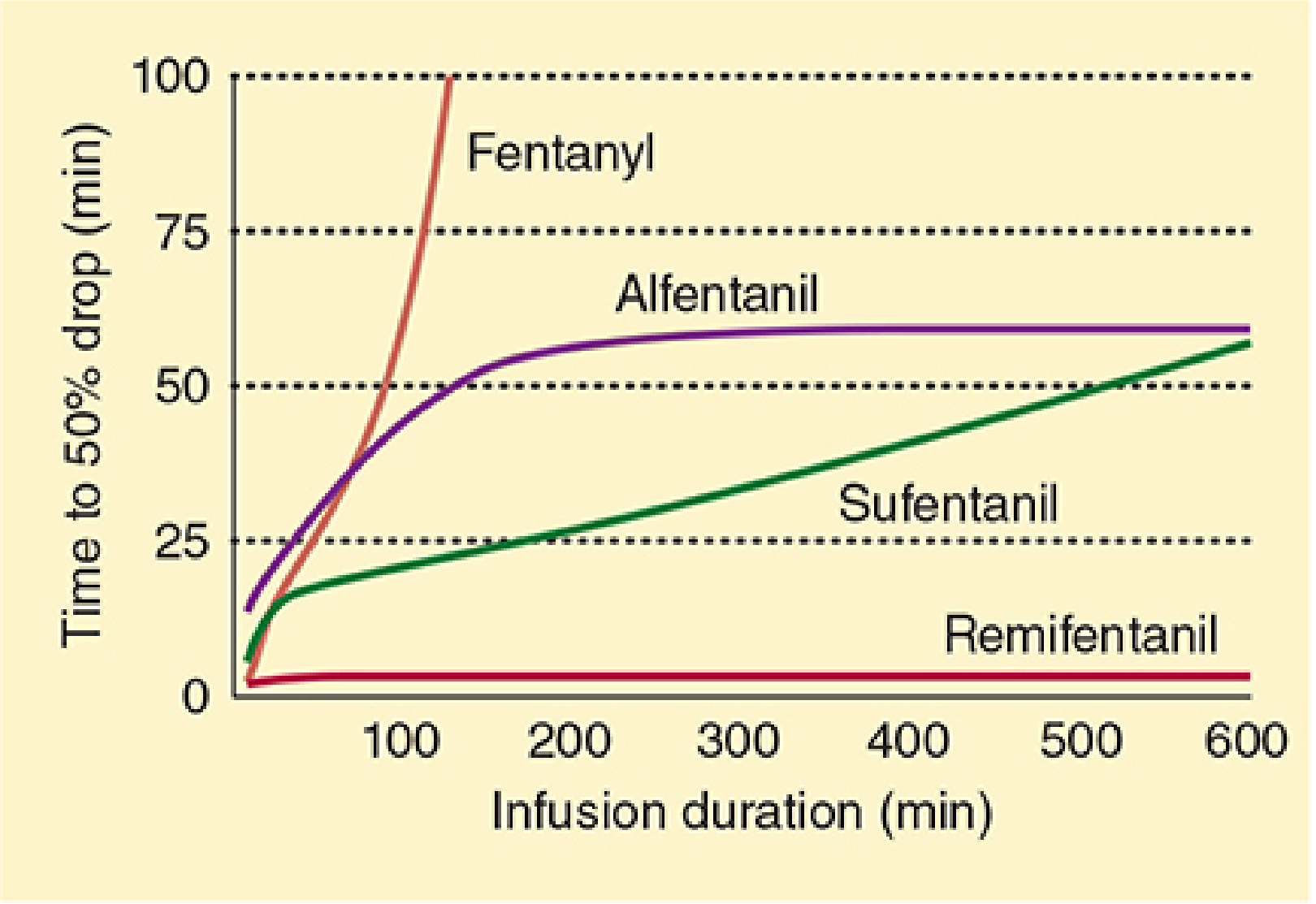
FIGURE: Time to 50% drop in plasma concentration vs. infusion duration for opioids. Remifentanil (bottom, flat) is uniquely context-insensitive. - Morgan & Mikhail's Clinical Anesthesiology 7e
Pharmacodynamics
Potency
- 100-200 times more potent than morphine at the MOR
- CP50 for no clinical response to surgical stimulation: highly variable (1.5-79 ng/mL) - a 50-fold range across patients
- Gender difference noted: CP50 ~4.1 ng/mL (men) vs. ~7.5 ng/mL (women) in one abdominal surgery study (attributable to procedural differences)
CNS
- Rapid, intense analgesia
- Dose-dependent sedation and respiratory depression
- No intrinsic amnesia - requires a hypnotic co-drug (propofol, midazolam)
- Reduces MAC of volatile agents significantly: remifentanil at 1 ng/mL target reduces sevoflurane MAC from ~4% to ~0.36% in some studies
- Reduces propofol requirements by >60% at therapeutic concentrations
Cardiovascular
- Decreases heart rate (vagal activation) and blood pressure
- Rapid bolus injection: risk of hypotension and bradycardia
- Low histamine release (hemodynamically stable)
Respiratory
- Dose-dependent respiratory depression
- Peak respiratory depression after bolus: ~5 min
- Recovery of spontaneous ventilation: rapid after infusion discontinuation or rate reduction
- Infusion rates of 0.1 ± 0.05 mcg/kg/min can maintain analgesia while permitting spontaneous ventilation
Chest Wall Rigidity
-
Can occur, especially with rapid bolus injection - related to peak concentration
-
Reverse with opioid antagonist, positive pressure ventilation, or neuromuscular blockade if needed
-
Barash's Clinical Anesthesia 9e; Miller's Anesthesia 10e
Formulation - Critical Restriction
Remifentanil is formulated with glycine as a carrier. Glycine is an inhibitory neurotransmitter in the dorsal horn of the spinal cord and causes reversible motor weakness when injected intrathecally in animal models. Therefore:
Remifentanil is CONTRAINDICATED for epidural or intrathecal (spinal) administration.
This is a hard stop - no intraspinal use regardless of clinical need.
- Goodman & Gilman's; Miller's Anesthesia 10e, p. 2806
Clinical Uses
1. Balanced General Anesthesia
- Continuous IV infusion: 0.1-1.0 mcg/kg/min for intraoperative analgesia
- Allows "most predictable and rapid trouble-free emergence" without postoperative respiratory depression
- Synergistic with propofol (TIVA) and volatile agents
- Dose adjusted between stimulation events (e.g., lower between intubation and incision)
2. Total Intravenous Anesthesia (TIVA) with Propofol
- Gold standard pairing; both drugs have short context-sensitive half-times allowing deep intraoperative analgesia without prolonged emergence
- Induction: remifentanil 2 mcg/kg with propofol; maintenance: 0.25-0.5 mcg/kg/min
3. Monitored Anesthesia Care (MAC) / Procedural Sedation
- Ideal for brief, painful procedures under regional or local anesthesia
- Clinical target: analgesia and patient comfort, not sedation
- Add midazolam (2 mg IV) or propofol for the hypnotic-amnesic component; midazolam reduces remifentanil requirements by up to 50%
- Practical infusion rates for MAC sedation: ~0.05-0.1 mcg/kg/min
4. ICU Sedation/Analgesia
- Short-term analgesia and sedation; rapidly titratable
5. Cardiac Surgery
- Induction: remifentanil 2 mcg/kg + propofol; maintenance: 0.25-0.5 mcg/kg/min for minimally invasive CABG
6. Neuroanesthesia
- Used where rapid neurological assessment post-procedure is needed
7. Spontaneously Breathing Patients
-
Feasible at low infusion rates (<0.1-0.2 mcg/kg/min) with appropriate monitoring
-
Miller's Anesthesia 10e; Barash's Clinical Anesthesia 9e
Dosing Summary
| Indication | Dose |
|---|---|
| Induction supplement | 0.5-1 mcg/kg IV over 30-60 sec (avoid rapid bolus) |
| Intraoperative maintenance (infusion) | 0.1-1.0 mcg/kg/min; titrate |
| TIVA (with propofol) | 0.25-0.5 mcg/kg/min |
| MAC / procedural sedation | 0.025-0.1 mcg/kg/min |
| Spontaneously breathing patients | <0.1-0.2 mcg/kg/min with monitoring |
The Post-Remifentanil Analgesia Problem
This is a clinically important and unique pitfall: because remifentanil disappears so rapidly after stopping, postoperative pain can be severe and abrupt if no bridging analgesia is in place.
Plan required before stopping remifentanil:
- Administer a longer-acting opioid (morphine, fentanyl) 15-30 min before the end of surgery
- Add NSAIDs, acetaminophen, regional blocks as part of multimodal analgesia
- Failure to plan leads to immediate, intense post-emergence pain
"The need for alternative analgesic therapies should be anticipated and administered in a timely fashion" - Miller's Anesthesia 10e
Opioid-Induced Hyperalgesia (OIH)
-
High-dose or prolonged remifentanil infusions can paradoxically lower the pain threshold after discontinuation - a phenomenon known as remifentanil-induced hyperalgesia
-
Mechanism: central sensitization via NMDA receptors
-
Management: ketamine (0.15 mg/kg bolus + 2 mcg/kg/min infusion) reduces intraoperative remifentanil requirements AND postoperative morphine consumption without adding side effects
-
PubMed 2024 systematic review confirmed pharmacological interventions for remifentanil-induced hyperalgesia remain an active area of research [PMID: 39636808]
-
Miller's Anesthesia 10e, p. 2837
Drug Interactions
| Interaction | Effect |
|---|---|
| Midazolam | Reduces remifentanil requirements by up to 50% |
| Propofol | Synergistic; each reduces the other's dose requirement |
| Volatile anesthetics (sevoflurane, isoflurane) | Reduces MAC significantly |
| Ketamine | Reduces OIH and postoperative opioid consumption |
| CNS depressants (benzodiazepines, alcohol) | Enhanced respiratory depression |
| MAOIs | Potential for severe adverse reactions (class effect) |
Special Populations
| Population | Consideration |
|---|---|
| Hepatic failure | No dose adjustment required |
| Renal failure | No dose adjustment for remifentanil itself; metabolite GI90291 is renally cleared but has negligible potency |
| Pseudocholinesterase deficiency | No effect - remifentanil is NOT a pseudocholinesterase substrate |
| Obese patients | Dose based on lean body weight (similar principle to other opioids) |
| Elderly | Age can affect clearance; titrate carefully |
| Pediatric | Used; dosing weight-based; MAC reduction data in children documented |
Summary Comparison: Remifentanil vs. Other Fentanyl Congeners
| Drug | Potency (vs. morphine) | t½ke0 | Context-Sensitive t½ | Metabolism | Spinal use |
|---|---|---|---|---|---|
| Remifentanil | 100-200x | 1-1.5 min | ~3 min (flat) | Plasma/tissue esterases | Contraindicated |
| Fentanyl | 100x | 4-5 min | Rises steeply | CYP3A4 (liver) | Yes |
| Alfentanil | ~10x | 0.6-1.2 min | Plateaus ~55 min | CYP3A4 (liver) | Yes |
| Sufentanil | 1000x | ~6 min | Rises slowly | CYP3A4 (liver) | Yes |
Sources: Miller's Anesthesia 10e; Barash, Cullen & Stoelting's Clinical Anesthesia 9e; Goodman & Gilman's Pharmacological Basis of Therapeutics; Morgan & Mikhail's Clinical Anesthesiology 7e
This is a shared conversation. Sign in to Orris to start your own chat.