sensitivity of chemoreceptors towards hypoxia
Reading File
Finding Sources
Finding Sources
Searching PubMed
peripheral chemoreceptor hypoxia sensitivity
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive, well-illustrated content from two authoritative physiology textbooks. Let me compile the full answer.
Sensitivity of Chemoreceptors to Hypoxia
Overview
Chemoreceptors involved in respiratory control are divided into peripheral and central types. Of these, only the peripheral chemoreceptors (carotid and aortic bodies) are sensitive to hypoxia. The central chemoreceptors in the medulla respond primarily to CO2/H+ and are essentially insensitive to hypoxia.
Peripheral Chemoreceptors - Anatomy and Blood Supply
The carotid bodies sit at the bifurcation of the common carotid arteries; the aortic bodies lie along the underside of the aortic arch. Three features make them ideal oxygen sensors:
- Extremely small - each carotid body weighs only ~2 mg
- Extraordinarily high blood flow - ~40x higher than the brain (normalized for weight); this means they are always bathed in arterial, not venous, blood
- High metabolic rate - 2-3x that of the brain, yet blood flow is so much greater that capillary PO2 closely mirrors arterial PO2
Afferents travel via the glossopharyngeal nerve (CN IX) from carotid bodies and the vagus nerve (CN X) from aortic bodies to the nucleus tractus solitarius (NTS) in the medulla. (Corneille Heymans won the 1938 Nobel Prize for establishing their chemoreceptor function.)
- Medical Physiology (Boron & Boulpaep), p. 1059-1060
The Glomus Cell - The Actual Oxygen Sensor
The chemosensitive cells are type I (glomus) cells - ~10 µm spherical neuroectodermal cells that:
- Have voltage-gated K+ and Ca2+ channels
- Generate action potentials upon depolarization
- Store neurotransmitters (acetylcholine, dopamine, norepinephrine, substance P, ATP) in intracellular vesicles
Cellular Mechanism of Hypoxia Detection
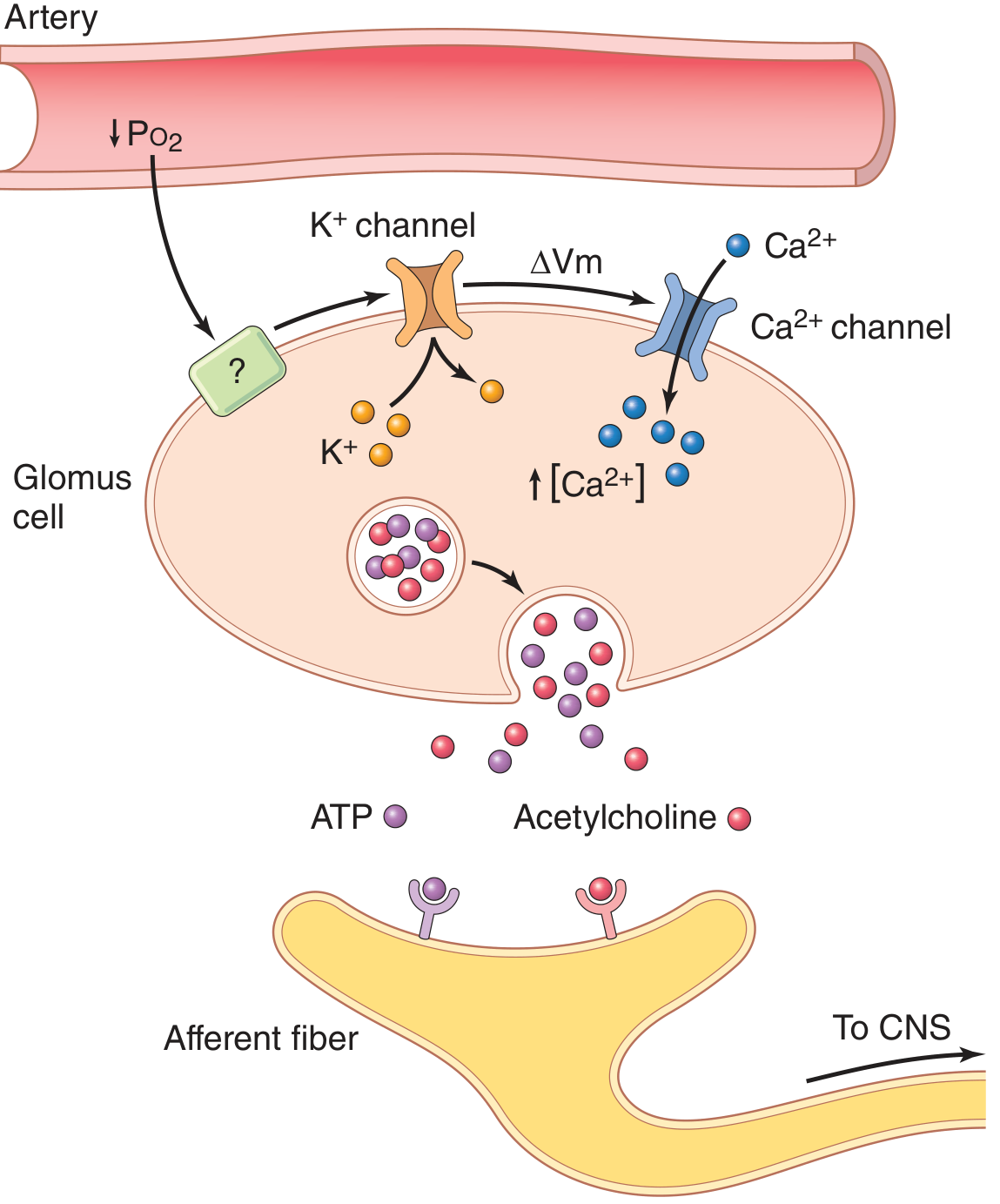
When arterial PO2 falls below ~60 mm Hg:
- Low PO2 detected by an O2-sensitive sensor (mechanism not fully resolved) → K+ channels close
- Closure of K+ channels → cell depolarizes (ΔVm)
- Depolarization → voltage-gated Ca2+ channels open → intracellular [Ca2+] rises
- Elevated [Ca2+] → exocytosis of neurotransmitters (ATP is likely the primary excitatory transmitter; dopamine and acetylcholine also released)
- Neurotransmitters activate afferent fibers of the carotid sinus nerve → signals sent to CNS → increased ventilation
- Guyton and Hall Textbook of Medical Physiology, p. 536
PO2 Range of Sensitivity
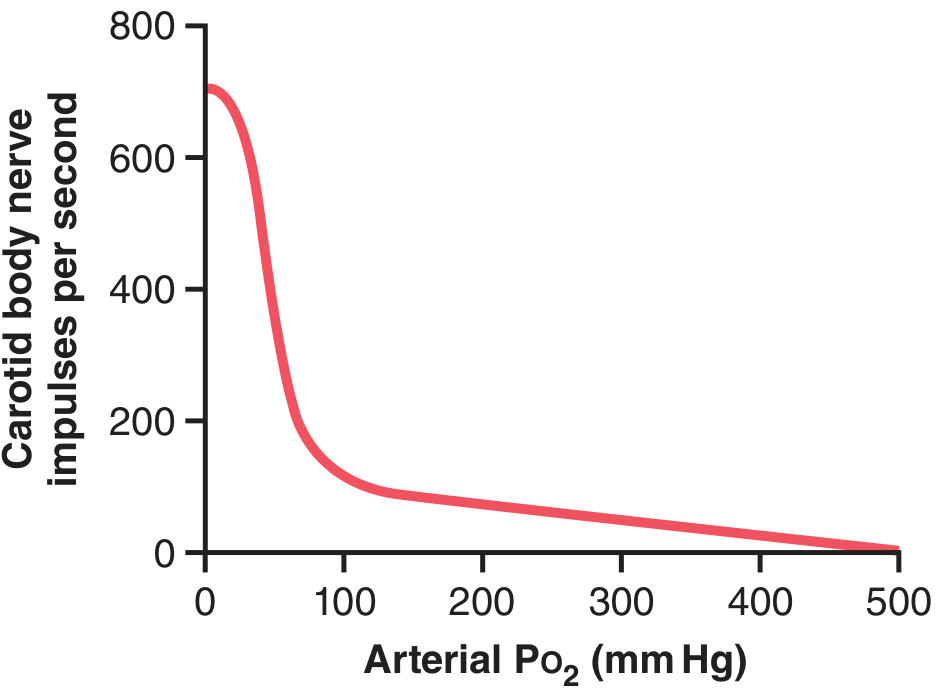
Key characteristics:
- Above ~100 mm Hg (normal): raising PO2 further has trivial effect on firing rate
- PO2 60-30 mm Hg: the most sensitive range - firing rate rises steeply. This corresponds precisely to the steep portion of the oxyhemoglobin dissociation curve where Hb saturation falls rapidly
- Below 30 mm Hg: near-maximal stimulation
Important distinction: The chemoreceptors respond to dissolved PO2 in plasma, not to oxygen content or hemoglobin saturation. This is why anemia (low Hb) or CO poisoning (Hb bound to CO) do not trigger strong peripheral chemoreceptor stimulation - PaO2 remains normal even though O2 delivery is compromised.
- Medical Physiology, p. 1059; Guyton and Hall, p. 536
Modulation of Hypoxic Sensitivity by PCO2 and pH
This is the most clinically important aspect of chemoreceptor physiology:
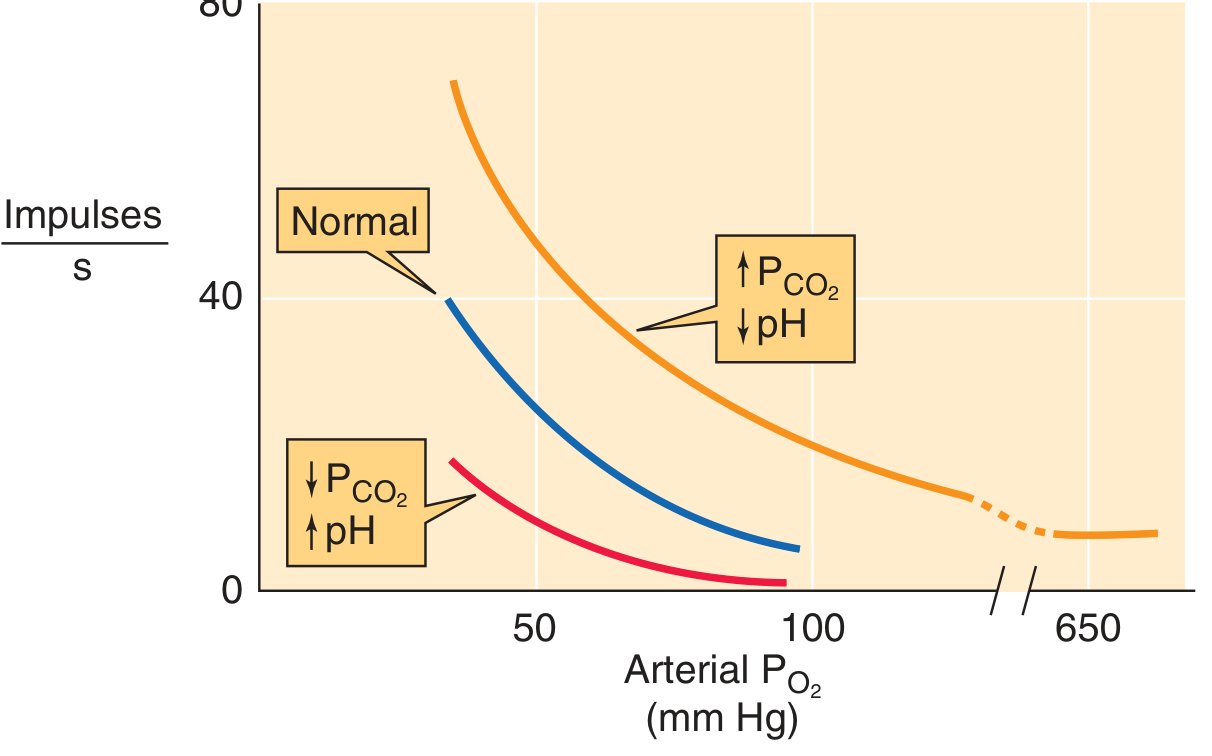
- Respiratory acidosis (↑PCO2 / ↓pH) - shifts the curve upward and leftward (orange curve): the carotid body fires more at any given PO2, and becomes more sensitive to hypoxia (steeper slope)
- Normal acid-base - baseline response (blue curve)
- Respiratory alkalosis (↓PCO2 / ↑pH) - shifts the curve downward and rightward (red curve): sensitivity to hypoxia is blunted
The mechanism: respiratory acidosis directly sensitizes the glomus cell membrane, making K+ channels even more susceptible to closure by low PO2.
This bidirectional interaction is clinically relevant: hypoxia also sensitizes the peripheral chemoreceptor response to CO2 (the curves become steeper when hypoxia coexists with hypercapnia).
- Medical Physiology, p. 1059, 2833
Integrated Ventilatory Responses
Hypoxia + Respiratory Acidosis Together
When both hypoxia and respiratory acidosis occur together (as in severe pulmonary disease):
- At any given PCO2, hypoxia raises baseline ventilation (peripheral chemoreceptor activation)
- Hypoxia increases the slope of the ventilation-PCO2 curve - meaning the ventilatory response per unit rise in PCO2 is amplified
- This synergy is partly explained by peripheral chemoreceptors becoming more sensitive to both stimuli when they coexist
Central chemoreceptors account for 65-80% of the ventilatory response to CO2 under normoxic conditions, but their response is slow (minutes). Peripheral chemoreceptors are faster (seconds) but contribute less to CO2 responses.
Factors That Decrease Chemoreceptor Sensitivity to Hypoxia
| Factor | Effect |
|---|---|
| Respiratory alkalosis | Blunted hypoxic response |
| Volatile anesthetics (≥1 MAC) | Near-complete suppression (dose-dependent) |
| Opioids | Significant blunting |
| Residual neuromuscular block (postoperative) | Decreased sensitivity |
| Carotid body denervation | Abolishes hypoxic ventilatory response |
| Chronic hypoxia (high altitude, cyanotic CHD) | Adaptation leads to diminished response |
| Growth hormone deficiency | Depressed peripheral chemoreceptor sensitivity |
- Miller's Anesthesia, p. block 6, block 15; Murray & Nadel's Respiratory Medicine
Central vs. Peripheral Chemoreceptors: Hypoxia Summary
| Feature | Peripheral (Carotid/Aortic Bodies) | Central (Medullary) |
|---|---|---|
| Sensitivity to hypoxia | Primary O2 sensor | Essentially none |
| Sensitivity to CO2/H+ | Yes, but less powerful than central | Primary CO2 sensor (65-80% of CO2 response) |
| Speed of response | Rapid (seconds) | Slow (minutes) |
| Key PO2 threshold | ~60 mm Hg (steep response begins) | Not applicable |
| Sensing molecule | Dissolved PaO2 | CSF/brain interstitial H+/CO2 |
The peripheral chemoreceptors, especially the carotid bodies, thus function as finely tuned arterial O2 sensors that trigger rapid ventilatory adjustments when PaO2 falls below ~60 mm Hg, and their sensitivity is powerfully amplified by coexisting hypercapnia or acidosis.
How do anesthetics suppress chemoreceptor hypoxic sensitivity mechanistically?
Finding Sources
Finding Sources
Searching PubMed
volatile anesthetic carotid body glomus cell hypoxia mechanism
Finding Sources
Finding Sources
Searching PubMed
anesthetics hypoxic ventilatory response suppression mechanism
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
carotid body volatile anesthetic TASK channel glomus
Reading File
Reading Article
PMID: 32826405
Reading Article
PMID: 20217350
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive mechanistic answer. Compiling the full response.
How Anesthetics Suppress Chemoreceptor Hypoxic Sensitivity - Mechanisms
The suppression occurs at two distinct levels: (1) the peripheral chemoreceptor itself (carotid body glomus cell) and (2) central integration of chemoreceptor signals in the brainstem. Different anesthetic classes act predominantly at one or both of these sites.
1. Volatile Anesthetics - Primary Target: the Glomus Cell
The Core Problem They Exploit: K+ Channel Closure
Recall the normal hypoxic sensing sequence in glomus cells:
Low PO2 → K+ channels close → depolarization → Ca2+ influx → neurotransmitter release → afferent firing
Volatile anesthetics short-circuit this sequence at the very first step by activating TASK (Two-pore-domain Acid-Sensitive K+) background potassium channels in glomus cells.
TASK Channel Activation: The Primary Mechanism
TASK channels (specifically TASK-1 and TASK-3) are the background K+ channels that normally close in response to hypoxia, initiating glomus cell depolarization. Research by Pandit et al. in Anesthesiology (2020) established:
- Volatile anesthetics activate (open) TASK channels, increasing their open probability well above baseline
- Halothane at 4% increased TASK channel open probability by ~226% above control
- Isoflurane at the same concentration increased it by a lesser degree (~50% in background channel recordings)
- By holding K+ channels open, the anesthetic opposes the hypoxia-driven closure - the glomus cell cannot depolarize, and the entire cascade downstream is blocked
The potency of different agents to open TASK channels directly parallels their potency to depress the hypoxic ventilatory response in whole humans - a powerful mechanistic confirmation.
Ca2+ Entry is Also Blocked
Even if some depolarization occurs, volatile anesthetics secondarily reduce the Ca2+ transient by:
- Reducing voltage-gated Ca2+ channel conductance
- Halothane reduced the Ca2+ response to a strong depolarizing stimulus (100 mM K+) by 44%, isoflurane by ~10%, indicating an additional Ca2+ channel-level effect (Pandit et al., 2010, Adv Exp Med Biol)
Dose-Response and Agent Comparison
The suppression is dose-dependent but begins at strikingly low concentrations:
Even 0.1 MAC of volatile anesthetics depresses the hypoxic ventilatory response by 25-75% - Barash Clinical Anesthesia, p. 1435
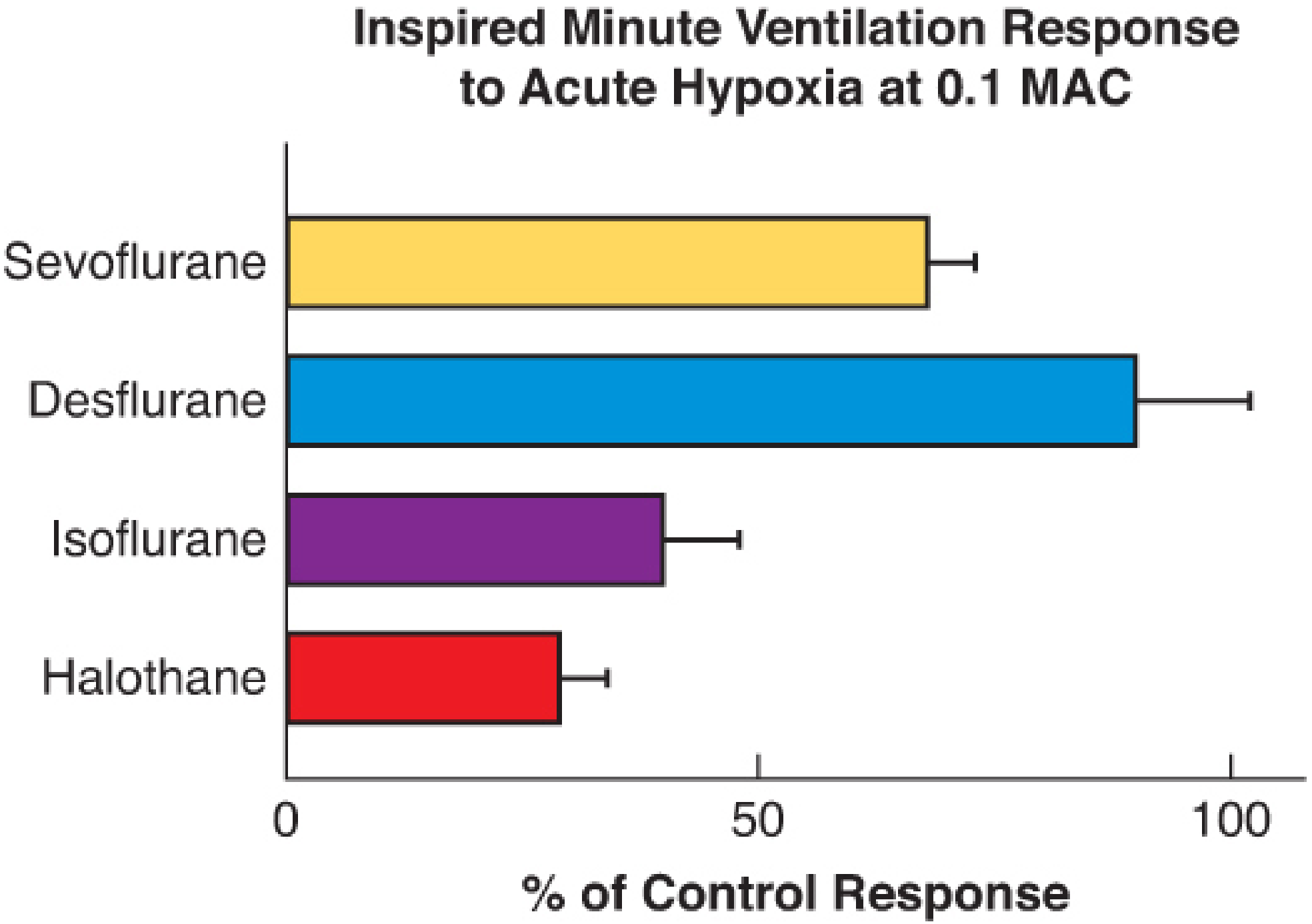
At 0.1 MAC:
- Halothane and isoflurane: ~60-65% depression (potent TASK openers)
- Sevoflurane: ~40-50% depression
- Desflurane: minimal effect at subanesthetic concentrations (weak TASK activator)
At ≥1 MAC, the peripheral chemoreflex loop is completely abolished - breathing depends entirely on automatic pontomedullary control and central chemoreceptor CO2 drive. - Miller's Anesthesia, 10e, p. 2134
Why the Peripheral Chemoreceptor is Disproportionately Affected
An important asymmetry: volatile anesthetics spare the central chemoreceptors at low doses. At 0.1 MAC of isoflurane and sevoflurane, peripheral chemoreflex sensitivity is already impaired with no change in central CO2 sensitivity. This selectivity arises because:
- TASK-1 and TASK-3 are highly expressed in glomus cells
- Central chemoreceptor neurons express different background K+ channel subtypes
- The central chemoreflex loop is only substantially affected above 1 MAC
2. Propofol - Direct Carotid Body Action + Ca2+ Pathway Inhibition
Propofol at maintenance infusion rates (50-120 mcg/kg/min) depresses the hypoxic ventilatory response "presumably by a direct action on carotid body chemoreceptors" - Miller's Anesthesia, 10e, p. 2475.
The cellular mechanism overlaps with but is distinct from volatile anesthetics:
- Propofol inhibits receptor-coupled signal transduction through inositol phosphate generation
- It blocks Ca2+ mobilization directly in the glomus cell
- It potentiates K+(ATP)-mediated pathways, which helps hold cells hyperpolarized
Because propofol's primary anesthetic target is GABA-A receptors (not TASK channels), its carotid body suppression is less potent per unit of anesthetic depth than halothane but still clinically significant.
3. Opioids - Primarily Central, with Some Peripheral Contribution
Opioids suppress hypoxic drive by a fundamentally different mechanism compared to volatile anesthetics.
Central Brainstem Mechanism (Primary)
Opioids bind µ-opioid receptors on neurons in brainstem respiratory centers:
- The preBötzinger complex (PreBötC) - the main respiratory rhythm generator - is a key target
- µ-receptor activation opens Gi-coupled GIRK (G protein-coupled inwardly rectifying K+) channels → hyperpolarization of respiratory neurons
- This directly depresses respiratory rate (more than tidal volume) and raises the apneic threshold
- The hypoxic drive is decreased because opioids blunt the brainstem's ability to convert peripheral chemoreceptor afferent signals into ventilatory output
Morgan and Mikhail, Clinical Anesthesiology, 7e, p. 357; Miller's Anesthesia, 10e, p. 2756
NTS Integration is Impaired
The carotid sinus nerve afferents first synapse in the nucleus tractus solitarius (NTS). µ-opioid receptors are expressed on NTS neurons, and opioid binding here reduces the gain of chemoreceptor signal transmission upstream to respiratory pattern generators.
Comparison with Volatile Anesthetics
| Feature | Volatile Anesthetics | Opioids |
|---|---|---|
| Primary site | Glomus cell (peripheral) | Brainstem/NTS (central) |
| Molecular target | TASK-1/TASK-3 K+ channels | µ-receptor → GIRK channels |
| Dose threshold | As low as 0.1 MAC | Dose-dependent (even analgesic doses) |
| Pattern of depression | Rate + volume both affected | Rate primarily (prolonged expiration) |
| Reversibility | Rapid washout (especially desflurane/sevo) | Naloxone-reversible |
| CO2 response | Preserved at low doses | Blunted (curve shifts right and down) |
4. Residual Neuromuscular Block - Indirect Peripheral Mechanism
An often-overlooked contributor: residual NMB at the nicotinic acetylcholine receptors of the carotid body directly reduces chemoreceptor sensitivity. The carotid body glomus cells have nicotinic cholinergic receptors involved in efferent modulation, and NMB agents interfere with this signaling pathway - contributing to the 33-64% incidence of impaired hypoxic response in post-anesthesia care units. - Fishman's Pulmonary Diseases, p. block 21
Clinical Takeaways
- The extreme subanesthetic sensitivity of the hypoxic response to volatile anesthetics (suppressed at 0.1 MAC) means residual drug in fat and muscle depresses hypoxic drive for hours after apparent emergence - dangerous in patients with chronic hypercapnia or OSA who depend on hypoxic drive
- Desflurane and sevoflurane are less suppressant at subanesthetic concentrations and wash out faster, making them preferable in at-risk patients
- Opioid + volatile anesthetic combinations are synergistic in suppressing both hypoxic and hypercapnic drives - not merely additive
This is a shared conversation. Sign in to Orris to start your own chat.