gullian barre synd
Reading File
Finding Sources
Searching PubMed
"Guillain-Barre syndrome"[MeSH Terms] AND treatment
Finding Sources
Reading File
Reading File
Reading File
Searching Images
Guillain-Barre syndrome nerve pathology demyelination
I have comprehensive information. Let me compile a thorough, well-structured answer on Guillain-Barré Syndrome.
Guillain-Barré Syndrome (GBS)
Overview
GBS is an acute immune-mediated polyradiculoneuropathy — the leading cause of acute paralytic disease in Western countries since the near-eradication of polio. Annual incidence is ~1.8 per 100,000. Males > females (1.5:1). Incidence increases with age (0.8/100,000 in <18 yrs → 3.2/100,000 in >60 yrs).
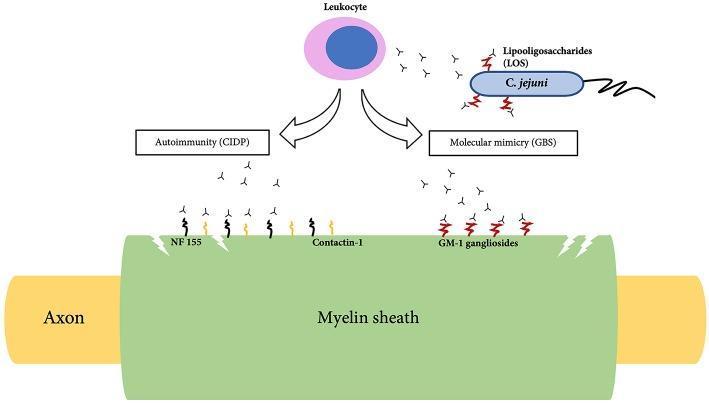
Pathophysiology
About two-thirds of cases are triggered by a preceding infection, occurring 1–4 weeks before neurological onset. The infection provokes microbe-specific T cells and antibodies that cross-react with nerve antigens (molecular mimicry).
Key triggers:
- Campylobacter jejuni (most common bacterial trigger — associated with axonal subtypes via GM1 ganglioside antibodies)
- Epstein-Barr virus, CMV, HIV, Zika virus, SARS-CoV-2
- Vaccines (rare association)
The pathological injury centers on spinal roots and proximal nerve segments, with mononuclear (macrophage-rich) infiltrates causing demyelination. In axonal subtypes, the attack targets the axolemma directly.
Subtypes (Box 106.11 — Bradley & Daroff's Neurology)
| Subtype | Key Features |
|---|---|
| AIDP (Acute Inflammatory Demyelinating Polyneuropathy) | Most common in Europe/North America; demyelinating |
| AMAN (Acute Motor Axonal Neuropathy) | Pure motor; epidemics in northern China in children; anti-GM1 antibodies |
| AMSAN (Acute Motor-Sensory Axonal Neuropathy) | Motor + sensory axonal; severe, poor recovery |
| Miller-Fisher Syndrome | Ophthalmoplegia, ataxia, areflexia triad; anti-GQ1b antibodies; 6% of GBS in West, up to 18% in Taiwan |
| Pharyngeal-cervical-brachial variant | Descending pattern |
| Facial diplegia with paresthesias | Cranial-predominant |
| Acute pandysautonomia | Pure autonomic involvement |
Clinical Features
Classic presentation:
- Ascending symmetrical weakness beginning in the lower limbs, spreading proximally over hours to days
- Areflexia/hyporeflexia — invariable feature (may be absent very early)
- Paresthesias in hands and feet — sensory loss is usually mild
- Progression peaks by 4 weeks (most reach nadir by 2–4 weeks)
Cranial nerve involvement: 45–75% of cases
- Bilateral facial paresis in ≥50%
- Extraocular muscle involvement (especially in MFS)
- Lower cranial nerve palsies (dysphagia, dysarthria)
Respiratory failure: 9–30% of hospitalized patients require ventilation (risk increases with age and disease severity)
Pain: Moderate–severe pain in extremities, interscapular region, or back in ~70% during the acute phase; may persist ≥1 year in a third of patients.
Autonomic dysfunction (65% of hospitalized patients):
- Orthostatic hypotension, urinary retention, GI atony
- Tachyarrhythmias, sinus tachycardia
- Bradycardia, heart block, asystole from vagal spells (can be triggered by tracheal suctioning)
- ECG changes: T-wave abnormalities, ST depression, QT prolongation, heart block
Diagnosis
Required Features (Asbury & Cornblath Criteria)
- Progressive weakness of both legs and arms
- Areflexia or hyporeflexia
Supportive Clinical Features
- Progression over days to ≤4 weeks
- Relative symmetry
- Mild sensory symptoms
- Bifacial palsies
- Autonomic dysfunction
- Absence of fever at onset
- Recovery beginning 2–4 weeks after progression ceases
Laboratory/Investigation Findings
| Test | Finding |
|---|---|
| CSF | Elevated protein, <10 cells/μL (albuminocytological dissociation) — hallmark |
| Nerve conduction studies | Slowed conduction velocity (demyelination) or reduced amplitude (axonal), conduction blocks |
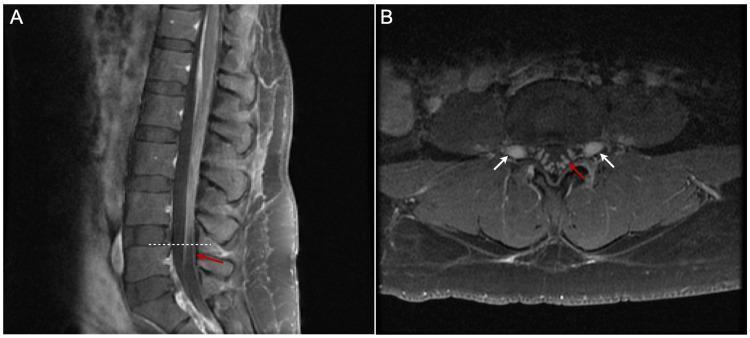
| MRI spine with contrast | Enhancement of cauda equina/nerve roots (breakdown of blood-nerve barrier) |
| Anti-ganglioside antibodies | Anti-GQ1b in MFS; Anti-GM1 in AMAN |
Treatment
Disease-Modifying Therapy
- Intravenous Immunoglobulin (IVIg) — 0.4 g/kg/day × 5 days (most widely used; suppresses immune response via multiple mechanisms)
- Plasmapheresis (plasma exchange) — removes offending antibodies; equally effective to IVIg; typically 5 exchanges over 2 weeks
- Combination of both offers no additional benefit over either alone
- Corticosteroids — NOT effective (do not alter outcome; may worsen it)
Supportive Care
- Respiratory monitoring: Forced vital capacity (FVC) every 4–6 hrs; intubate if FVC <15–20 mL/kg, rapid decline, or bulbar compromise ("20-30-40 rule")
- Cardiac monitoring (continuous ECG) for autonomic dysfunction
- DVT prophylaxis (subcutaneous heparin + compression stockings)
- Nutrition, pain management (gabapentin, carbamazepine, opioids)
- Physiotherapy and rehabilitation
Prognosis
- Mortality: ~1–5% (down from 33% before positive-pressure ventilation was introduced)
- Most patients recover over weeks to months
- ~15–20% have residual significant disability at 1 year
- Poor prognostic factors: older age, rapid onset, requirement for ventilation, severe axonal involvement, C. jejuni preceding infection, low CMAP amplitude
A 2025 systematic review (PMID: 39377571) identified older age, rapid clinical progression, and need for mechanical ventilation as major predictors of worse GBS outcomes.
Key Differentials
| Condition | Distinguishing Features |
|---|---|
| CIDP | Same demyelinating process but >2 months duration; chronic/relapsing course |
| Poliomyelitis | Fever at onset, asymmetric, CSF pleocytosis |
| Transverse myelitis | Spinal cord signs, sensory level, bladder involvement early |
| Botulism | Descending paralysis, pupillary involvement, no sensory symptoms |
| Myasthenia gravis | Fatigable weakness, no CSF changes, NCS normal |
Sources: Bradley and Daroff's Neurology in Clinical Practice; Robbins & Kumar Basic Pathology (9780323790185)
reactive arthritis
Finding Sources
Searching PubMed
"reactive arthritis"[MeSH Terms] AND management
Reading File
Reading File
Searching Images
reactive arthritis skin lesions keratoderma balanitis
Reading File
Finding Sources
Reading File
I now have comprehensive material for a full answer. Here it is:
Reactive Arthritis (ReA)
Definition
Reactive arthritis is an aseptic inflammatory arthritis that develops after an extra-articular infection — most commonly of the genitourinary or gastrointestinal tract — with a latency of 1–3 weeks between infection and joint onset. It is classified within the seronegative spondyloarthropathies (HLA-B27-associated).
The classic triad (formerly "Reiter's syndrome") is:
Arthritis + Urethritis/Cervicitis + Conjunctivitis
Modern usage broadens the definition to include mono- or oligoarthritis following GI or GU infection even without the complete triad.
Epidemiology
- Global prevalence: ~30 per 100,000 adults
- Predominantly affects young adults (20–40 years)
- More commonly diagnosed in men (genitourinary trigger) though GI-triggered cases affect men and women equally
- HLA-B27 is present in the majority; B27-positive individuals have a 20% risk of developing ReA after Salmonella or Yersinia epidemics (vs. 2–7% in B27-negative)
Triggering Pathogens
| Tract | Organisms |
|---|---|
| Gastrointestinal | Salmonella typhimurium, Yersinia enterocolitica, Shigella flexneri, Campylobacter jejuni, Clostridioides difficile |
| Genitourinary | Chlamydia trachomatis (most common overall trigger) |
| Other/emerging | C. pneumoniae, Giardia, HIV (alters course rather than triggers) |
Pathobiology
- Bacterial antigens have been identified in joints by immunofluorescence after both GI and GU infections
- PCR studies are most consistently positive in post-Chlamydia ReA, suggesting viable Chlamydia may persist in joint tissue in a metabolically altered state
- Toll-like receptor 2 (TLR-2) genetic variants implicate innate immune dysregulation in susceptibility
- Both T cell–mediated and antibody-mediated mechanisms are involved
- Dactylitis results from inflammation of the joint capsule, entheses, periarticular structures, and periosteal bone collectively
Clinical Features
Articular
- Asymmetric oligoarthritis of lower extremities (knee most common)
- Predilection for large joints; waxing/waning course
- Enthesitis: Achilles tendinitis, plantar fasciitis → heel pain and swelling
- Dactylitis: "sausage digit" — synovitis of a digital tendon sheath; may progress to calcaneal spurs and bony outgrowths
- Sacroiliitis: typically asymmetrical (distinguishes from ankylosing spondylitis, which is symmetrical)
- In chronic disease: bulky, non-marginal, asymmetrical syndesmophytes (vs. the thin marginal syndesmophytes of AS)
- Inflammatory low back pain is a common accompaniment
Extra-articular Features
| System | Manifestations |
|---|---|
| Urogenital | Urethritis (dysuria, discharge), circinate balanitis (vesicles/shallow ulcers on glans penis), cervicitis (often asymptomatic in women) |
| Ocular | Conjunctivitis (bilateral, painful); acute anterior uveitis (unilateral, less painful) |
| Skin | Keratoderma blennorrhagica — painless papulosquamous eruption on palms/soles; nail pitting, onycholysis, subungual keratosis |
| Mucous membranes | Painless oral/lingual ulcers |
| Cardiac | Aortic insufficiency (rare) |


Diagnosis
No single diagnostic test — diagnosis is clinical, supported by:
| Investigation | Finding |
|---|---|
| X-ray (peripheral joints) | Soft tissue swelling, juxta-articular osteopenia; periosteal new bone formation |
| X-ray (sacroiliac joints) | Asymmetrical sacroiliitis |
| X-ray (spine) | Bulky, non-marginal, asymmetrical syndesmophytes |
| Synovial fluid | Inflammatory (WBC 2,000–50,000); culture to exclude septic arthritis |
| HLA-B27 | Positive in majority; guides prognosis |
| Urethral/cervical swab / PCR | Identify Chlamydia |
| Stool culture/serology | For GI triggers |
Key differential: Septic arthritis — both Yersinia and Salmonella can cause true septic arthritis. Synovial fluid culture must be obtained before diagnosing reactive arthritis.
Treatment
Step 1 — Treat the Triggering Infection
- Post-Chlamydia ReA: 6-month course of combination antibiotic therapy:
- Rifampicin 300 mg/day + doxycycline 100 mg twice daily or azithromycin (500 mg twice daily × 5 days, then 500 mg/week)
- Response rate 65% (vs. ~20% with placebo); complete remission in 20% (vs. 0%)
- Appropriate antibiotic treatment for GI triggers if indicated
Step 2 — Anti-inflammatory Therapy
- NSAIDs — first-line for joint symptoms and enthesitis
- Glucocorticoid injections — effective for individual joint or enthesis involvement
- Sulfasalazine — recommended in more severe cases, especially if started within the first 3 months; more efficacious than methotrexate for this condition
Step 3 — Refractory / Chronic Disease
- Anti-TNF agents (infliximab, etanercept, adalimumab) — used in chronic HLA-B27-positive spondyloarthritis, though evidence specifically for ReA is limited
- Note: ~50% of patients recover within 6 months, so aggressive biologic use must be weighed carefully
Prognosis
- ~50% recover within 6 months
- ~50% have recurrent arthritis, tendinitis, or lumbosacral pain
- Risk of progression to chronic spondyloarthritis / ankylosing spondylitis exists (frequency not precisely defined)
- HLA-B27 positivity confers risk for axial involvement and chronicity
- HIV co-infection: more aggressive, refractory course
Sources: Goldman-Cecil Medicine, 26e (9780323930345); Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528)
ioc
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
What is the investigation of choice in reactive arthritis?
There is no single "investigation of choice" for reactive arthritis — the diagnosis is primarily clinical. However, here is how investigations are prioritized:
Investigation of Choice — Reactive Arthritis
1. Most Important Test: Synovial Fluid Analysis (Arthrocentesis)
- Purpose: To exclude septic arthritis — the most critical differential
- Findings in ReA: inflammatory fluid (WBC 2,000–50,000/μL, predominantly neutrophils), sterile on culture
- Both Yersinia and Salmonella can cause true septic arthritis, so synovial fluid must be cultured before diagnosing ReA
⚠️ Culture of synovial fluid must precede the diagnosis of reactive arthritis whenever possible (Goldman-Cecil Medicine).
2. HLA-B27 Testing
- Positive in the majority of patients
- Not diagnostic on its own, but:
- Guides prognosis (B27+ → higher risk of axial involvement, chronicity, sacroiliitis)
- B27+ individuals have up to 20% risk of ReA after epidemic GI infection (vs. 2–7% in B27−)
3. Identify the Triggering Infection
| Suspected trigger | Test |
|---|---|
| Chlamydia trachomatis | Urethral/cervical PCR (most sensitive; also detectable in synovial fluid/blood by PCR) |
| GI pathogens (Salmonella, Shigella, Yersinia, Campylobacter) | Stool culture + serology |
PCR for Chlamydia in synovial tissue is most consistently positive in post-Chlamydia ReA — suggesting viable organisms persist in the joint.
4. Radiology (Supportive, Not Diagnostic)
- X-ray of affected joints: juxta-articular osteopenia, periosteal new bone, enthesophytes
- X-ray of sacroiliac joints: asymmetric sacroiliitis (distinguishes from ankylosing spondylitis, which is symmetric)
- Not first-line for diagnosis but useful for staging and ruling out other causes
5. Non-Specific Inflammatory Markers
- ESR, CRP — elevated but non-specific
- CBC: leukocytosis
- Useful for monitoring disease activity, not diagnosis
Summary Table
| Investigation | Role |
|---|---|
| Synovial fluid culture | Exclude septic arthritis (most essential step) |
| HLA-B27 | Prognostication, supports diagnosis |
| Chlamydia PCR (urine/swab/synovial) | Identifies GU trigger |
| Stool culture/serology | Identifies GI trigger |
| X-ray | Assess joint/SI joint changes |
| ESR/CRP | Monitors inflammation |
Bottom line: ReA has no pathognomonic test. The diagnostic workup is directed at (1) excluding septic arthritis via synovial fluid, and (2) identifying the triggering organism via PCR or culture — with HLA-B27 adding prognostic value.
Source: Goldman-Cecil Medicine, 26e; Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.