I am postgraduate student in ent and. Want to deliver lecture on vertigo so I want you to give me detailed information on vertigo like physiology,pathology,clinical features and management of it
Reading File
Finding Sources
Finding Sources
Searching PubMed
vertigo vestibular disorders management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
vestibular system anatomy semicircular canals otolith organs
Loading Image
Loading Image
Searching the Web
vertigo ENT lecture comprehensive physiology pathology clinical management 2025
I now have comprehensive, authoritative content from Cummings Otolaryngology and K.J. Lee's Essential Otolaryngology. Let me compile the full lecture content:
VERTIGO — A Comprehensive Lecture for ENT Postgraduates
Sources: Cummings Otolaryngology Head & Neck Surgery; K.J. Lee's Essential Otolaryngology; Goldman-Cecil Medicine
1. DEFINITION & CLASSIFICATION
Vertigo is a sense of spontaneous movement — the illusion that either the patient or the environment is rotating, spinning, or tilting. It must be distinguished from other forms of dizziness:
| Type | Description |
|---|---|
| Vertigo | Illusion of rotational movement (true vestibular origin) |
| Presyncope | Near-fainting, lightheadedness from reduced cerebral perfusion |
| Disequilibrium | Imbalance/unsteadiness without head sensation |
| Non-specific dizziness | Ill-defined, vague floating sensation |
Peripheral vs. Central Vertigo
| Feature | Peripheral | Central |
|---|---|---|
| Severity | Severe, incapacitating | Milder, often chronic |
| Nystagmus | Horizontal-torsional, fixed direction | Variable, may be purely vertical |
| Fixation suppression | Present | Absent |
| Smooth pursuit | Normal | Saccadic (broken) |
| Saccades | Normal | Dysmetric |
| CNS symptoms | Absent | Often present |
| Caloric response | Unilateral canal paresis | Perverted or intact |
2. PHYSIOLOGY OF THE VESTIBULAR SYSTEM
The "Sixth Sense"
Balance is unique among the senses — it is automatic and subconscious until disrupted. The vestibular system serves two broad functions:
- Maintenance of balance (postural stability)
- Maintenance of stable gaze (via the vestibulo-ocular reflex, VOR)
Peripheral End Organs
The vestibular end organs comprise:
- Otolith organs (utricle and saccule) — detect linear acceleration and static head tilt relative to gravity
- Three semicircular canals (SCCs) — detect angular/rotational acceleration
- Lateral (horizontal) canal
- Superior (anterior) canal
- Posterior canal
The SCCs are paired structures:
- Left lateral ↔ Right lateral
- Left superior ↔ Right posterior
- Left posterior ↔ Right superior
The SCCs are oriented near-orthogonally to each other. Eye movements produced by VOR occur in the plane of the stimulated canal.
Hair Cell Transduction
Hair cells within the SCCs fire at a baseline (tonic) rate at rest. Head rotation causes endolymph — by inertia — to remain relatively stationary while the canal moves. This deflects the cupula, bending hair cell stereocilia:
- Toward the kinocilium (utricle direction in lateral canal = ampullopetal) → increased firing rate
- Away from kinocilium → decreased firing rate
This differential between the two paired canals is what the CNS reads as head movement.
The Vestibulo-Ocular Reflex (VOR)
The VOR maintains stable gaze by generating eye movements equal and opposite to head movements. Defects in VOR cause reduced dynamic visual acuity due to "retinal slip" (image not held on the fovea during head movement). This is the basis of the Head Impulse Test (HIT/HIT).
The Ewald Laws (Critical for Understanding Pathology)
- Ewald's 1st Law: Eye movements occur in the plane of the stimulated canal
- Ewald's 2nd Law (lateral canal): Ampullopetal (towards utricle) stimulation produces a greater response than ampullofugal
- Ewald's 3rd Law (vertical canals): Ampullofugal stimulation is excitatory
Asymmetry and Disease
When one vestibular labyrinth is suddenly destroyed, there is an abrupt asymmetry in firing rates. The intact side now fires at resting rate while the lesioned side fires at near-zero. The CNS interprets this imbalance as sustained rotation toward the healthy side — causing:
- Nystagmus (fast phase toward healthy ear, slow phase toward lesion)
- Nausea and vomiting
- Tendency to fall toward the lesion side
Over time, the CNS undergoes central compensation, gradually restoring equilibrium even without the damaged peripheral organ.
Otolith Organs
- Utricle: detects horizontal linear acceleration and head tilt
- Saccule: detects vertical linear acceleration
- Hair cells sit in the macula, covered by the otolithic membrane embedded with calcium carbonate crystals (otoconia/otoliths)
- Displacement of the otolith membrane relative to the macula stimulates hair cells

3. CLASSIFICATION OF VERTIGO (Etiological)
Peripheral Causes (labyrinth or vestibular nerve):
- BPPV (most common — ~48% of all cases)
- Ménière's disease (idiopathic endolymphatic hydrops)
- Vestibular neuritis
- Labyrinthitis
- Superior semicircular canal dehiscence (SSCD)
- Perilymphatic fistula
- Otosclerosis (cochlear type)
- Drug/ototoxicity (aminoglycosides, loop diuretics, quinine)
- Acoustic neuroma (vestibular schwannoma)
Central Causes (brainstem/cerebellum):
- Cerebellar/brainstem infarction or hemorrhage
- Multiple sclerosis
- Vertebrobasilar insufficiency
- Migraine-associated vertigo (vestibular migraine)
- Cerebellar tumors
Other/Systemic:
- Metabolic (hypothyroidism, diabetes, anemia)
- Cardiovascular (orthostatic hypotension, arrhythmias)
- Cervicogenic vertigo
- PPPD (persistent postural-perceptual dizziness)
- Psychogenic
4. DIFFERENTIAL DIAGNOSIS ALGORITHM
The key initial classification is episodic vs. constant:
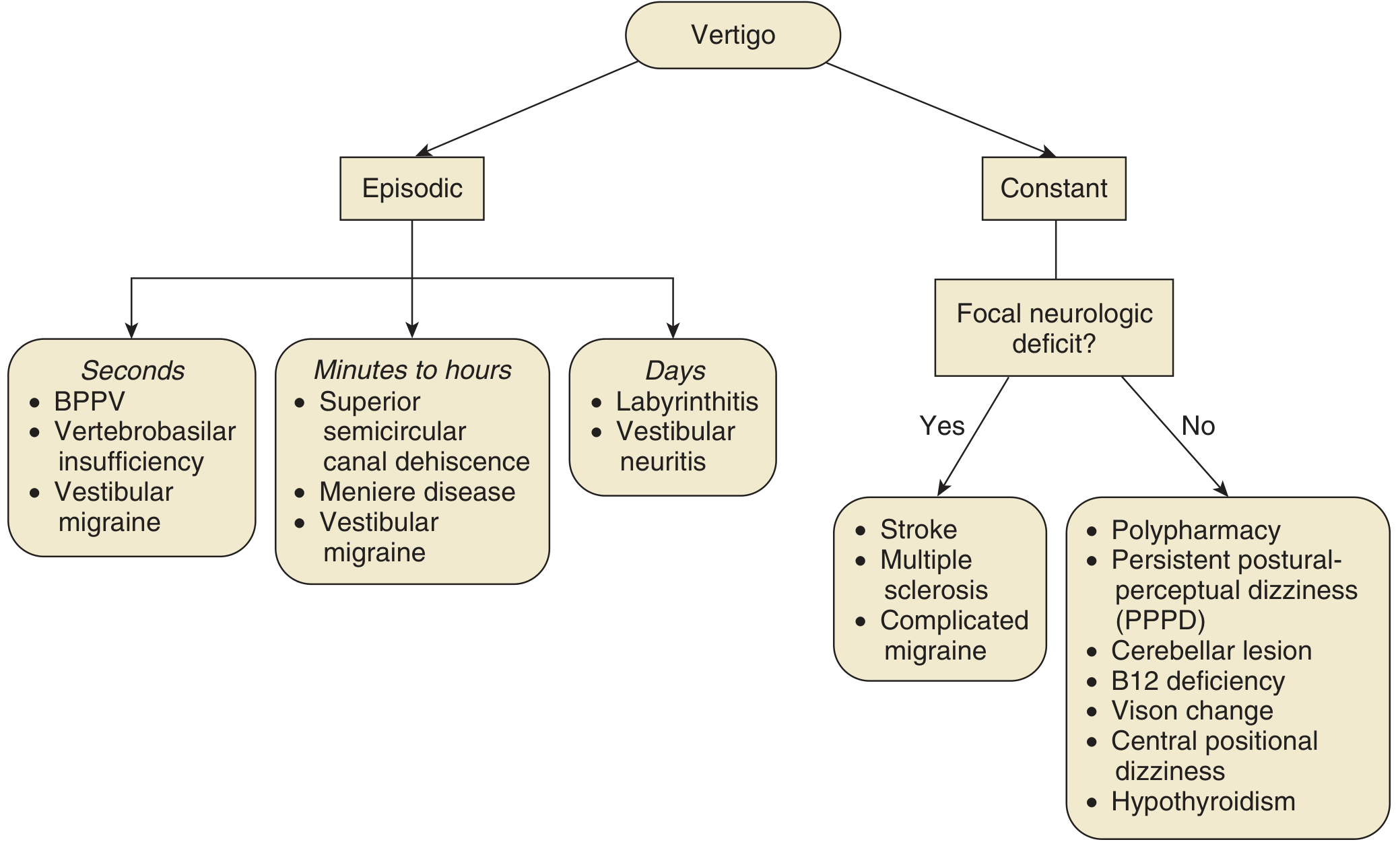
5. MAJOR CAUSES — PATHOLOGY, CLINICAL FEATURES & MANAGEMENT
5A. Benign Paroxysmal Positional Vertigo (BPPV)
The most common vestibular disorder (~48.5% of vertigo cases)
Pathophysiology
Two theories:
- Cupulolithiasis (original theory): Otoconia adhere to the cupula of the posterior SCC, making it gravity-sensitive — now largely replaced
- Canalolithiasis (current accepted theory): Otoconia detach from the utricular macula (due to degeneration or trauma) and float freely in the endolymph of the posterior SCC (most common), stimulating the cupula with head movement
The posterior SCC is most commonly involved because it is the most inferior SCC — the anatomic "sump" into which loose otoconia gravitate.
Canal involvement by frequency:
- Posterior SCC: ~85–90%
- Lateral (horizontal) SCC: ~10%
- Superior SCC: rare
Risk Factors
Head injury, prior vestibular neuritis, inner ear infections, ear surgery, osteoporosis, vitamin D deficiency
Clinical Features
- Sudden, severe vertigo triggered by specific head positions (lying down, rolling in bed, looking up, bending forward)
- Duration: seconds (< 1 minute per episode)
- No hearing loss, no tinnitus (differentiates from Ménière's)
- Nausea may accompany severe attacks
Nystagmus Characteristics (Dix-Hallpike test)
| Feature | BPPV (posterior canal) |
|---|---|
| Direction | Rotatory + upbeat (geotropic, toward the affected ear) |
| Latency | 2–10 seconds |
| Duration | < 60 seconds |
| Fatigability | Fatigues on repeated testing |
| Reversal | Reverses on returning to upright |
Horizontal (lateral) canal BPPV: Horizontal nystagmus in roll test — geotropic (toward ground) = canalolithiasis; apogeotropic (away from ground) = cupulolithiasis
Investigations
- Dix-Hallpike maneuver: Gold standard diagnostic test for posterior canal BPPV
- Supine Roll Test (Pagnini-McClure): For horizontal canal BPPV
- Audiogram: Normal (essential to exclude Ménière's)
Management
Conservative (first-line):
- Epley canalith repositioning procedure (CRP) — most effective; repositions otoconia back into the utricle; single treatment effective in ~80% of cases
- Semont liberatory maneuver — alternative, rapid, forceful positioning
- Brandt-Daroff exercises — habituation exercises for home use when CRP not feasible
Medical:
- Vestibular suppressants (meclizine, diazepam) — short-term symptom relief only; do NOT treat the underlying cause and may impede compensation
- Most cases resolve spontaneously within weeks to months
Surgical (rare, refractory cases):
- Posterior SCC occlusion (canal plugging)
- Singular neurectomy
5B. Ménière's Disease (Idiopathic Endolymphatic Hydrops)
Pathophysiology
Characterized by endolymphatic hydrops — distension of the endolymphatic compartment with increased pressure. The exact mechanism is debated but involves:
- Impaired endolymph reabsorption in the endolymphatic sac
- Possible immune-mediated mechanisms
- Rupture of Reissner's membrane → mixing of endolymph (high K⁺) and perilymph → potassium toxicity to hair cells → acute attack
Clinical Features — The Classic Tetrad (Lermoyez tetrad)
- Episodic vertigo — attacks lasting 30 minutes to 2 hours; severe with nausea/vomiting
- Fluctuating sensorineural hearing loss — characteristically low-frequency initially
- Tinnitus — typically low-pitched, "roaring" or "rushing water"
- Aural fullness/pressure — in the affected ear
Important: 85% unilateral at onset. Second ear involvement usually within 36 months. Natural remission in ~60% of patients.
Nystagmus in Ménière's Disease
- Irritative phase (early attack): nystagmus beats toward the affected ear
- Paralytic/deafferentative phase (later): nystagmus beats toward the healthy ear
- Recovery phase: reverses back toward the affected ear
Variants
- Cochlear hydrops: fluctuating SNHL + tinnitus, no vertigo
- Vestibular hydrops: episodic vertigo + aural fullness, no hearing loss
- Lermoyez syndrome: increasing tinnitus/hearing loss relieved by an attack of vertigo
- Crisis of Tumarkin (drop attack): sudden loss of extensor tone → fall, no loss of consciousness; occurs late in disease
Investigations
- Pure tone audiogram: Low-frequency SNHL, fluctuating; "rising" audiogram pattern
- Electrocochleography (ECoG): Increased SP/AP ratio (> 0.35) — reflects raised endolymphatic pressure
- Electronystagmography (ENG)/Videonystagmography (VNG): Unilateral canal paresis
- Glycerol test: Oral glycerol (1.2 mL/kg) reduces endolymph osmotically → transient improvement in hearing confirms endolymphatic hydrops
- MRI with gadolinium (3T): Gold standard for visualizing endolymphatic hydrops directly
Management
A. Conservative (Medical)
- Low-sodium diet (<1500–2000 mg/day) — reduces endolymph production
- Avoid caffeine, alcohol, smoking, MSG
- Diuretics (hydrochlorothiazide-triamterene, acetazolamide) — reduce endolymph volume
- Antivertiginous drugs (vestibular suppressants): meclizine, promethazine, diazepam — for acute attacks
- Vasodilators, calcium channel blockers
- Betahistine (widely used, especially in Europe)
B. Hearing-conservative, Non-ablative
- Intratympanic steroid injections (dexamethasone 4–24 mg/mL) — significant vertigo control in 80% of patients; avoids ablative surgery in ~80–91% of patients
- Endolymphatic sac decompression/shunt — controversial; debated efficacy
- Tenotomy of tensor tympani/stapedial tendons — controversial
C. Hearing-conservative, Vestibular Ablative
- Intratympanic gentamicin — selectively destroys vestibular hair cells; highly effective (preferred when hearing is still serviceable)
- Vestibular neurectomy (retrolabyrinthine, retrosigmoid, or middle cranial fossa approach)
D. Non-hearing-conservative, Vestibular Ablative
- Labyrinthectomy — when hearing is non-serviceable and vertigo is refractory
5C. Vestibular Neuritis
Second most common cause of peripheral vertigo after BPPV
Pathophysiology
- Selective inflammation and degeneration of the vestibular nerve, with sparing of the peripheral receptor structure
- Etiology: presumed viral (herpes simplex virus type 1) — reactivation in the vestibular ganglion (analogous to Bell's palsy from HSV-1 in the facial nerve)
- Superior vestibular nerve more commonly involved than inferior division — its bony canal is longer and narrower, making it more susceptible to compressive swelling
- No cochlear involvement (no hearing loss) — distinguishes it from labyrinthitis
Clinical Features
- Sudden onset, severe rotatory vertigo — worst at onset
- Nausea and vomiting (vegetative symptoms)
- Duration: intense vertigo for 1–3 days, gradual improvement over days to weeks; balance complaints may persist months
- No hearing loss, no tinnitus (critical distinguishing feature)
- May follow an upper respiratory infection ("epidemic vertigo")
- Can recur; bilateral disease described (must exclude bilateral vestibular loss)
- Subsequent BPPV in a small percentage of patients
Examination Findings
- Spontaneous horizontal-torsional nystagmus (fast phase away from lesioned side, toward intact ear)
- Head Impulse Test (HIT) positive on the affected side — corrective saccade seen
- Positive caloric unilateral canal paresis
- Normal hearing on audiogram
- Normal neurological examination (no focal deficits)
Investigations
- Videonystagmography (VNG): spontaneous nystagmus, unilateral canal paresis on calorics
- Video Head Impulse Test (vHIT): reduced VOR gain on affected side
- VEMP (vestibular evoked myogenic potentials): rarely useful since inferior vestibular nerve is rarely involved
- MRI with gadolinium: may show enhancement of the vestibular nerve; used to exclude retrocochlear lesion (acoustic neuroma)
Management
- Early ambulation — most important — promotes central compensation
- Vestibular suppressants (diazepam, meclizine) — short-term only (first 1–3 days); prolonged use impedes compensation
- Corticosteroids (methylprednisolone) — may improve caloric recovery if started early (within 3 days); current evidence is weak for symptomatic benefit
- Antivirals (valacyclovir) — not shown to have benefit in controlled trials
- Vestibular rehabilitation exercises — promotes and accelerates central compensation
5D. Labyrinthitis
- Inflammation affecting both the vestibular AND cochlear systems
- Presents with vertigo plus sensorineural hearing loss (distinguishes from vestibular neuritis)
- Causes: viral (most common), bacterial (usually from otitis media via round window membrane), syphilitic, autoimmune
- Bacterial labyrinthitis is the most severe form — can lead to meningitis; treat aggressively with antibiotics and steroids
- Management: underlying cause, vestibular suppressants acutely, hearing rehabilitation
5E. Superior Semicircular Canal Dehiscence (SSCD)
- Absence of bone overlying the superior SCC creates a third mobile window in the inner ear
- Classic presentation: Tullio phenomenon (vertigo/nystagmus induced by loud sound) and Hennebert sign (vertigo with pressure changes)
- Vertigo with Valsalva maneuver or nose-blowing
- Low-frequency conductive hearing loss with normal acoustic reflexes (mimics otosclerosis)
- Diagnosis: High-resolution CT temporal bone — confirms dehiscence; cVEMP shows reduced thresholds
- Management: Conservative (ear protection); surgical — canal plugging via middle cranial fossa or transmastoid approach
5F. Vestibular Migraine
- Most common central cause of episodic vertigo
- International criteria (ICHD-3): ≥5 episodes of moderate/severe vestibular symptoms (20 minutes to 72 hours) with current/past history of migraine with or without aura
- May occur without headache
- Episodic — seconds to hours duration; positional component possible
- Management: Acute — triptans, NSAIDs; Prophylaxis — propranolol, amitriptyline, topiramate, verapamil, valproate
6. CLINICAL EVALUATION
History — The 85% Rule
Patient history accounts for 85% of diagnostic information in the dizzy patient.
Key questions:
| Domain | Questions |
|---|---|
| Description | True spinning vs. lightheadedness vs. imbalance |
| Timing | Episodic vs. constant; duration (seconds/minutes/hours/days) |
| Triggers | Position change, head movement, noise/pressure, spontaneous |
| Associated symptoms | Hearing loss, tinnitus, aural fullness, headache, diplopia, dysarthria |
| Neurological | Focal weakness/numbness, diplopia, dysphagia |
| Medications | Aminoglycosides, furosemide, antiepileptics, antihypertensives |
Physical Examination
- Otoscopy — exclude acute otitis media, cholesteatoma, effusion
- Tuning fork tests (Weber, Rinne)
- Spontaneous nystagmus — direction, character, fixation suppression
- Dix-Hallpike maneuver — BPPV
- Supine Roll Test — horizontal canal BPPV
- Head Impulse Test (HIT/vHIT) — unilateral vestibular loss
- HINTS exam (Head Impulse, Nystagmus direction, Test of Skew) — to rule out stroke in acute vestibular syndrome
- Romberg test, Fukuda stepping test — falls toward lesion side in peripheral disease
- Cerebellar tests — finger-nose, heel-shin, dysdiadochokinesis
- Fistula test — tragal compression/pneumatic otoscopy for SSCD/perilymph fistula
HINTS Exam (for Acute Vestibular Syndrome)
| Test | Peripheral | Central (concerning) |
|---|---|---|
| Head Impulse | Abnormal (corrective saccade) | Normal |
| InNystagmus | Unidirectional | Direction-changing |
| Test of Skew | Absent | Skew deviation present |
A normal HIT + direction-changing nystagmus + skew deviation = central (stroke until proven otherwise). A positive HIT + unidirectional nystagmus + no skew = peripheral.
7. INVESTIGATIONS
Audiological Tests
| Test | Significance |
|---|---|
| Pure tone audiometry (PTA) | Flat/low-frequency SNHL in Ménière's; normal in BPPV/vestibular neuritis |
| Electrocochleography (ECoG) | SP/AP ratio >0.35 = endolymphatic hydrops |
| Auditory brainstem response (ABR) | Retrocochlear lesion (acoustic neuroma) |
Vestibular Function Tests
| Test | What It Measures |
|---|---|
| VNG/ENG with calorics | Canal function; unilateral canal paresis |
| Video Head Impulse Test (vHIT) | VOR gain per canal; identifies partial lesions |
| Rotary chair test | Bilateral vestibular loss |
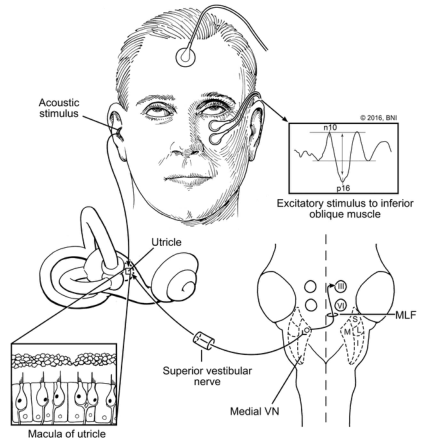
| cVEMP (cervical VEMP) | Saccule + inferior vestibular nerve |
| oVEMP (ocular VEMP) | Utricle + superior vestibular nerve; low thresholds in SSCD |
| Posturography (CDP) | Functional balance, sensory weighting |
| Glycerol test | Endolymphatic hydrops (Ménière's) |
Imaging
- MRI with gadolinium (3T): Acoustic neuroma, brainstem lesions, enhancement of vestibular nerve in neuritis; direct visualization of endolymphatic hydrops
- HRCT temporal bone: SSCD, otosclerosis, fractures, cholesteatoma
- MRI brain/posterior fossa DWI: Stroke/infarction in central vertigo
8. MANAGEMENT OVERVIEW
Acute Attack Management
- Bed rest in position of comfort (minimizes movement-triggered vertigo)
- Vestibular suppressants:
- Antihistamines: Meclizine 25–50 mg TDS; Promethazine (also antiemetic)
- Benzodiazepines: Diazepam 2–5 mg — most potent suppressant
- Phenothiazines: Prochlorperazine — good antiemetic
- Anticholinergics: Scopolamine patch — motion sickness
- Antiemetics: Metoclopramide, ondansetron
Caution: Vestibular suppressants should be used short-term only. Prolonged use delays central compensation and worsens long-term outcomes.
Vestibular Rehabilitation (VRT)
- The cornerstone of long-term recovery in most peripheral vestibular disorders
- Utilizes adaptation, habituation, and substitution exercises
- Promotes central compensation through plasticity of the cerebellar-vestibular pathways
- Particularly effective in vestibular neuritis, unilateral vestibular loss, PPPD
Surgical Options Summary
| Condition | Procedure | Ear-Preserving? |
|---|---|---|
| Ménière's (non-serviceable hearing) | Labyrinthectomy | No |
| Ménière's (serviceable hearing) | Vestibular neurectomy / IT gentamicin | Yes |
| Ménière's (all stages) | Endolymphatic sac decompression | Yes |
| BPPV (refractory) | Posterior canal occlusion | Yes |
| SSCD | Canal plugging (MCF or transmastoid) | Yes |
| Acoustic neuroma | Microsurgical removal | Depends on size |
9. PERIPHERAL vs. CENTRAL VERTIGO — SUMMARY TABLE
| Feature | Peripheral | Central |
|---|---|---|
| Onset | Sudden | Variable |
| Severity | Severe | Mild–moderate |
| Nystagmus direction | Horizontal-torsional, unidirectional | Any direction; may be vertical or direction-changing |
| Fixation | Suppresses nystagmus | No suppression |
| Hearing loss | May be present | Rare |
| Tinnitus | May be present | Rare |
| CNS signs | Absent | Present (dysarthria, diplopia, ataxia, weakness) |
| Head Impulse Test | Positive (abnormal VOR) | Negative (normal VOR) |
| Falls | Toward lesion | Variable/cerebellar |
| Nausea/vomiting | Prominent | Variable |
10. QUICK MNEMONIC AIDS
Ménière's tetrad — "FVTH": Fullness, Vertigo, Tinnitus, Hearing loss
BPPV treatment — "Epley moves the rocks" (canalith repositioning)
HINTS exam in AVS — "H-I-N-T-S": Horizontal HIT, Nystagmus type, Test of Skew
Peripheral nystagmus — "SLOW toward lesion, FAST toward sky" (Alexander's law: intensity increases with gaze toward fast phase)
Recent Evidence (PubMed 2024–2025)
- A 2025 systematic review [PMID 41166161] examined prophylactic management of vestibular migraine, now recognized as the most common central vestibular disorder requiring ENT referral.
- A 2025 meta-analysis [PMID 39693701] found a significant association between obstructive sleep apnea and vertigo — OSA screening is now advisable in recurrent vertigo patients.
LECTURE OUTLINE SUGGESTION
- Introduction — definition, epidemiology, burden
- Anatomy & Physiology of the vestibular system
- Differential diagnosis approach (episodic vs. constant; peripheral vs. central)
- BPPV — the commonest (pathophysiology + Epley demonstration)
- Ménière's Disease — the classic triad
- Vestibular Neuritis — diagnosis and HINTS exam
- Investigations — what, when, and why
- Management principles — acute, rehabilitative, surgical
- When to worry — red flags for central vertigo
- Case-based Q&A
— Cummings Otolaryngology Head and Neck Surgery | K.J. Lee's Essential Otolaryngology | Goldman-Cecil Medicine
I want you to give me more detailed and schematic approach of physiology and balance pathways
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
vestibular pathways nuclei VOR vestibulospinal reflex diagram
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive, deeply detailed content from Cummings, Kandel's Principles of Neural Science, and Ganong's Physiology. Let me now synthesize the full detailed schematic lecture:
PHYSIOLOGY OF BALANCE & VESTIBULAR PATHWAYS
A Detailed Schematic Account for ENT Postgraduates
Sources: Cummings Otolaryngology Head & Neck Surgery; Kandel's Principles of Neural Science (6th ed.); Ganong's Review of Medical Physiology (26th ed.); K.J. Lee's Essential Otolaryngology
MODULE 1: THE THREE PILLARS OF BALANCE
Balance is not a single-sense function. It depends on the integration of three sensory systems converging on the CNS:
┌─────────────────────────────────────────────────────────────┐
│ THE BALANCE TRIAD │
│ │
│ ┌──────────────┐ ┌──────────────┐ ┌──────────────┐ │
│ │ VESTIBULAR │ │ VISUAL │ │PROPRIOCEPTION│ │
│ │ SYSTEM │ │ SYSTEM │ │ (Somatosen) │ │
│ │ (dominant) │ │ (retina/OKN) │ │ (joints/feet)│ │
│ └──────┬───────┘ └──────┬───────┘ └──────┬───────┘ │
│ └──────────────────┼──────────────────┘ │
│ ↓ │
│ VESTIBULAR NUCLEI (pontomedullary) │
│ + CEREBELLUM (flocculonodular lobe) │
│ ↓ │
│ ┌──────────────────┼──────────────────┐ │
│ ↓ ↓ ↓ │
│ VOR (gaze) VSR (posture) Perception/ │
│ Eye movement Spinal cord Cortex │
└─────────────────────────────────────────────────────────────┘
When two of the three systems conflict or one fails, vertigo, dizziness, or imbalance results.
MODULE 2: PERIPHERAL VESTIBULAR END ORGANS
2A. Bony and Membranous Labyrinth
BONY LABYRINTH
│
├── Cochlea (hearing)
│
└── VESTIBULAR APPARATUS
│
├── 3 Semicircular Canals (SCCs)
│ ├── Lateral (Horizontal)
│ ├── Superior (Anterior)
│ └── Posterior
│
└── 2 Otolith Organs
├── Utricle
└── Saccule
Each SCC contains membranous semicircular duct filled with endolymph (high K⁺, low Na⁺), surrounded by perilymph (high Na⁺, low K⁺) in the bony labyrinth.
2B. The Semicircular Canals — Detecting Rotation
Structural Organization
SEMICIRCULAR CANAL (cross-section)
┌─────────────────────────────────────┐
│ Membranous duct │
│ │
│ ENDOLYMPH ─────────────────→ │
│ (K⁺-rich, 150 mEq/L K⁺) │
│ │
└──────────────────┬──────────────────┘
│
AMPULLA
│
┌───┴───┐
│ CRISTA │ ← Sensory receptor organ
│AMPULL.│
└───┬───┘
│
CUPULA
(gelatinous partition,
Sp. gravity = 1.0,
same as endolymph)
│
HAIR CELLS
Type I (calyceal afferents)
Type II (bouton afferents)
The Three Planes — Critical for Clinical Application
The three SCCs are oriented nearly orthogonally, each maximally sensitive to rotations in its own plane:
RIGHT LABYRINTH — CANAL PLANES:
SUPERIOR (ANTERIOR) CANAL
↗ plane ~45° to sagittal
LATERAL CANAL
→ horizontal plane
POSTERIOR CANAL
↘ plane ~45° to sagittal
Functional Canal Pairs (push-pull system):
| Canal (side A) | Paired with (side B) | Movement detected |
|---|---|---|
| Right Lateral | Left Lateral | Yaw (left-right turn) |
| Right Superior | Left Posterior | Pitch on right side / roll |
| Left Superior | Right Posterior | Pitch on left side / roll |
2C. Hair Cell Transduction — Molecular Mechanism
HAIR CELL BUNDLE ARCHITECTURE:
Kinocilium (tallest, 1 per cell)
│
─────┼─────────────────────────────
Stereocilia (graded height, ~80)
connected by TIP LINKS
│
─────┼─────────────────────────────
│
HAIR CELL BODY
│
Afferent nerve terminal (glutamate)
Efferent nerve terminal (ACh)
Transduction Mechanism:
HEAD ROTATION
│
▼
Endolymph lags (INERTIA)
│
▼
Cupula deflected
│
┌──┴──────────────────────────┐
│ │
↓ ↓
TOWARD kinocilium AWAY from kinocilium
(Ampullopetal in (Ampullofugal)
lateral canal)
↓ ↓
Tip links STRETCHED Tip links SLACKENED
↓ ↓
Mechanosensitive K⁺ K⁺ channels CLOSE
channels OPEN
↓ ↓
K⁺ influx from Hyperpolarization
endolymph (150 mEq/L)
↓
Depolarization
↓
Ca²⁺ influx at base
↓
Glutamate release
↓
INCREASED afferent DECREASED afferent
firing rate firing rate
(+above resting ~80 sp/s) (→ 0 sp/s minimum)
Ewald's 2nd & 3rd Laws explained by this mechanism:
- Lateral canal: Ampullopetal (towards utricle) = toward kinocilium = EXCITATION (stronger response)
- Vertical canals: Ampullofugal = toward kinocilium = EXCITATION
2D. Semicircular Canal Response to Rotation — Step by Step
PHASE 1: ACCELERATION (head starts turning right)
──────────────────────────────────────────────────
Head: → rotates right
Endolymph: lags behind (inertia) → relatively moves LEFT relative to canal
RIGHT lateral canal: endolymph → ampullopetal → cupula toward utricle
→ RIGHT canal INCREASES firing rate ↑
LEFT lateral canal: endolymph → ampullofugal → cupula away from utricle
→ LEFT canal DECREASES firing rate ↓
CNS reads: RIGHT > LEFT → perceives rightward rotation → CORRECT
PHASE 2: CONSTANT VELOCITY (steady rotation)
──────────────────────────────────────────────────
Endolymph reaches same speed as canal → no differential movement
Cupula returns to neutral position (time constant ~7 seconds)
Firing rates return to resting level
CNS reads: no rotation (perceptual adaptation — illusion of stopping)
PHASE 3: DECELERATION (rotation stops)
──────────────────────────────────────────────────
Canal stops but endolymph continues (momentum)
RIGHT canal: now ampullofugal → DECREASES below resting rate
LEFT canal: now ampullopetal → INCREASES above resting rate
CNS reads: LEFTWARD rotation (opposite direction!)
→ Post-rotational nystagmus / vertigo (beating to the left)
2E. The Otolith Organs — Detecting Linear Acceleration & Gravity
OTOLITH ORGAN STRUCTURE:
OTOLITHIC MEMBRANE (gelatinous layer)
│
OTOCONIA (CaCO₃ crystals, Sp. gravity 2.71–2.94)
│
──────────────────────── STRIOLA (dividing line)
│ │
TYPE I hair cells TYPE II hair cells
(irregular, fast) (regular, slow)
│
MACULA (sensory epithelium)
│
Hair cell cilia embedded in membrane
Orientation of Maculae:
UTRICLE (horizontal macula)
Plane: ~ horizontal
Function: detects HORIZONTAL linear acceleration
(e.g., car moving forward/backward)
+ STATIC HEAD TILT relative to gravity
SACCULE (vertical macula)
Plane: ~ vertical (sagittal)
Function: detects VERTICAL linear acceleration
(e.g., elevator going up/down)
Transduction by Otolith:
LINEAR ACCELERATION (e.g., head tilts left)
↓
Otoconia (dense, Sp. gravity 2.71) SLIDE relative to macula
↓
Hair cell cilia bent by otolithic membrane displacement
↓
Cells on side of kinocilium bending: EXCITED
Cells away from kinocilium: INHIBITED
↓
CNS decodes direction and magnitude of linear force vector
The "Striola" divides the macula into mirror-image halves with opposite polarizations, allowing detection of bidirectional linear accelerations.
MODULE 3: THE VESTIBULAR NERVE
HAIR CELLS (cristae + maculae)
│
Afferent fibers
Cell bodies in SCARPA'S GANGLION
│
VESTIBULAR NERVE (superior + inferior divisions)
│
Travels in INTERNAL AUDITORY CANAL (IAC)
alongside cochlear nerve (CN VIII)
│
Enters BRAINSTEM at cerebellopontine angle
│
▼
VESTIBULAR NUCLEI complex
Fiber Types in Vestibular Nerve:
| Type | Origin | Discharge | Function |
|---|---|---|---|
| Calyceal (irregular) | Striola (central crista) | Irregular, high sensitivity | Transient/dynamic signals |
| Bouton (regular) | Peripheral crista | Regular, low sensitivity | Sustained/tonic signals |
| Dimorphic | Both zones | Intermediate | Mixed |
Resting discharge rate: ~60–80 spikes/second in mammals. This tonic firing enables the push-pull system — one side can increase AND the other decrease around a stable baseline.
Efferent vestibular system: Medial olivocochlear neurons project back to hair cells via efferent vestibular fibers (ACh as neurotransmitter) — modulate sensitivity during voluntary movement (efference copy mechanism).
MODULE 4: THE VESTIBULAR NUCLEI — THE CENTRAL RELAY HUB
The vestibular nuclei (VN) sit at the pontomedullary junction in the floor of the 4th ventricle. There are 4 main nuclei and 6 minor cell groups:
VESTIBULAR NUCLEAR COMPLEX
(floor of 4th ventricle, pontomedullary junction)
┌─────────────────────────────────────────────┐
│ │
│ SUPERIOR VESTIBULAR NUCLEUS (of Bechterew) │
│ - SCC afferents (mainly) │
│ - Projects to: oculomotor nuclei, cereb. │
│ - Role: HORIZONTAL and VERTICAL VOR │
│ │
│ MEDIAL VESTIBULAR NUCLEUS (of Schwalbe) │
│ - SCC + some otolith input │
│ - Projects to: oculomotor nuclei │
│ - Gives rise to: MEDIAL VESTIBULOSPINAL TRACT│
│ (runs in Medial Longitudinal Fasciculus) │
│ - Role: VOR + vestibulocervical reflex │
│ │
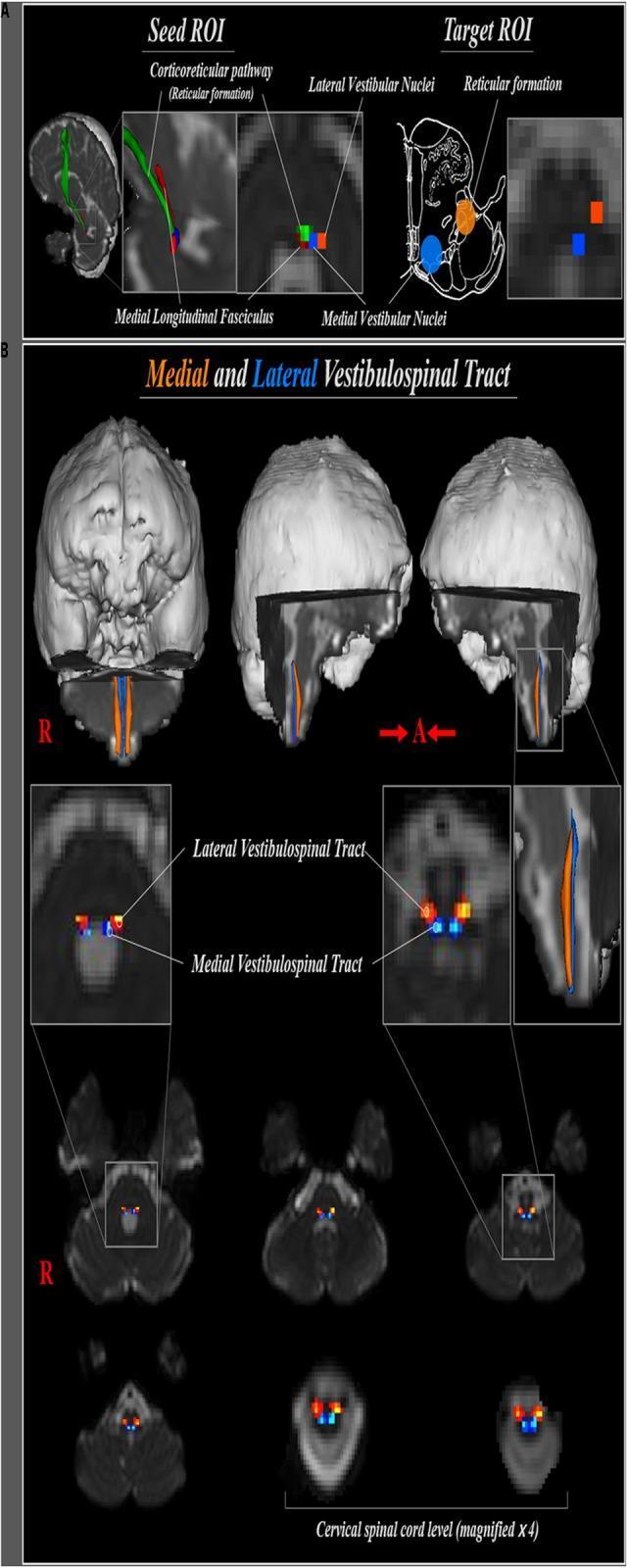
│ LATERAL VESTIBULAR NUCLEUS (Deiters' nucleus)│
│ - Otolith input (lateral), SCC (medial) │
│ - Contains giant DEITERS' CELLS │
│ - Gives rise to: LATERAL VESTIBULOSPINAL TRACT│
│ (somatotopically organized, full cord) │
│ - Role: POSTURAL reflexes (limb, axial) │
│ │
│ INFERIOR (DESCENDING) VESTIBULAR NUCLEUS │
│ - Mainly otolith input + some SCC │
│ - Projects to: cerebellum, reticular form. │
│ - Role: cerebellar feedback, autonomic │
└─────────────────────────────────────────────┘
Inputs to Vestibular Nuclei
INPUTS TO VESTIBULAR NUCLEI
┌─────────────────────────────────────────────────┐
│ Ipsilateral vestibular nerve (primary afferents)│
│ Contralateral VN (inhibitory commissural fibers)│
│ Cerebellum (flocculonodular lobe, fastigial n.) │
│ Visual cortex / optokinetic system │
│ Proprioceptive inputs (spinal cord) │
│ Reticular formation │
│ Premotor cortex │
│ Nucleus preposituse hypoglossi (NPH) │
└─────────────────────────────────────────────────┘
The Inhibitory Commissural System
RIGHT VN ────inhibitory (GABA)────→ LEFT VN
LEFT VN ────inhibitory (GABA)────→ RIGHT VN
Effect:
- When RIGHT ear excites RIGHT VN → simultaneously inhibits LEFT VN
(push-pull amplification)
- When RIGHT labyrinth is destroyed:
→ RIGHT VN silent
→ LEFT VN releases from inhibition → fires excessively
→ CNS reads: "leftward rotation"
→ NYSTAGMUS (fast phase to LEFT = toward intact side)
→ VERTIGO
→ FALLS toward lesion (rightward)
This commissural system explains why acute unilateral vestibular loss causes spontaneous nystagmus, and why central compensation (VN plasticity) eventually restores tone balance.
MODULE 5: THE FOUR MAJOR OUTPUT PATHWAYS FROM VESTIBULAR NUCLEI
╔═══════════════════════════════════════════════════════════════╗
║ VESTIBULAR NUCLEI — OUTPUT PATHWAYS ║
╠═══════════════════════════════════════════════════════════════╣
║ ║
║ 1. VESTIBULO-OCULAR REFLEX (VOR) PATHWAY ║
║ → Gaze stabilization ║
║ ║
║ 2. MEDIAL VESTIBULOSPINAL TRACT (MVST) ║
║ → Head/neck stabilization ║
║ ║
║ 3. LATERAL VESTIBULOSPINAL TRACT (LVST) ║
║ → Postural/limb stabilization ║
║ ║
║ 4. VESTIBULO-THALAMOCORTICAL PATHWAY ║
║ → Conscious perception of motion & space ║
╚═══════════════════════════════════════════════════════════════╝
PATHWAY 1: THE VESTIBULO-OCULAR REFLEX (VOR)
Function: Moves eyes EQUAL and OPPOSITE to head movement to stabilize gaze on the fovea.
HEAD TURNS RIGHT (angular velocity signal from RIGHT lateral SCC)
│
▼
RIGHT Lateral SCC excited → RIGHT Superior + Medial VN activated
│
▼
Signal crosses midline via MLF (Medial Longitudinal Fasciculus)
│
┌─────┴──────────────────────────────────────────┐
│ │
▼ ▼
LEFT ABDUCENS NUCLEUS (CN VI) RIGHT OCULOMOTOR NUCLEUS (CN III)
Activates LEFT lateral rectus Activates RIGHT medial rectus
(eye moves LEFT) (eye moves LEFT)
│ │
└─────────────────┬──────────────────────────────┘
▼
BOTH EYES MOVE LEFT
(compensatory, equal to head speed, opposite direction)
GAZE MAINTAINED ON TARGET ✓
VOR Arc Summary:
SCC → Scarpa's ganglion → Vestibular nerve → Vestibular nucleus → MLF →
→ Contralateral Abducens nucleus (CN VI) → Lateral rectus
→ Ipsilateral CN III (via MLF) → Medial rectus
VOR Gain: Normal = ~1.0 (eye velocity = head velocity)
- VOR gain < 1 = under-compensation → retinal slip (oscillopsia)
- Measured clinically by video Head Impulse Test (vHIT)
VOR Pathways for Vertical Eye Movements use the interstitial nucleus of Cajal (INC) and riMLF (rostral interstitial nucleus of MLF) as the vertical neural integrators.
PATHWAY 2: MEDIAL VESTIBULOSPINAL TRACT (MVST)
Origin: Medial + Inferior VN
Fiber type: Both ipsilateral and contralateral fibers
Runs in: Medial Longitudinal Fasciculus (MLF) — descends bilaterally
Terminates: Cervical and upper thoracic spinal cord (ventral horn interneurons → neck/upper limb muscles)
Fiber type: Both ipsilateral and contralateral fibers
Runs in: Medial Longitudinal Fasciculus (MLF) — descends bilaterally
Terminates: Cervical and upper thoracic spinal cord (ventral horn interneurons → neck/upper limb muscles)
MEDIAL VESTIBULAR NUCLEUS
│
▼
MEDIAL LONGITUDINAL FASCICULUS (MLF)
│
Descends bilaterally
│
▼
CERVICAL SPINAL CORD (C1–C4)
→ Neck extensors and flexors
→ Upper limb muscles
│
▼
VESTIBULOCERVICAL REFLEX (VCR):
Stabilizes HEAD position during body movement
(counter-rotation of head opposite to body tilt)
Clinical significance of MLF: Lesions of MLF → Internuclear Ophthalmoplegia (INO) — impaired adduction of ipsilateral eye with contralateral nystagmus. Seen in MS, brainstem stroke.
PATHWAY 3: LATERAL VESTIBULOSPINAL TRACT (LVST)
Origin: Lateral VN (Deiters' nucleus) — giant Deiters' cells
Organization: Somatotopic — most important for whole-body posture
Organization: Somatotopic — most important for whole-body posture
LATERAL VESTIBULAR NUCLEUS (Deiters')
│
├── Medium-sized neurons → Cervical spinal cord → UPPER LIMB
│
└── Large neurons → Lumbar spinal cord → LOWER LIMB
↓
Descends IPSILATERALLY in lateral funiculus of spinal cord
↓
Ventral horn → Alpha and gamma motoneurons
↓
EXCITES: Extensor muscles (anti-gravity, limb extensors, axial muscles)
INHIBITS: Flexor muscles (reciprocal inhibition via interneurons)
Function — Vestibulosplinal Reflex (VSR):
HEAD/BODY TILTS LEFT (otolith organs activated)
│
▼
LEFT Utricle stimulated more than right
│
▼
LEFT LVST → more excitatory drive to left limb EXTENSORS
RIGHT LVST → less drive to right limb extensors
│
▼
LEFT limbs extend (preventing fall)
RIGHT limbs flex
│
▼
BODY RETURNS TO UPRIGHT POSITION
This is why a patient with unilateral vestibular loss falls and deviates toward the lesion side — the intact side has unopposed extensor drive.
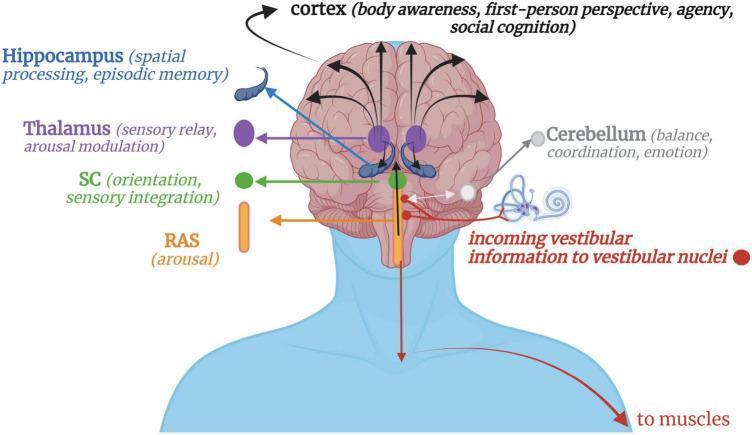
PATHWAY 4: VESTIBULO-THALAMOCORTICAL PATHWAY
Function: Conscious perception of movement, spatial orientation, vertigo
VESTIBULAR NUCLEI (Superior + Medial)
│
▼
THALAMUS
(Ventral posterior lateral nucleus — VPLc)
(Ventral posterolateral oral nucleus — VPLo)
│
▼
VESTIBULAR CORTEX
(No single dedicated area — distributed processing)
Key cortical areas:
├── PARIETO-INSULAR VESTIBULAR CORTEX (PIVC)
│ (Insula + parietal operculum — primary vestibular cortex)
│ Conscious tilt/rotation perception
│
├── AREA 2v (somatosensory cortex S1/S2)
│ Multisensory integration
│
├── HIPPOCAMPUS
│ Spatial navigation, cognitive map
│
└── PREFRONTAL CORTEX
Higher-order spatial cognition, agency
MODULE 6: THE CEREBELLUM IN VESTIBULAR CONTROL
The cerebellum is the master comparator and error corrector of the vestibular system.
CEREBELLAR REGIONS IN VESTIBULAR CONTROL:
┌──────────────────────────────────────────────────┐
│ FLOCCULONODULAR LOBE ("Vestibulocerebellum") │
│ • Flocculus + Nodulus │
│ • Receives: direct vestibular afferents │
│ • Receives: visual (optokinetic) input │
│ • Projects back to: Vestibular nuclei │
│ • Function: VOR adaptation, smooth pursuit, │
│ gaze holding, VOR suppression │
│ │
│ VERMIS (anterior + posterior) │
│ • Receives: spinal cord, VN input │
│ • Controls: axial/trunk postural muscles │
│ │
│ FASTIGIAL NUCLEUS (deep cerebellar) │
│ • Main output nucleus of vestibulocerebellum │
│ • Projects back to VN (inhibitory) │
│ • Also projects to brainstem reticular form. │
└──────────────────────────────────────────────────┘
Cerebellar feedback loop:
VESTIBULAR NUCLEI
│
├──→ FLOCCULUS (via mossy fibers + climbing fibers)
│ │
│ ←─────┘ (Purkinje cell inhibition — GABAergic)
│
└──→ NODULUS (via otolith signals)
│
←─────┘ (modulates tilt-rotation interaction)
VOR Adaptation (critical for rehabilitation):
The cerebellum (flocculus) compares expected vs. actual eye movement during head turns. When there is a mismatch (e.g., after unilateral labyrinthectomy), climbing fibers carry an error signal from the inferior olive → Purkinje cells → modify VOR gain over days/weeks. This is the neural basis of vestibular rehabilitation.
VOR Suppression:
When you track a moving target (e.g., watching a tennis ball), the VOR must be suppressed. This requires the flocculus to override the VOR arc. Failure of VOR suppression = cerebellar disease.
MODULE 7: THE OPTOKINETIC SYSTEM — VISUAL CONTRIBUTION TO BALANCE
MOVING VISUAL FIELD (e.g., train moving past you)
│
▼
Retinal image moves across fovea (optic flow)
│
▼
OPTIC TRACT → PRIMARY VISUAL CORTEX (V1)
│
▼
ACCESSORY OPTIC SYSTEM
(nucleus of optic tract, dorsal terminal nucleus)
│
▼
VESTIBULAR NUCLEI
(visual-vestibular convergence)
│
▼
OPTOKINETIC NYSTAGMUS (OKN):
Slow phase follows moving stripes
Fast phase resets back
│
COMPLEMENTARY to VOR at LOW frequencies
(VOR dominates at HIGH frequency/speed)
Clinical importance: OKN drum test; absent OKN in cortical/occipital lesions; perverted OKN in brainstem disease.
MODULE 8: SOMATOSENSORY / PROPRIOCEPTIVE INPUT
PERIPHERAL RECEPTORS:
├── Muscle spindles (Ia afferents) — joint position sense
├── Golgi tendon organs — muscle tension
├── Cutaneous mechanoreceptors (feet) — ground contact
└── Cervical proprioceptors — neck position (important for
cervicogenic vertigo)
│
▼
SPINAL CORD (dorsal columns + spinocerebellar tracts)
│
▼
VESTIBULAR NUCLEI (somatosensory input — especially from neck)
+ CEREBELLUM (spinocerebellar tracts → vermis + hemispheres)
│
▼
INTEGRATION with vestibular and visual signals
Sensory reweighting (Nashner's model):
NORMAL: Vision 20% + Vestibular 60% + Proprioception 20%
DARK: Vision 0% + Vestibular 70% + Proprioception 30%
ON FOAM: Vision 40% + Vestibular 50% + Proprioception 10%
When one input is unavailable, the CNS up-weights the others. When the vestibular system is damaged, patients become excessively vision-dependent and suffer when vision is disrupted (Romberg test on foam).
MODULE 9: NEURAL INTEGRATORS — CONVERTING VELOCITY TO POSITION
The VOR pathway encodes angular velocity of head movement. But the eyes need to know their static position to remain steady after a head movement. This requires mathematical integration (velocity → position signal):
SCC afferent: codes HEAD VELOCITY (ω)
│
▼
NEURAL INTEGRATOR
├── Nucleus Prepositus Hypoglossi (NPH) — horizontal
└── Interstitial Nucleus of Cajal (INC) — vertical
│
▼
Eye position signal → Motoneurons of CN III, IV, VI
│
▼
GAZE HOLDING (eyes stay put after head movement stops)
Leaky integrator = gaze-evoked nystagmus:
When the neural integrator is damaged (e.g., cerebellar disease, drugs like alcohol, benzodiazepines), the position signal "leaks" — eyes drift back to center → corrective saccade → gaze-evoked nystagmus (beats in direction of gaze). This is a central sign.
MODULE 10: VESTIBULAR COMPENSATION — THE RECOVERY PROCESS
After sudden unilateral vestibular loss (e.g., vestibular neuritis, labyrinthectomy):
ACUTE PHASE (hours 0–72):
───────────────────────────────────────────────────
Lesion: Right labyrinth destroyed
Right VN: silent (no input)
Left VN: loses inhibition from commissural right VN
→ fires excessively
CNS interprets: leftward head rotation (that isn't happening)
Result: Spontaneous nystagmus (fast phase LEFT)
Vertigo (sense of spinning left)
Nausea, vomiting
Falls to RIGHT (toward lesion)
SUBACUTE PHASE (days 3–14): STATIC COMPENSATION
───────────────────────────────────────────────────
Mechanisms:
1. Right VN increases spontaneous activity (plastic upregulation)
2. Removal of inhibitory inputs → VN sensitivity changes
3. Cerebellum adjusts the gain of VN commissural inhibition
4. Re-weighting of visual/proprioceptive inputs
Result: Spontaneous nystagmus decreases and disappears at rest
CHRONIC PHASE (weeks to months): DYNAMIC COMPENSATION
───────────────────────────────────────────────────
VOR adaptation by FLOCCULUS (error-signal driven)
Movement-induced symptoms diminish with repeated exposure
Vestibular rehabilitation accelerates this phase
Key neurotransmitters in compensation:
├── GABA (commissural inhibition modulation)
├── Glutamate (excitatory plasticity)
├── Acetylcholine (efferent modulation)
└── BDNF/NGF (neurotrophin-mediated synaptic remodeling)
MODULE 11: FULL PATHWAY SCHEMA — ONE-PAGE OVERVIEW
┌─────────────────────────────────────────────────────────────────────┐
│ VESTIBULAR SYSTEM — COMPLETE PATHWAY │
│ │
│ PERIPHERAL RECEPTOR │
│ ┌──────────────────────────────────────────────┐ │
│ │ SCCs (rotation) → CRISTA → HAIR CELLS │ │
│ │ Otoliths (linear) → MACULA → HAIR CELLS │ │
│ └──────────────────┬───────────────────────────┘ │
│ │ Glutamate │
│ ▼ │
│ VESTIBULAR NERVE (CN VIII) │
│ Scarpa's Ganglion → Superior + Inferior divisions │
│ │ │
│ ┌──────────▼─────────┐ │
│ │ VESTIBULAR NUCLEI │ ◄── Cerebellum feedback │
│ │ (4 main + minor) │ ◄── Contralateral VN (GABA) │
│ │ Pontomedullary │ ◄── Visual/OKN input │
│ └──────────┬─────────┘ ◄── Proprioception (spinal) │
│ │ │
│ ┌──────────────┼──────────────────────────┐ │
│ │ │ │ │ │
│ ▼ ▼ ▼ ▼ │
│ VOR pathway MVST (MLF) LVST Thalamocortical │
│ CN III/IV/VI Cervical cord Full cord (VPL thalamus) │
│ Gaze stable Head/neck Posture/ Conscious perception │
│ stabilization limb control Spatial orientation │
│ │ │ │ │
│ ▼ ▼ ▼ │
│ EYE MUSCLES NECK MUSCLES LIMB/AXIAL CORTEX (PIVC, insula, │
│ (gaze fixed) (head stable) MUSCLES hippocampus) │
│ (posture) │
│ │
│ CEREBELLUM │
│ ┌─────────────────────┐ │
│ │ Flocculonodular lobe│ │
│ │ ← VN + visual input │ │
│ │ → VN (inhibitory) │ │
│ │ VOR adaptation │ │
│ │ VOR suppression │ │
│ └─────────────────────┘ │
└─────────────────────────────────────────────────────────────────────┘
MODULE 12: NEUROTRANSMITTERS OF THE VESTIBULAR SYSTEM
| Location | Neurotransmitter | Effect |
|---|---|---|
| Hair cell → afferent nerve | Glutamate | Excitatory |
| Efferent vestibular (lateral olivocochlear) | Acetylcholine | Inhibitory (modulates sensitivity) |
| VN → oculomotor nuclei (excitatory) | Glutamate | Excitatory VOR |
| Commissural VN → contralateral VN | GABA | Inhibitory (push-pull) |
| Purkinje cells (cerebellum → VN) | GABA | Inhibitory (cerebellar braking) |
| VN inhibitory interneurons | Glycine | Inhibitory |
Pharmacological Consequences:
- Benzodiazepines (enhance GABA): suppress VN firing → reduce vertigo acutely; but also impair compensation
- Betahistine (histamine H1/H3 agonist/antagonist): increases blood flow to labyrinth; may reduce VN excitability via H3 presynaptic receptors
- Aminoglycosides: toxic to type I hair cells preferentially (striolar region) → bilateral vestibular loss
MODULE 13: PHYSIOLOGICAL BASIS OF KEY CLINICAL SIGNS
| Clinical Sign | Physiological Basis |
|---|---|
| Spontaneous nystagmus | VN asymmetry → tonic drive to VOR pathway → slow eye drift toward lesion + fast corrective saccade |
| Head Impulse Test positive | Reduced VOR gain on affected side; high-speed impulse reveals inadequate compensation → corrective catch-up saccade |
| Alexander's Law | Nystagmus increases with gaze toward fast phase — due to leaky neural integrator effect |
| Romberg sign | Loss of vestibular input → falls when visual compensation removed (eyes closed) |
| Fukuda stepping test | LVST asymmetry → deviation/rotation toward lesion side |
| Dix-Hallpike nystagmus | Loose otoconia in posterior SCC → gravity-driven movement of debris → cupular deflection → posterior SCC firing |
| Post-rotational nystagmus | Deceleration creates opposite cupular deflection to acceleration; normal response |
| Caloric nystagmus | Cold water cools lateral SCC endolymph → decreased convection → mimics ipsilateral head turn → nystagmus away from tested ear (COWS: Cold Opposite Warm Same) |
| VOR suppression failure | Cerebellar (flocculus) lesion → cannot suppress VOR when tracking moving target |
SUMMARY SCHEMA — 10-SECOND RECALL
HEAR → FEEL HEAD MOVE → SEMICIRCULAR CANALS / OTOLITHS
↓
VESTIBULAR NERVE (CN VIII)
↓
VESTIBULAR NUCLEI (4)
┌──────────────┤├──────────────┐
↓ ↓ ↓
VOR (eyes) VSR (posture) CORTEX (perception)
↑
CEREBELLUM (adapts/suppresses VOR)
Sources: Cummings Otolaryngology Head & Neck Surgery (Ch. 129) | K.J. Lee's Essential Otolaryngology (Ch. 16) | Kandel's Principles of Neural Science, 6th Ed. (Ch. 27) | Ganong's Review of Medical Physiology, 26th Ed. (Ch. 11)
This is a shared conversation. Sign in to Orris to start your own chat.