Epilepsy
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"epilepsy"[MeSH Terms] AND "anticonvulsants"[MeSH Terms]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Epilepsy - Management & Treatment Guidelines (Exam Notes)
1. When to Start Antiseizure Drug (ASD) Therapy
| Situation | Action |
|---|---|
| Single unprovoked seizure, normal exam/EEG/imaging | Defer treatment - discharge from ED, outpatient follow-up |
| Single seizure + risk factors (prior brain injury, EEG epileptiform activity, structural MRI lesion, nocturnal seizure) | Treat |
| Recurrent unprovoked seizures | Always treat |
| Seizure from reversible cause (electrolyte, drug-induced) | Correct the cause; ASDs usually unnecessary |
| Structural lesion (tumor, abscess, AVM) | Treat underlying cause; maintain ASD for 6-12 months post-surgery |
Risk of recurrence after first unprovoked seizure: 31-71% in first 12 months.
2. General Principles of ASD Selection
- Monotherapy first - controls seizures with minimum toxicity in most patients
- Choice depends on: seizure type > expected side effects > drug interactions > comorbidities > cost > dosing frequency
- Target: complete seizure freedom with no side effects
- ~30% of focal epilepsy patients are refractory to medical treatment
3. Drug Selection by Seizure Type
| Seizure Type | First-Line ASDs | Drugs to AVOID |
|---|---|---|
| Focal (partial) seizures | Carbamazepine, Oxcarbazepine, Lamotrigine, Levetiracetam, Valproate, Phenytoin | - |
| Generalized tonic-clonic (GTC) | Valproate, Lamotrigine, Levetiracetam, Topiramate | - |
| Absence seizures | Ethosuximide (first-line), Valproate, Lamotrigine | CBZ, PHT, Vigabatrin, Tiagabine (can worsen!) |
| Myoclonic seizures | Valproate, Levetiracetam, Clonazepam | CBZ, PHT, Gabapentin (can worsen!) |
| Atonic seizures / Lennox-Gastaut | Valproate + Lamotrigine + Benzodiazepine; Topiramate, Felbamate, Clobazam, Rufinamide | - |
| Juvenile Myoclonic Epilepsy (JME) | Valproate (drug of choice), Lamotrigine, Levetiracetam | CBZ (can worsen myoclonus) |
Exam trap: CBZ/PHT given for IGE (absence, myoclonic) can worsen seizures.
4. Key Antiseizure Drugs - Quick Reference
| Drug | Mechanism | Key Notes |
|---|---|---|
| Phenytoin | Na+ channel blocker | Dose-dependent kinetics (zero-order at therapeutic doses); IV: precipitates in dextrose, use NS only; causes gingival hyperplasia, hirsutism, folate deficiency, teratogen |
| Carbamazepine | Na+ channel blocker | Induces own metabolism (autoinduction); drug interactions; aplastic anemia (rare); hyponatremia; teratogen |
| Valproate | Na+ channel + GABA enhancement + T-Ca2+ | Broadest spectrum; weight gain, tremor, hepatotoxicity, pancreatitis; highest teratogen risk (neural tube defects); monitoring: LFTs, CBC |
| Lamotrigine | Na+ channel blocker | Slow titration to avoid Stevens-Johnson syndrome; safe in pregnancy (relatively); interaction with VPA (increases levels 2x) |
| Levetiracetam | SV2A protein (vesicle release) | Broad spectrum; minimal drug interactions; behavioral side effects (irritability, depression) |
| Ethosuximide | T-type Ca2+ channel blocker | Only effective for absence seizures |
| Phenobarbital | GABA-A enhancer | IV highly effective but causes severe sedation, respiratory depression, hypotension |
| Topiramate | Na+ channel + GABA + AMPA/kainate blocker | Cognitive side effects ("dopamax"), kidney stones, metabolic acidosis, angle-closure glaucoma |
| Oxcarbazepine | Na+ channel blocker | Fewer drug interactions than CBZ; hyponatremia more common |
| Gabapentin/Pregabalin | α2δ subunit Ca2+ channels | Mainly focal seizures; no serious drug interactions |
| Lacosamide | Slow Na+ inactivation | IV form available for SE; monitor ECG (PR prolongation) |
5. Therapeutic Drug Monitoring (TDM)
TDM ranges should be interpreted flexibly - some patients maintain remission at "subtherapeutic" levels. Indications for checking levels:
- Change in formulation
- Breakthrough seizures
- Adding/removing interacting drug
- Pregnancy
- Assessment of adherence
| Drug | Therapeutic Range |
|---|---|
| Carbamazepine | 4-12 mcg/mL |
| Phenytoin | 10-20 mcg/mL (total) |
| Valproate | 50-100 mcg/mL |
| Ethosuximide | 40-100 mcg/mL |
| Phenobarbital | 15-40 mcg/mL |
| Lamotrigine | 3-13 mcg/mL |
| Levetiracetam | 12-46 mcg/mL |
(Source: Katzung's Basic & Clinical Pharmacology, 16th ed.)
6. Refractory Epilepsy
- Defined as failure of 2 adequate trials of appropriate ASDs
- Affects ~30% of focal epilepsy patients
- Options:
- Combination pharmacotherapy - combine first-line drugs (CBZ, OXC, LTG, VPA, LEV, PHT)
- Surgery - resection of epileptogenic focus (requires presurgical evaluation: video-EEG, high-res MRI, neuropsychology, PET/SPECT)
- Vagus nerve stimulation (VNS)
- Dietary therapy (ketogenic diet - especially in children)
- Responsive neurostimulation (RNS)
For drug-refractory focal epilepsy: surgical resection offers excellent chance of seizure-free outcome. Presurgical workup includes EEG, MRI, PET, SPECT (SISCOM - subtraction ictal SPECT coregistered to MRI).
7. Status Epilepticus (SE) Management
Definition: Seizure lasting ≥5 min OR ≥2 seizures without recovery between them
Step-by-Step Protocol (Adams & Victor; Katzung)
STEP 1 - Stabilize (0-5 min)
- Ensure airway, ventilation, BP; intubate if needed
- IV access; send glucose, electrolytes, toxic screen
- Administer glucose + thiamine (if alcoholism/malnutrition suspected)
- Check for cranial/cervical injury if onset unwitnessed
STEP 2 - Benzodiazepines (First-line)
- IV Lorazepam 0.1 mg/kg (preferred for sustained effect) OR
- IV Diazepam 0.15-0.2 mg/kg
- Prehospital: rectal diazepam, intranasal midazolam, or buccal midazolam
- Lorazepam vs. Diazepam: lorazepam has longer duration (less peripheral redistribution); recent data do not clearly favor one over the other
STEP 3 - Second-line ASDs (after BZD failure)
- IV Levetiracetam, Valproate, Fosphenytoin, or Phenytoin (all equally effective for BZD-refractory SE)
- Seizure cessation in ~50% of patients with any of these agents
- Phenytoin: 15-20 mg/kg IV at 25-50 mg/min in normal saline (precipitates in dextrose!); monitor BP and ECG
- Fosphenytoin: 50-75 mg/min; can be given faster, IM possible
- IV Lacosamide: also used but monitor ECG (arrhythmia risk)
STEP 4 - Refractory SE (seizures continue ≥30 min after steps 1-3)
- Anesthetic doses:
- Midazolam 0.2 mg/kg load then 0.1-0.4 mg/kg/h infusion
- Propofol 2 mg/kg/h (caution: propofol infusion syndrome >48h)
- Pentobarbital 10 mg/kg/h
- Inhalational anesthetics (isoflurane)
- Add phenobarbital 10 mg/min to total 20 mg/kg IV, or carbamazepine/levetiracetam via NG
- Neuromuscular paralysis + continuous EEG monitoring if convulsions persist
STEP 5 - Super-refractory SE (SE recurs ≥24h after anesthesia)
- No established therapy - reinstate general anesthesia
Special SE Situations
| Type | Treatment |
|---|---|
| Absence SE | BZD → IV Valproate; then oral ethosuximide or VPA long-term |
| Focal non-convulsive SE | IV ASDs; avoid general anesthesia |
| Non-convulsive SE in coma | Often refractory; may need general anesthesia |
8. Epilepsy in Special Populations
Pregnancy
- Valproate has highest teratogenicity - avoid if possible (neural tube defects, cognitive effects in offspring)
- Lamotrigine and levetiracetam are relatively preferred in pregnancy
- AAN/AES 2024 guideline: All ASDs carry some teratogenic risk; decision involves risk-benefit for mother and fetus
- Women with seizure disorders who are seizure-free before conception may be candidates for non-pharmacologic observation
Elderly
- Reduced hepatic metabolism and renal clearance - lower starting doses
- Avoid drugs with complex pharmacokinetics (PHT)
Children
- Infantile spasms (West syndrome): ACTH or vigabatrin
- Childhood absence epilepsy: ethosuximide or valproate
- Juvenile myoclonic epilepsy: valproate (lifelong in most)
- Benign rolandic epilepsy: often spontaneously remits; treatment if frequent
9. Non-Pharmacologic Management
| Option | Indication |
|---|---|
| Surgery (temporal lobectomy, lesionectomy) | Drug-refractory focal epilepsy |
| Ketogenic diet | Drug-refractory epilepsy, especially children; glucose transporter deficiency |
| Vagus nerve stimulation (VNS) | Drug-refractory epilepsy, not surgical candidates |
| Responsive neurostimulation (RNS) | Drug-refractory focal epilepsy |
| Deep brain stimulation (DBS) | Refractory generalized epilepsy |
10. Precipitating Factors / Lifestyle Advice
- Sleep deprivation - universal precipitant; optimize sleep
- Alcohol intake - lower seizure threshold
- Reflex epilepsy triggers (video games, music, startle)
- Stress reduction (exercise, meditation, counseling)
- Driving - prohibited until cleared by neurologist (per state/local law)
- Avoid swimming alone, working at heights, operating hazardous machinery
High-Yield Exam Points (Summary)
- Lorazepam > diazepam for IV SE (longer central nervous system effect due to less peripheral redistribution)
- Phenytoin IV must be in normal saline (precipitates in dextrose); max rate 50 mg/min (risk: hypotension, heart block)
- Ethosuximide is only effective for absence - not GTC or focal
- Valproate = broadest spectrum but highest teratogenicity
- CBZ/PHT/Vigabatrin/Tiagabine can worsen absence and myoclonic seizures
- Refractory SE = failure of BZD + 2nd-line agent → anesthesia (pentobarbital, propofol, midazolam)
- Levetiracetam, Valproate, Fosphenytoin, Phenytoin are equally effective as 2nd-line IV agents in SE
- Before epilepsy surgery: must do presurgical evaluation (video-EEG, MRI, neuropsychology, ± PET/SPECT)
- Single unprovoked seizure + normal exam/EEG/imaging = do not treat, defer to outpatient
- JME = valproate DOC; lifelong therapy usually required; CBZ worsens it
Sources: Harrison's Principles of Internal Medicine 22E (2025); Adams & Victor's Principles of Neurology 12th Ed; Katzung's Basic & Clinical Pharmacology 16th Ed; Tintinalli's Emergency Medicine; Bradley & Daroff's Neurology in Clinical Practice
Advites
Ascites
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I have everything needed. Here are the comprehensive exam-focused notes on Ascites:
Ascites - Exam-Focused Notes
1. Definition & Causes
Ascites = abnormal accumulation of fluid in the peritoneal cavity.
Causes by frequency:
- Cirrhosis - 84% of all cases (most common)
- Cardiac ascites / heart failure - ~5%
- Peritoneal carcinomatosis - ~10%
- "Mixed" ascites (cirrhosis + 2nd disease)
- Less common: TB peritonitis, pancreatitis, nephrotic syndrome, Budd-Chiari syndrome, massive hepatic metastases, hypothyroidism, Chlamydia infection
First and cheapest confirmation test = abdominal ultrasound (detects as little as 100 mL)
2. Pathophysiology
In Cirrhosis (Portal Hypertension)
- Hepatic fibrosis → disrupts sinusoidal architecture → increased hepatic resistance to portal flow
- Decreased hepatic eNOS → reduced NO → intrahepatic vasoconstriction
- Paradoxically: splanchnic vasodilation (systemic NO, VEGF, TNF) → pooling of blood → reduced effective circulating volume
- Kidneys perceive "hypovolemia" → activate RAAS + SNS + ADH → Na and water retention → ascites
In Absence of Cirrhosis
- Peritoneal carcinomatosis / TB - protein-rich fluid from inflamed peritoneum + lymphatic obstruction
- Pancreatic ascites - leakage of pancreatic enzymes into peritoneum
- Nephrotic syndrome / hypoalbuminemia - reduced oncotic pressure
3. Diagnostic Paracentesis
Mandatory in all patients with new-onset ascites - safe even with coagulopathy. Left lower quadrant preferred (thinner wall, more fluid depth). Use ultrasound guidance if percussion cannot locate fluid.
Fluid to Send:
| Test | Indication |
|---|---|
| Albumin (+ simultaneous serum albumin) | Always - to calculate SAAG |
| Total protein | Always |
| PMN/Cell count + differential | Always - screens for SBP |
| Bacterial cultures (into blood culture bottles at bedside) | Always |
| Cytology | If malignancy suspected |
| Glucose + LDH | If secondary peritonitis suspected |
| Amylase | If pancreatic ascites suspected |
| AFB smear + culture, ADA | If TB suspected |
Gross Appearance Clues:
| Appearance | Cause |
|---|---|
| Turbid / cloudy | Infection or tumor cells |
| White/milky (chylous) | Triglycerides >200 mg/dL; lymphatic disruption (trauma, cirrhosis, tumor, TB) |
| Dark brown | High bilirubin - biliary tract perforation |
| Black | Pancreatic necrosis or metastatic melanoma |
| Bloody | Malignancy, trauma, or TB |
4. SAAG - The Key Diagnostic Tool
SAAG = Serum albumin - Ascitic fluid albumin (specimens drawn same day)
Accuracy ~97% for diagnosing portal hypertension. SAAG reflects hepatic sinusoidal pressure and correlates well with HVPG (r = 0.72).
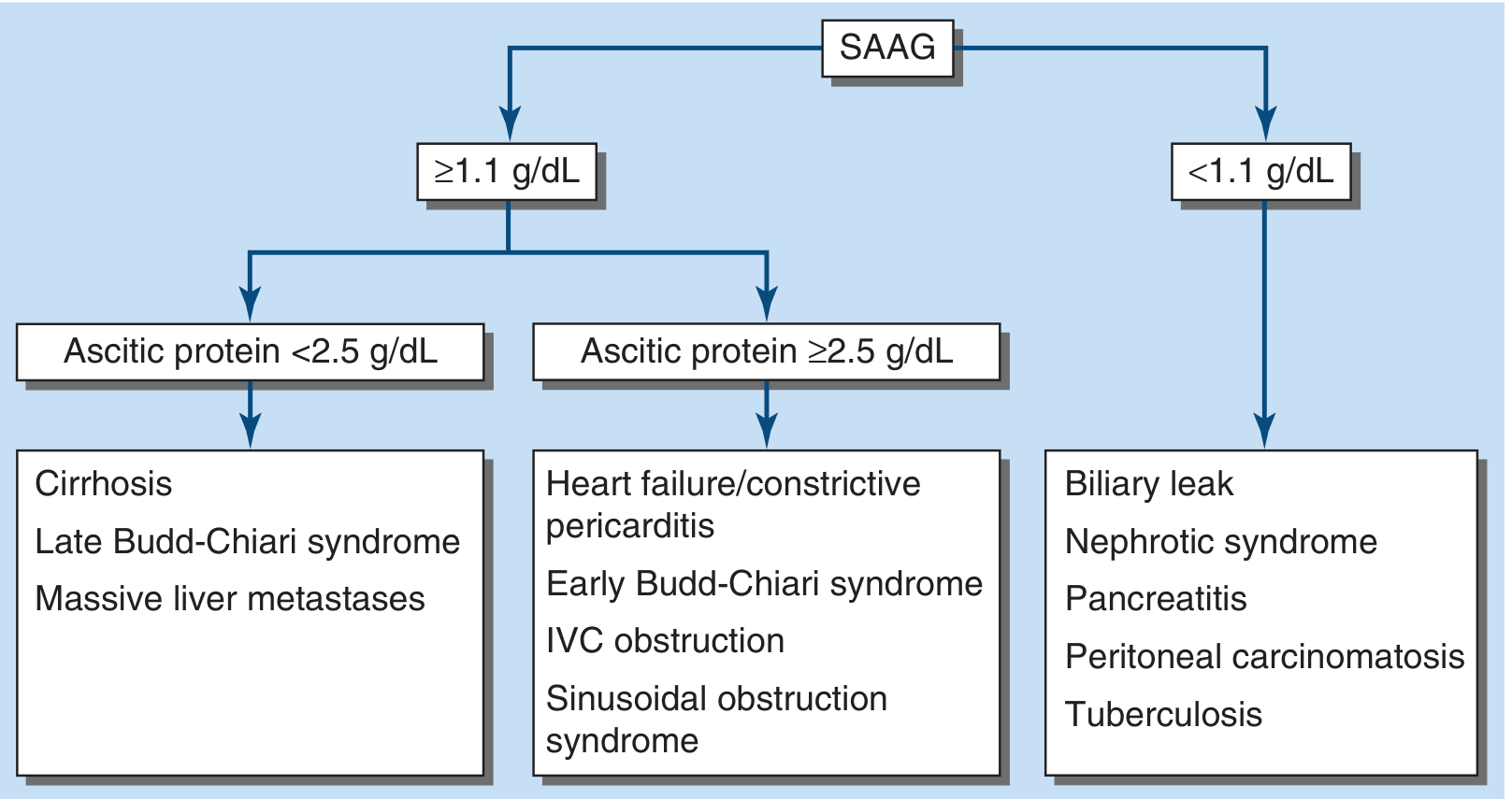
Interpreting SAAG + Ascitic Protein Together:
| Condition | SAAG | Ascitic Protein | Mechanism |
|---|---|---|---|
| Cirrhosis | ≥1.1 (HIGH) | <2.5 (LOW) | Capillarized sinusoids don't leak protein |
| Heart failure / constrictive pericarditis | ≥1.1 (HIGH) | ≥2.5 (HIGH) | Normal (leaky) sinusoids, congested |
| Early Budd-Chiari / IVC obstruction | ≥1.1 (HIGH) | ≥2.5 (HIGH) | Sinusoidal obstruction |
| Late Budd-Chiari / Massive metastases | ≥1.1 (HIGH) | <2.5 (LOW) | Fibrosed sinusoids |
| Peritoneal carcinomatosis / TB | <1.1 (LOW) | ≥2.5 (HIGH) | Peritoneal exudate |
| Nephrotic syndrome / Pancreatitis | <1.1 (LOW) | Variable | No portal hypertension |
Exam trick: BNP elevated in serum → points to cardiac ascites (high-SAAG + high protein).
False SAAG results: Chylous ascites (falsely HIGH); serum hyperglobulinemia >5 g/dL (narrows gradient - use correction: SAAG × [0.16 × (serum globulin + 2.5)])
5. Management of Cirrhotic Ascites
Step 1 - Mild/Moderate Ascites: Dietary + Diuretics
Sodium restriction: 2 g/day (88 mmol/day). More restrictive diets compromise nutrition.
Diuretics (spironolactone + furosemide - classic combination):
| Drug | Starting Dose | Max Dose | Mechanism |
|---|---|---|---|
| Spironolactone | 100 mg/day (morning) | 400 mg/day | Aldosterone antagonist - more effective than loop diuretics alone |
| Furosemide | 40 mg/day | 160 mg/day | Loop diuretic - add if insufficient response or hyperkalemia |
- Ratio maintained at furosemide:spironolactone = 40:100 (e.g., 80 mg:200 mg)
- Adjust every 3-4 days
- Goal: Weight loss 1 kg first week, then 2 kg/week subsequently
- Stop or reduce if: Weight loss >0.5 kg/day (no edema) or >1 kg/day (with peripheral edema) - risk of hypovolemia
Diuretic side effects: Hypovolemic hyponatremia, hyperkalemia, renal dysfunction, encephalopathy, gynecomastia (spironolactone) - substitute amiloride (5-40 mg/day) if gynecomastia distressing.
AVOID in cirrhotic ascites: NSAIDs, ACE inhibitors, ARBs (worsen renal perfusion). Beta blockers should be used cautiously in refractory ascites (associated with decreased survival).
Step 2 - Refractory Ascites (10-20% of patients)
Definition: Ascites persisting despite Na restriction + maximum diuresis, OR inability to tolerate maximum diuresis due to side effects.
Options:
| Option | Notes |
|---|---|
| Large-Volume Paracentesis (LVP) (>5 L) + albumin 6-8 g/L removed | Albumin prevents "post-paracentesis circulatory dysfunction" and reduces mortality. Required when >5 L removed. |
| TIPS (transjugular intrahepatic portosystemic shunt) | More effective than LVP at preventing recurrence; higher risk of hepatic encephalopathy; no overall mortality difference. PTFE-covered TIPS improves survival in patients needing >2 LVPs/month |
| Midodrine (α1-agonist) ± Clonidine | Counteract splanchnic vasodilation; improve diuretic response |
| Peritoneovenous shunt | For patients unsuitable for TIPS or transplant |
| Alfapump (automated pump to bladder) | Reduces LVP frequency; high technical failure and renal dysfunction risk |
| Long-term albumin (40 g twice weekly × 2 weeks, then 40 g weekly) | Added to spironolactone + furosemide; reduces recurrence and improves 18-month survival |
| Liver transplantation | Definitive treatment |
Albumin alone acutely (without diuretics) is of no benefit and may increase risk of pulmonary edema.
6. Spontaneous Bacterial Peritonitis (SBP)
Definition: Infection of ascitic fluid without a surgically correctable source.
Pathogens: Gram-negative rods (E. coli, Klebsiella) most common; also streptococci and enterococci. Multidrug-resistant organisms increasing.
Clinical features: Abdominal pain/tenderness (only 40% have tenderness!), fever, nausea/vomiting, unexplained hepatic encephalopathy or renal dysfunction. Often asymptomatic - diagnostic paracentesis should be done on all cirrhotic patients admitted to hospital.
Diagnosis:
- Ascitic PMN count ≥250/µL = diagnostic of SBP
- Cultures positive in only 40-50% of cases (inoculate blood culture bottles at bedside)
- PMN count >250 + multiple organisms → suspect secondary bacterial peritonitis (perforated viscus)
Treatment:
- IV Cefotaxime 2 g every 8-12 hours for 5 days (third-generation cephalosporin)
- IV Albumin 1.5 g/kg on day 1 AND 1 g/kg on day 3 → prevents hepatorenal syndrome, reduces mortality
- Repeat paracentesis at 48 hours - confirm PMN count decreased ≥25%
- Nosocomial SBP or critically ill → consider carbapenem (MDR organisms)
SBP Prophylaxis:
- Oral norfloxacin or ciprofloxacin (daily) for: prior SBP history, ascitic protein <1 g/dL, active GI bleeding
- IV ceftriaxone for inpatients
7. Hepatorenal Syndrome (HRS)
Definition: Functional kidney injury in severe portal hypertension/end-stage liver disease - diagnosis of exclusion.
Mechanism: Extreme splanchnic vasodilation → renal vasoconstriction → renal failure without structural kidney damage.
Types:
| Type | Characteristics |
|---|---|
| HRS-AKI (type 1) | Rapid progressive (creatinine doubles to >2.5 mg/dL in <2 weeks), often precipitated by SBP, GI bleed, LVP without albumin |
| HRS-CKD (type 2) | Slower, more stable, associated with refractory ascites |
Diagnosis - only after excluding:
- Sepsis/vasodilators (worsen vasodilation)
- GI hemorrhage, overdiuresis, diarrhea (decrease circulating volume)
- NSAIDs (renal vasoconstriction)
- Aminoglycosides (nephrotoxic)
- Volume expansion with albumin (1 g/kg/day × 2 days) must fail to improve creatinine
Treatment:
- Vasoconstrictors: Terlipressin (preferred) or norepinephrine + IV albumin
- Liver transplantation = definitive (HRS is a transplant priority)
8. Hepatic Hydrothorax
- Transudation of ascites through diaphragmatic defects into pleural space (usually right-sided, ~85%)
- Manage similarly to ascites: Na restriction + diuretics
- Thoracentesis for diagnostic/symptomatic relief; repeated drainage discouraged
- TIPS if refractory
9. Other Complications
Hyponatremia (serum Na <130 mEq/L)
- Fluid restriction to 1.5 L/day
- Tolvaptan (V2-receptor antagonist) can raise Na but not approved long-term (hepatotoxicity); use only as bridge to transplant
Hepatic Encephalopathy (HE)
- Graded I-IV; overt HE diagnosed clinically + asterixis
- Ammonia levels unreliable for grading (high >150 µmol/L supportive but non-specific)
- EEG: generalized slowing + triphasic waves
- Minimal/subclinical HE in up to 80% of cirrhotics
Hepatopulmonary Syndrome (HPS)
- Criteria: PaO2 <80 mmHg OR A-a gradient >15 mmHg + pulmonary vascular shunting on contrast echo
10. Ascitic Fluid Analysis Summary Table
| Parameter | Cirrhosis | Cardiac | Peritoneal Cancer | TB | Pancreatic |
|---|---|---|---|---|---|
| SAAG | ≥1.1 | ≥1.1 | <1.1 | <1.1 | <1.1 |
| Total protein | <2.5 | ≥2.5 | ≥2.5 | ≥2.5 | High |
| PMN count | Low | Low | Variable | Elevated | Variable |
| Special tests | - | BNP elevated | Cytology | ADA >30-45 U/L, AFB | Amylase very high |
High-Yield Exam Points
- Cirrhosis = 84% of all ascites; paracentesis is mandatory for new-onset ascites even in coagulopathy
- SAAG ≥1.1 = portal hypertension (97% accurate); does NOT change with diuresis
- Cirrhosis = high SAAG + LOW protein (capillarized sinusoids don't leak protein)
- Cardiac ascites = high SAAG + HIGH protein - the key differentiator from cirrhosis
- SBP = ascitic PMN ≥250/µL; treat with IV cefotaxime + IV albumin (albumin prevents HRS)
- LVP >5 L must be accompanied by albumin 6-8 g per liter removed (prevents circulatory dysfunction)
- Spironolactone:Furosemide ratio = 100:40 (5:2); max 400:160 mg/day
- TIPS = better than LVP at preventing ascites recurrence; more hepatic encephalopathy
- Beta blockers should be used cautiously in refractory ascites (may reduce survival)
- Terlipressin + albumin = treatment of HRS; liver transplant = definitive
- Avoid NSAIDs, ACE inhibitors, ARBs in cirrhotic ascites (worsen renal perfusion)
- Chylous ascites = milky appearance, TG >200 mg/dL; causes: lymphatic trauma, cirrhosis, tumor, TB
Sources: Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine International Edition; Yamada's Textbook of Gastroenterology 7th Ed; Sleisenger & Fordtran's GI and Liver Disease; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.