Haemorrhagic shock in details
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching PubMed
"hemorrhagic shock" AND resuscitation
Loading Image
Loading Image
I now have all the material needed for a comprehensive, detailed answer. Let me compile it.
Haemorrhagic Shock - A Detailed Overview
Definition
Haemorrhagic shock is a state of circulatory failure resulting from a rapid reduction in intravascular blood volume due to acute blood loss. It produces an imbalance between systemic oxygen delivery and oxygen consumption, leading to cellular hypoxia, metabolic derangement, and - if untreated - death. It is the most common form of hypovolaemic shock and a component of virtually all other shock states.
- Bailey and Love's Short Practice of Surgery, 28th ed
- ROSEN's Emergency Medicine
Aetiology / Causes
Blood loss leading to haemorrhagic shock may be:
External haemorrhage:
- Trauma (lacerations, fractures)
- Gastrointestinal bleed (haematemesis, melaena, PR bleeding)
- Obstetric haemorrhage (postpartum, placenta praevia)
Internal haemorrhage:
-
Haemothorax, haemoperitoneum, retroperitoneal haematoma
-
Ruptured ectopic pregnancy, ruptured aortic aneurysm
-
Pelvic fractures (>2000 mL blood loss), femur fractures (800-1000 mL)
-
Schwartz's Principles of Surgery, 11th ed
Pathophysiology
Macrocirculatory Response
Haemorrhage reduces venous return, preload, and cardiac output. Initially, an increase in heart rate and cardiac contractility is triggered. Baroreceptors in the aortic arch and carotid sinus detect the fall in arterial pressure and activate sympathetic outflow, causing:
- Peripheral vasoconstriction (to preserve perfusion to heart, brain, kidneys)
- Tachycardia
- Release of catecholamines (epinephrine, norepinephrine)
- Activation of the renin-angiotensin-aldosterone axis (renin, angiotensin II, aldosterone)
- ADH/vasopressin release (water retention + vasoconstriction)
- Cortisol, growth hormone, and glucagon release
The initial response is a narrowing of pulse pressure (vasoconstriction raises diastolic pressure) before systolic pressure falls. Hypotension is therefore a late sign of significant haemorrhage.
- ROSEN's Emergency Medicine
Microcirculatory Response
Even before cardiac output falls, blood is diverted away from non-critical tissues. Ischemic cells:
- Take up interstitial fluid (further depleting intravascular volume)
- Produce lactate and free radicals
- Cause cellular oedema, which can restrict adjacent capillary flow - the "no-reflow" phenomenon - preventing reversal of ischaemia even with restored macroperfusion
The cells also release inflammatory mediators: prostacyclin, thromboxane, prostaglandins, leukotrienes, endothelin, complement, interleukins, and TNF. Damage-associated molecular patterns (DAMPs), mitochondrial DNA, and formyl peptides amplify the systemic inflammatory response.
- Miller's Anesthesia, 10th ed
The Shock Cascade
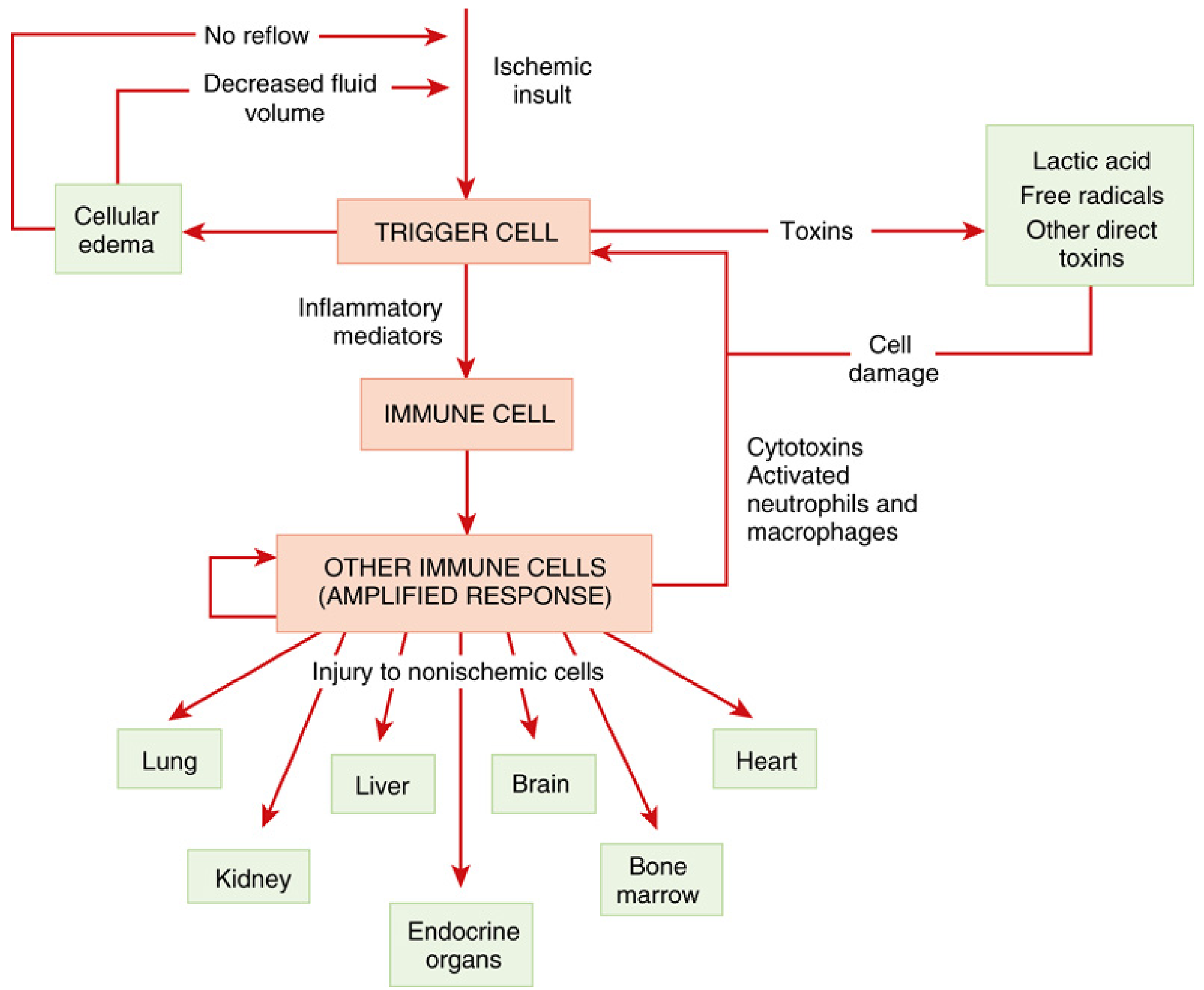
The "Shock Cascade" (Miller's Anesthesia, 10th ed): Ischemia triggers cellular and immune responses that injure remote, non-ischemic organs - the basis of MODS.
This inflammatory response becomes a self-sustaining disease process independent of its origin, laying the foundation for multiple organ dysfunction syndrome (MODS).
Base Deficit as an Early Marker
Lactic acid accumulates even before cardiac output falls significantly. Bicarbonate in plasma buffers pH, so pH may remain near normal while base deficit worsens. A base deficit more negative than -2 mEq/L is an early marker distinguishing trivial from clinically significant haemorrhage. A base deficit >8 mmol/L implies ongoing cellular shock.
- ROSEN's Emergency Medicine; Schwartz's Principles of Surgery
Progressive vs. Nonprogressive Shock
A key physiological concept (Guyton & Hall):
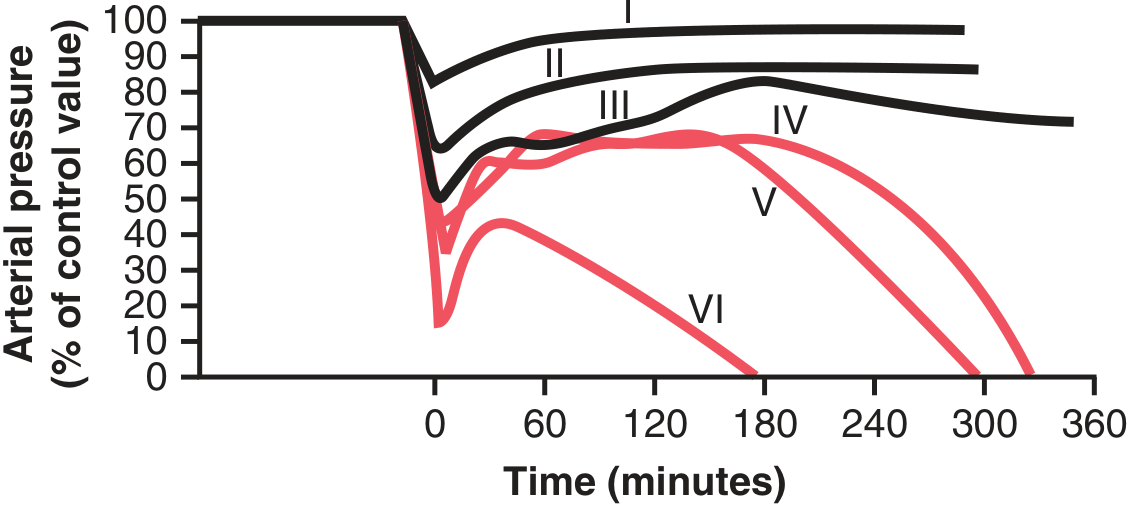
Fig. 24.2 (Guyton & Hall): Groups I-III (black lines, BP never below ~45 mmHg) - compensated/nonprogressive shock with recovery. Groups IV-VI (red lines) - progressive shock leading to death despite initial partial recovery.
Beyond a critical threshold of blood loss, shock becomes self-perpetuating - "the shock itself causes more shock." This is a vicious cycle driven by:
- Baroreceptor reflexes (powerful sympathetic stimulation)
- CNS ischaemic response (activated when MAP <50 mmHg)
- Reverse stress-relaxation of blood vessels
- RAAS activation
- ADH secretion
- Adrenal medullary epinephrine/norepinephrine release
- Fluid absorption from intestinal tract and capillaries
- Guyton and Hall Textbook of Medical Physiology
Organ-Specific Effects
| Organ | Response |
|---|---|
| CNS | Prime neuroendocrine trigger; cortical activity depressed with hypoperfusion (reversible initially, then permanent); failure to recover neurological function = poor prognosis |
| Kidney | Selective medullary vasoconstriction; inability to concentrate urine (renal hibernation); tubular necrosis with prolonged hypotension; adrenal insufficiency in ~86% of acute haemorrhagic shock cases (high mortality association) |
| Heart | Protected until late stages; maintained or increased nutrient blood flow; cardiac dysfunction occurs terminally due to lactate, free radicals, and humoral negative inotropes; elderly cannot mount tachycardic response - rapidly progressive |
| Lung | Acts as a filter for inflammatory by-products; neutrophil/platelet aggregation in capillaries; increased permeability → ARDS (sentinel organ for MODS) |
| Gut | Earliest organ of hypoperfusion; intense vasoconstriction; "no-reflow" on macro-restoration; barrier breakdown → bacterial translocation → potentiates ARDS |
| Liver | Complex microcirculation; reperfusion injury; synthetic failure |
- Miller's Anesthesia, 10th ed
Classification (ATLS / PHTLS Staging)
The Advanced Trauma Life Support classification divides haemorrhagic shock into 4 classes:
| Parameter | Class I | Class II | Class III | Class IV |
|---|---|---|---|---|
| Blood loss (mL) | Up to 750 | 750-1500 | 1500-2000 | >2000 |
| Blood loss (% BV) | Up to 15% | 15-30% | 30-40% | >40% |
| Pulse rate | <100 | >100 | >120 | >140 |
| Blood pressure | Normal | Normal | Decreased | Decreased |
| Pulse pressure | Normal/increased | Decreased | Decreased | Decreased |
| Respiratory rate | 14-20 | 20-30 | 30-40 | >35 |
| Urine output (mL/h) | >30 | 20-30 | 5-15 | Negligible |
| Mental status | Slightly anxious | Mildly anxious | Anxious/confused | Confused/lethargic |
Important caveat: HR and BP are notoriously unreliable as sole indicators of haemorrhagic shock severity. Tachycardia may be blunted by beta-blockers, cardiac disease, or high fitness level. Pregnant patients must lose a larger relative blood volume before manifesting hypovolaemia. Elderly patients may not mount tachycardia.
- Schwartz's Principles of Surgery, 11th ed; ROSEN's Emergency Medicine
Clinical Features and Diagnosis
History: Mechanism of injury, estimated visible blood loss, prior medications (anticoagulants, beta-blockers), last known vital signs
Physical exam signs:
- Pallor, cold clammy skin, diaphoresis
- Tachycardia (may be absent in elderly, beta-blocked patients)
- Hypotension (late sign)
- Narrowed pulse pressure
- Decreased urine output
- Altered mental status (confusion, agitation, obtundation)
- Prolonged capillary refill time
Initial response to fluid:
- Responders - normalise and stay stable; unlikely ongoing haemorrhage
- Transient responders - improve then deteriorate; suggest ongoing bleeding
- Non-responders - persistent hypotension despite resuscitation; mandate immediate source identification and intervention
Investigations:
- Haemoglobin/haematocrit (may be normal acutely due to haemoconcentration)
- Base deficit (most sensitive early marker)
- Serum lactate
- Arterial blood gas
- Coagulation screen (PT/INR, aPTT, fibrinogen)
- Viscoelastic testing: TEG (thromboelastography) or ROTEM (rotational thromboelastometry) for dynamic clotting assessment
- FAST ultrasound (haemoperitoneum, haemopericardium, haemothorax)
- Chest and pelvic X-rays
- CT (only in stable or rapidly stabilising patients - hazardous to transport hypotensive patient for CT)
The Lethal Triad
A critical concept in haemorrhagic shock management:
Hypothermia + Acidosis + Coagulopathy
These three conditions are mutually reinforcing and progressively worsen outcomes:
- Hypothermia impairs clotting factor function and platelet aggregation
- Acidosis (partly iatrogenic from crystalloid resuscitation - normal saline pH 5.0, Lactated Ringer's pH 6.5) worsens coagulopathy
- Coagulopathy leads to ongoing haemorrhage, further worsening hypothermia and acidosis
The lethal triad is often precipitated or worsened by inappropriate crystalloid resuscitation.
- Fischer's Mastery of Surgery, 8th ed; Sabiston Textbook of Surgery
Acute Coagulopathy of Trauma (ACT)
ACT occurs early in haemorrhagic shock, before significant haemodilution from resuscitation fluids. Its mechanisms involve:
- Tissue trauma activating the coagulation and fibrinolytic cascades
- Consumption of clotting factors
- Protein C activation (anticoagulant effect)
- Endotheliopathy of trauma
Clinically, ACT is distinct from dilutional coagulopathy (which results from excessive crystalloid resuscitation). Both, however, contribute to ongoing haemorrhage if not recognised and treated.
Management
Prehospital
- Direct pressure / tourniquet for compressible external haemorrhage
- Pelvic binder for pelvic fractures
- Splinting of long bone fractures
- Large-bore IV access and commence blood products if available (prehospital blood transfusion reduces mortality in selected cases)
Emergency Department - Primary Survey (ATLS: ABCDE)
- Airway with C-spine control
- Breathing - address tension pneumothorax, haemothorax (needle decompression / chest drain)
- Circulation - haemorrhage control, IV access, blood products
- Disability - GCS
- Exposure - full exposure, keep warm
Haemorrhage Control
- Direct pressure, wound packing, tourniquet
- Pelvic external fixation or binder
- Resuscitative thoracotomy (in extremis penetrating trauma: cardiac arrest or imminent)
- REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta) - for non-compressible torso haemorrhage as a bridge to definitive surgery; a 2026 systematic review compared REBOA vs resuscitative thoracotomy for this indication
Permissive Hypotension (Hypotensive Resuscitation)
Target systolic BP 80-90 mmHg (MAP ~60 mmHg) until definitive haemorrhage control is achieved. Rationale: aggressive normotension can "pop off" a sealing clot, worsen haemorrhage, dilute clotting factors, and cause hypothermia.
Important contraindications to permissive hypotension:
-
Traumatic brain injury (TBI): maintain SBP >110 mmHg per Brain Trauma Foundation; if combined haemorrhagic shock + severe TBI: MAP >80 mmHg
-
Blunt trauma (most cases)
-
Elderly patients with comorbidities (cardiac disease, carotid stenosis)
-
Penetrating trauma in urban settings is the primary evidence base
-
Mulholland & Greenfield's Surgery, 7th ed; Tintinalli's Emergency Medicine
Damage Control Resuscitation (DCR)
The modern paradigm for massive haemorrhage:
1. Avoid crystalloids
- Crystalloids worsen dilutional coagulopathy, acidosis, and hypothermia
- Use only as a temporary bridge when blood products are unavailable
2. Blood product resuscitation in 1:1:1 ratio
- pRBCs : Fresh Frozen Plasma : Platelets = 1:1:1
- Rationale: reconstitutes whole blood; the PROPPR trial showed early survival benefit (28-day mortality difference was not statistically significant)
- Type O-negative pRBCs for women of childbearing age; pre-thawed AB plasma can be used immediately
3. Whole blood
- Recent evidence suggests whole blood may be superior to component therapy when available
4. Tranexamic acid (TXA)
- Anti-fibrinolytic agent
- Given as early as possible after injury (ideally within 3 hours; benefit is lost after 3 hours)
- Standard dose: 1 g IV over 10 min, then 1 g IV over 8 hours
5. Massive transfusion protocol (MTP)
- Predefined protocol for patients needing >10 units pRBCs in 24 hours (up to 5% of civilian trauma)
- Improves survival and reduces adverse outcomes when activated early
6. Viscoelastic testing (TEG/ROTEM)
- Used alongside or instead of empiric MTP
- Guides targeted component therapy (when to give FFP, cryoprecipitate, platelets, or TXA)
- EAST guidelines endorse TEG in trauma and ICU patients
- Mortality benefit over empiric MTP in penetrating trauma receiving >10 units pRBCs (33% vs. 54% mortality in one study)
7. Vasopressors
-
Minimal evidence for routine use in haemorrhagic shock
-
May be used as a temporising measure while blood products are administered
-
A "vasopressin-deficient" state has been described; vasopressin administration can be helpful in this subset
-
Sabiston Textbook of Surgery; Mulholland & Greenfield's Surgery, 7th ed; Miller's Anesthesia, 10th ed
Keep Warm - Prevent/Treat Hypothermia
- Warm all IV fluids and blood products
- Warm environment, active patient warming
- Goal: prevent the lethal triad
Damage Control Surgery
- Early operative bleeding control without full repair
- Temporary vascular shunts, abdominal packing, abbreviated laparotomy
- Definitive repair once patient physiology is restored in ICU
Endpoints of Resuscitation
Normalisation of:
- Vital signs (HR, BP, urine output >30 mL/h)
- Mental status
- Base deficit (towards >-2 mEq/L)
- Serum lactate (clearance rate is prognostic)
- CVP / IVC collapse on ultrasound (distinguishes cardiogenic from hypovolaemic shock)
Complications
| Early | Late |
|---|---|
| Exsanguination / cardiac arrest | ARDS |
| Acute kidney injury | Multi-organ dysfunction syndrome (MODS) |
| Coagulopathy / DIC | Abdominal compartment syndrome |
| Hypothermia | Nosocomial infection |
| Metabolic acidosis | Transfusion-related complications (TRALI, TACO, transfusion reactions) |
Special Populations
- Pregnancy: Circulating blood volume increases progressively; significantly larger blood loss required before haemodynamic compromise is apparent
- Elderly: Cannot mount adequate tachycardia; often on beta-blockers or anticoagulants; haemorrhagic shock is rapidly progressive and unpredictable
- TBI with haemorrhagic shock: Permissive hypotension contraindicated; requires higher BP targets to maintain cerebral perfusion pressure
Recent Evidence (2024-2026)
- A 2025 systematic review on adjuvant therapies (PMID: 40158128) examined emerging adjuncts beyond standard DCR
- A 2025 network meta-analysis (PMID: 41380067) on fluid resuscitation strategies in emergency settings found blood-based resuscitation strategies superior to crystalloid-based
- A 2026 meta-analysis (PMID: 41885281) compared REBOA vs. resuscitative thoracotomy for non-compressible torso haemorrhage, adding to the growing literature on endovascular haemorrhage control
Summary Mnemonic: "HALT the Shock"
- H - Haemorrhage control (direct pressure, TXA, surgery/REBOA)
- A - Avoid crystalloids (use blood products 1:1:1)
- L - Low BP tolerance (permissive hypotension unless TBI)
- T - Temperature / Triad prevention (warm fluids, prevent hypothermia/acidosis/coagulopathy)
This is a shared conversation. Sign in to Orris to start your own chat.