Perkinson disease features reduced
"Parkinson disease"[MeSH Terms] AND pathophysiology
Parkinson's Disease - Reduced Features
1. Dopaminergic System (Core Deficit)
| Reduced Item | Detail |
|---|---|
| Dopamine | Primary neurochemical deficit - depletion in the neostriatum due to nigrostriatal neuron loss |
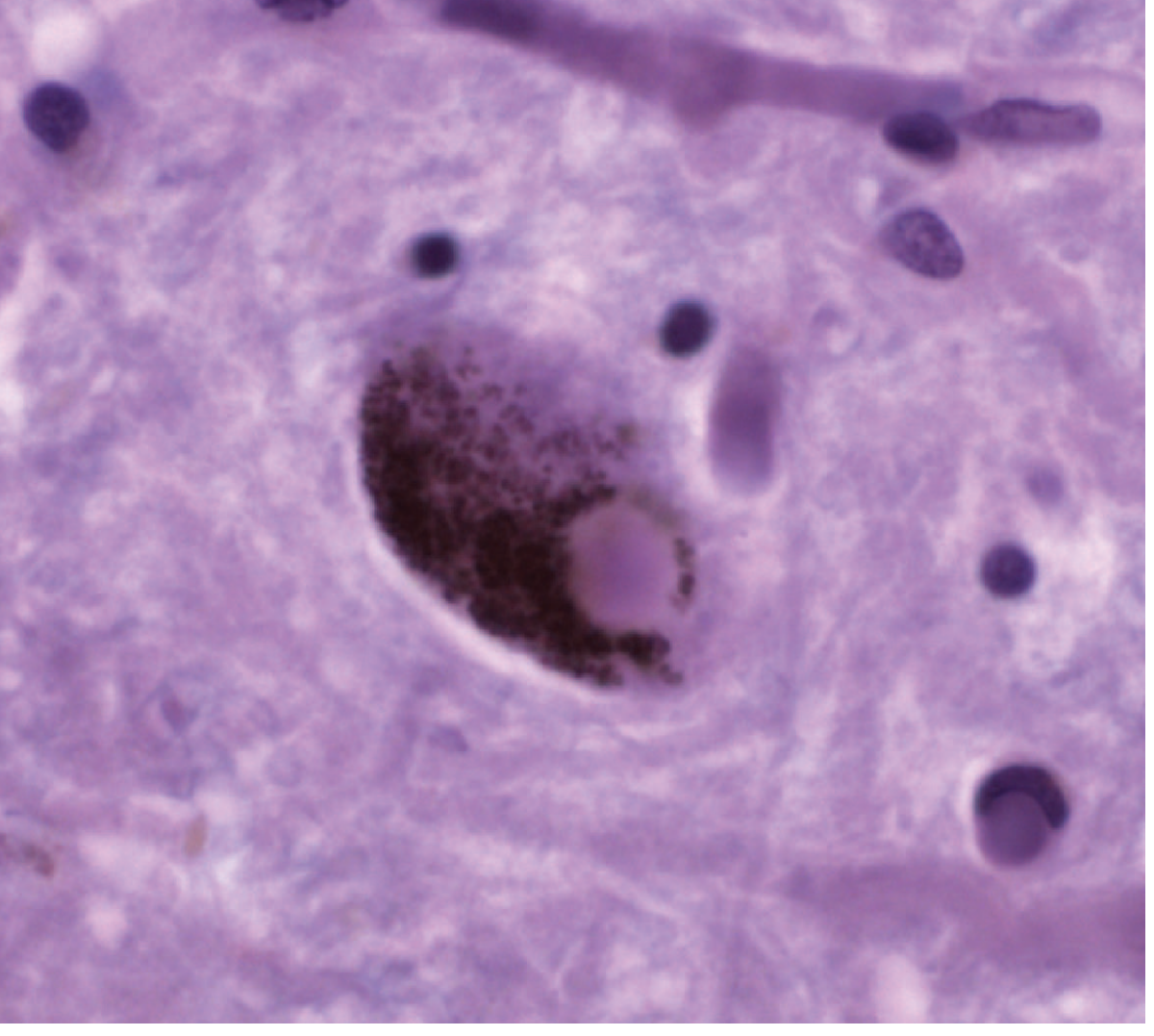
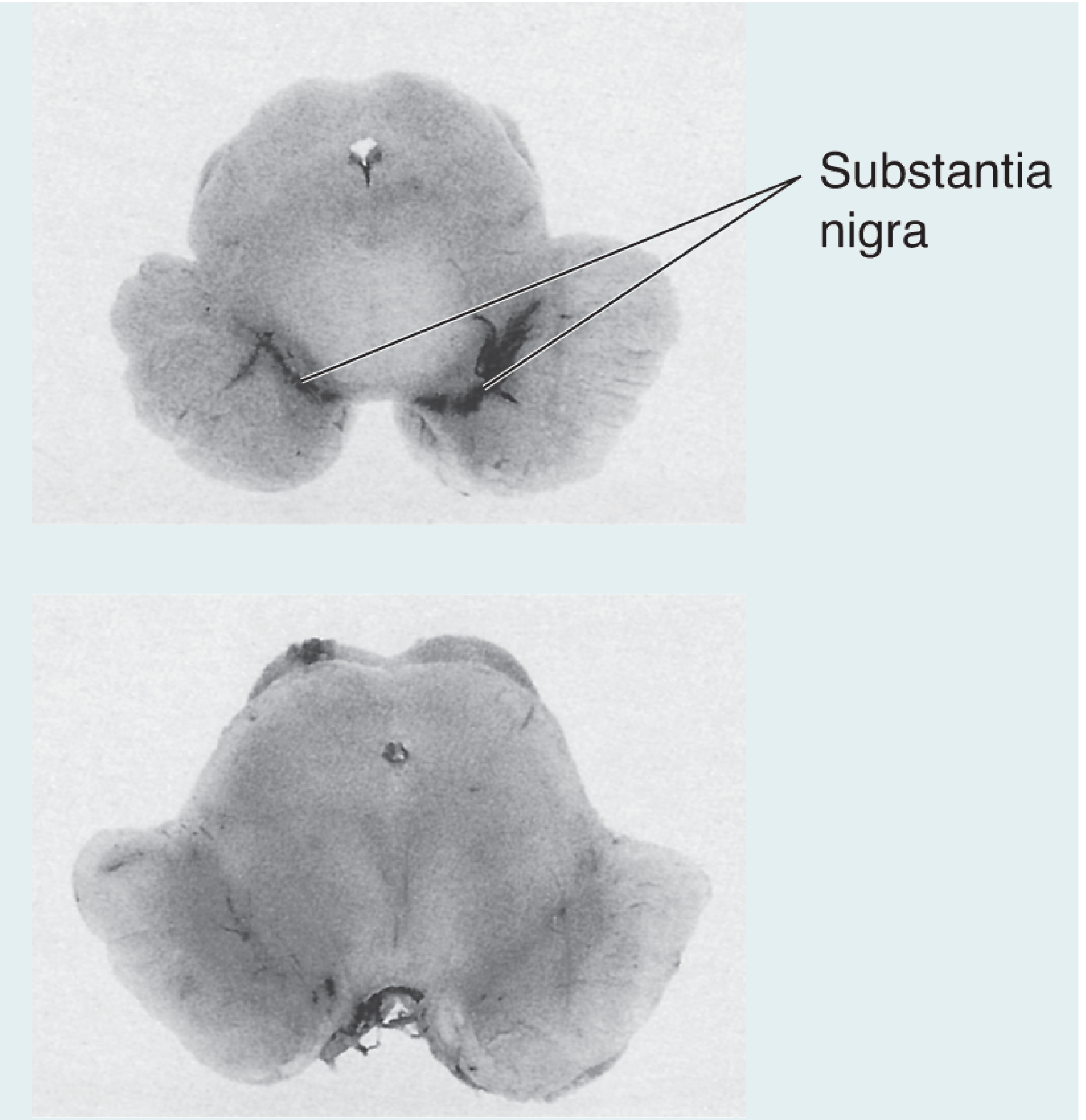
| Dopaminergic neurons (substantia nigra pars compacta) | Reduced to 30% or less of age-matched controls; absolute number reduced by ~66% |
| Tyrosine hydroxylase | Rate-limiting enzyme for dopamine synthesis - diminishes correspondingly with neuron loss |
| Dopamine transporter (DAT) | Abnormal/reduced on imaging |
| Melanin-containing neurons | Loss of pigmented (neuromelanin-rich) neurons in substantia nigra - visible as depigmentation at autopsy |
2. Biochemical Reductions Within Nigral Neurons
| Reduced Item | Significance |
|---|---|
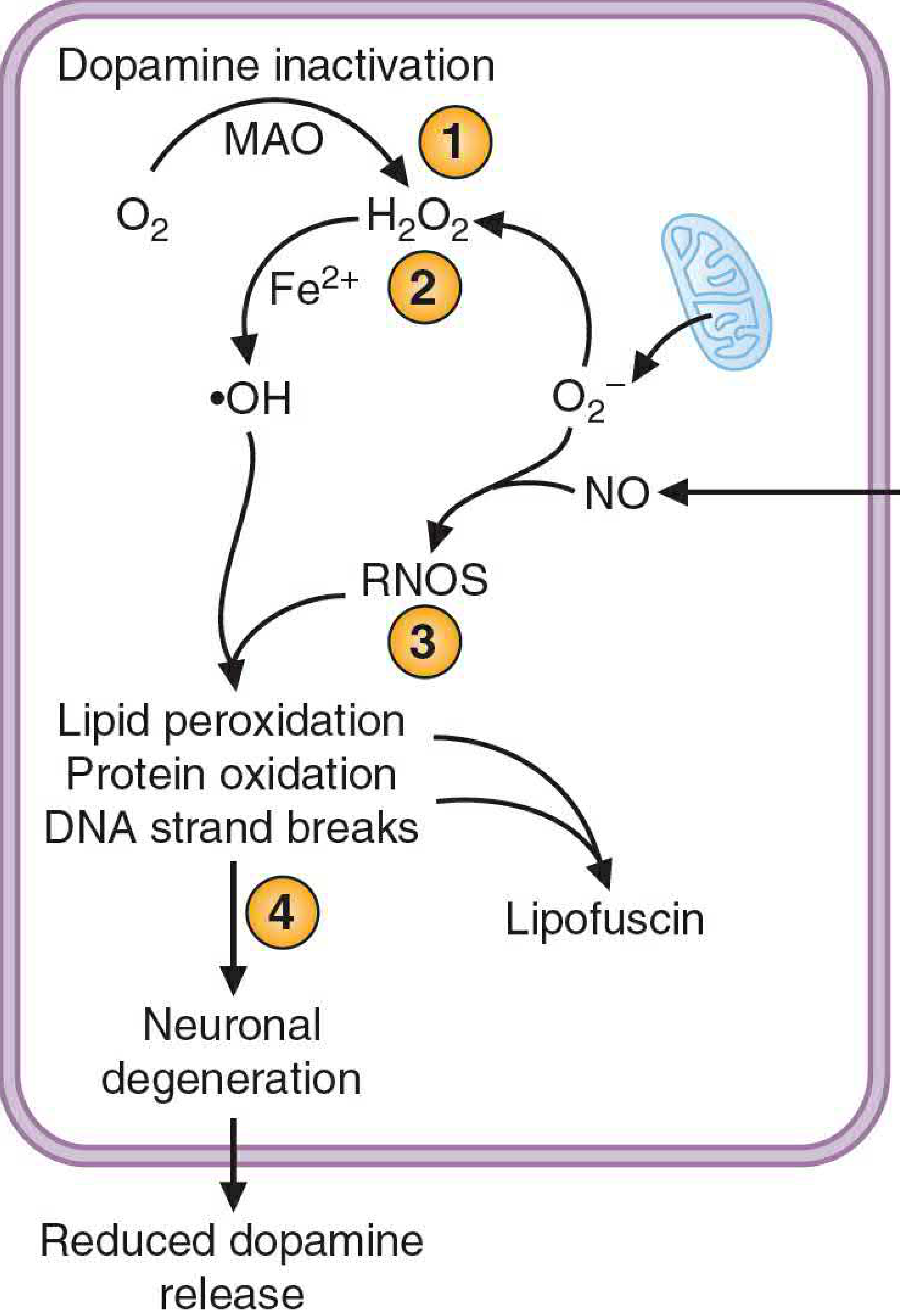
| Glutathione | Antioxidant defense is reduced, increasing vulnerability to oxidative stress |
| Complex I activity (mitochondrial) | Reduced by 30-40% - impairs ATP production |
| ATP production | Reduced, negatively affects the ubiquitin-proteasome degradation pathway |
| Ferritin (iron storage form) | Lower ferritin with increased free iron - promotes Fenton reaction and hydroxyl radical formation |
| NADH:CoQ oxidoreductase activity | Inhibited (mirrored by MPTP toxicity model) |
3. Other Neurotransmitter / Neurochemical Reductions
| Reduced Item | Region / Note |
|---|---|
| Norepinephrine | Locus ceruleus neurons are lost - explains autonomic and mood symptoms |
| Serotonin | Reduced in brainstem raphe nuclei - contributes to depression in PD |
| Acetylcholine (relative) | Cholinergic tone is relatively preserved but dopamine-ACh balance is disrupted (ACh relatively dominant, but absolute ACh can also be reduced in dementia-PD overlap) |
4. Structural / Cellular Reductions
| Reduced Item | Detail |
|---|---|
| Pigmented neurons (locus ceruleus) | Lewy bodies present here with neuronal loss |
| Neurons in mesencephalic reticular formation | Project to thalamus and limbic lobes |
| Sympathetic ganglia neurons (slight) | Contributes to autonomic dysfunction |
| Cardiac MIBG (metaiodobenzylguanidine) uptake | Reduced in PD - useful to distinguish from MSA and PSP (normal in those) |
5. Functional / Pathway Reductions
| Reduced Item | Consequence |
|---|---|
| Striatal dopaminergic drive to putamen-globus pallidus pathway | Reduced inhibition of subthalamic nucleus → GPi hyperactivity → motor symptoms |
| GABA influence on subthalamic nucleus | Reduced, rendering globus pallidus interna hyperactive |
| Alpha-synuclein solubility | Aggregates into filaments (Lewy bodies) - not "reduced" per se but its normal soluble form is functionally lost |
| Olfactory function | Reduced (anosmia is an early non-motor feature - dorsal olfactory nucleus affected early per Braak staging) |
Summary Table at a Glance
| Category | What is Reduced |
|---|---|
| Neurons | Pigmented dopaminergic neurons (SN), locus ceruleus, raphe, sympathetic ganglia |
| Neurotransmitters | Dopamine (primary), norepinephrine, serotonin |
| Enzymes | Tyrosine hydroxylase, Complex I, NADH:CoQ oxidoreductase |
| Antioxidants | Glutathione, ferritin |
| Energy | ATP (mitochondrial dysfunction) |
| Imaging | DAT scan uptake, cardiac MIBG |
| Clinical function | Smell (anosmia), gut motility, autonomic function |
A 60-year-old male is suffering from difficulty in initiation of any motor activity. While sitting he is having tremor in his hand which stops during any activity. Doctors also noted, along with change of emotions, there is no change in facial expression. i. What is your probable diagnosis? ii. Explain the pathophysiology of the disease with a diagram. iii.explain the physiological basis of hyperkinesia iv. Name two drugs used to reduce hypokinesia in this patient. v. What type of rigidity is seen in this patient and how does it differ from the rigidity of upper motor neuron lesion? 1+6+3+2+3
Clinical Case Answer: Parkinson's Disease
i. Probable Diagnosis (1 mark)
| Feature | Significance |
|---|---|
| Difficulty initiating motor activity | Akinesia / bradykinesia |
| Tremor at rest that stops during activity | Classic resting tremor (pill-rolling, 4-6 Hz) |
| Change in emotions without change in facial expression | Hypomimia (mask-like facies) - loss of spontaneous facial expression despite intact emotional processing |
| Age 60, male | Classic demographic |
ii. Pathophysiology with Diagram (6 marks)
Core Lesion
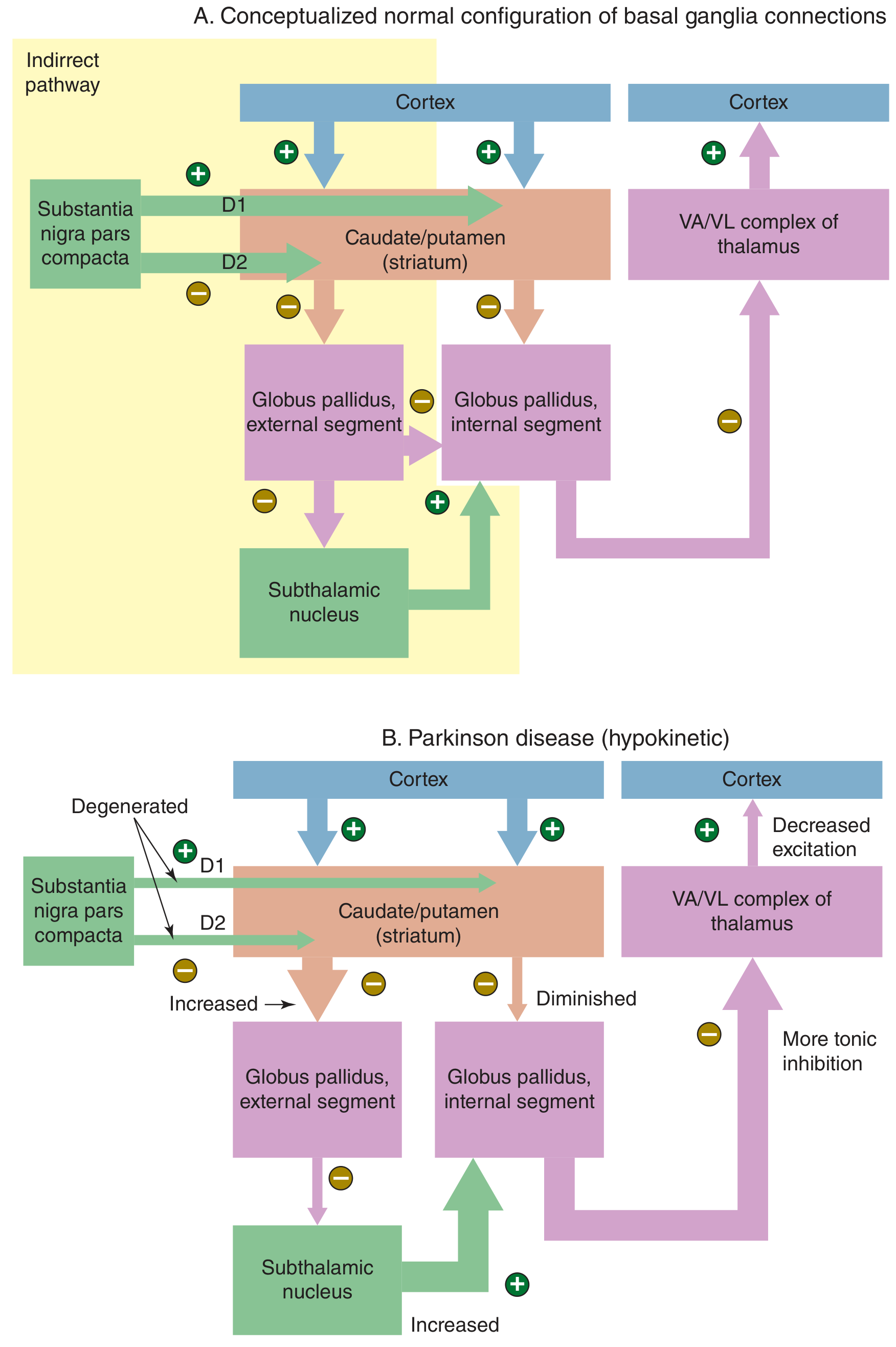
Normal Basal Ganglia Circuit
Cortex → Striatum → GPi (inhibit) → Thalamus disinhibited → Cortex excited → Movement initiated
Cortex → Striatum → GPe (inhibit) → Subthalamic Nucleus disinhibited → GPi excited → Thalamus inhibited → Movement suppressed
- D1 receptors on direct pathway neurons → excites them (facilitates movement)
- D2 receptors on indirect pathway neurons → inhibits them (reduces suppression of movement)
In Parkinson's Disease - Loss of Dopamine
| Pathway | Effect of Dopamine Loss |
|---|---|
| Direct pathway | Less D1 stimulation → striatum LESS inhibits GPi → GPi becomes MORE active |
| Indirect pathway | Less D2 inhibition → striatum LESS inhibits GPe → GPe inhibits STN less → STN becomes MORE active → STN excites GPi MORE |
| Net result | GPi is overactive → excessively inhibits VA/VL thalamus → decreased thalamo-cortical excitation → hypokinesia |
Summary Flow:
↓ Dopamine (SNpc degeneration)
↓
Direct pathway ↓ + Indirect pathway ↑
↓
GPi OVERACTIVATED
↓
VA/VL Thalamus OVER-INHIBITED
↓
Motor Cortex UNDER-STIMULATED
↓
HYPOKINESIA / AKINESIA / BRADYKINESIA
iii. Physiological Basis of Hyperkinesia (3 marks)
| Step | Event |
|---|---|
| 1 | Loss of striatal neurons (especially those of the indirect pathway) |
| 2 | Striatum LESS inhibits GPe → GPe becomes overactive |
| 3 | GPe excessively inhibits STN → STN activity falls |
| 4 | STN provides LESS excitatory drive to GPi → GPi becomes underactive |
| 5 | GPi LESS inhibits thalamus → VA/VL thalamus disinhibited |
| 6 | Thalamus over-excites motor cortex → excess, unwanted movements |
"Decreased basal ganglia output leads to hyperkinesia, an excess of movement." - Neuroscience: Exploring the Brain, 5th Ed.
iv. Two Drugs Used to Reduce Hypokinesia (2 marks)
- Levodopa (L-DOPA) + Carbidopa
- Levodopa is the dopamine precursor that crosses the blood-brain barrier and is converted to dopamine in surviving nigral neurons and striatum.
- Carbidopa is a peripheral decarboxylase inhibitor - prevents peripheral conversion of L-DOPA, reducing side effects and increasing CNS bioavailability.
- Most effective drug for hypokinesia/bradykinesia in PD.
- Dopamine Agonists (e.g., Pramipexole, Ropinirole, Bromocriptine)
- Directly stimulate D2 (and D1/D3) receptors in the striatum, bypassing degenerating neurons entirely.
- Used as monotherapy in early PD or as adjuncts to levodopa in later stages.
- Reduce "off" time and improve motor function.
v. Type of Rigidity in Parkinson's vs UMN Lesion Rigidity (3 marks)
In Parkinson's Disease: Cogwheel Rigidity (type of Lead-Pipe/Plastic Rigidity)
| Feature | Detail |
|---|---|
| Type | Cogwheel rigidity (also described as plastic or lead-pipe rigidity) |
| Mechanism | Extrapyramidal - loss of dopaminergic modulation of basal ganglia → tonic overactivity of alpha motor neurons via reticulospinal pathways |
| Character | Ratchet-like, intermittent "catches" felt during passive movement (due to superimposed resting tremor on underlying plastic rigidity) |
| Velocity dependence | Velocity-independent - same resistance throughout the range of motion regardless of speed of passive stretch |
| Muscles affected | Both flexors and extensors equally |
| Distribution | Often starts asymmetrically (one limb), then generalizes |
Comparison: Cogwheel (PD) vs Clasp-Knife (UMN) Rigidity
| Feature | Cogwheel Rigidity (PD/Extrapyramidal) | Clasp-Knife Rigidity (UMN/Spasticity) |
|---|---|---|
| Mechanism | Basal ganglia dysfunction - extrapyramidal | Corticospinal tract lesion - pyramidal |
| Velocity dependence | Velocity-independent | Velocity-dependent (increases with faster stretch) |
| Character | Ratchet/cog-wheel feel - uniform interrupted resistance | Initial resistance then sudden "give" (like a clasp-knife opening) |
| Muscles predominantly affected | Flexors AND extensors equally | Predominantly antigravity muscles - upper limb flexors, lower limb extensors |
| Tendon reflexes | Normal or mildly increased | Hyperreflexia (brisk DTRs) |
| Plantar response | Flexor (normal) | Extensor (Babinski sign) |
| Associated clonus | Absent | Often present |
| Distribution | Limb, neck, trunk; often asymmetric | Hemi/para/quadriplegia pattern |
| Examples | Parkinson's disease, other parkinsonian syndromes | Stroke, MS, spinal cord injury, cerebral palsy |
"Spasticity is velocity dependent, has a sudden release after reaching a maximum (the 'clasp-knife' phenomenon)... Rigidity is hypertonia that is present throughout the range of motion ('lead pipe' or 'plastic' stiffness) and affects flexors and extensors equally; it sometimes has a cogwheel quality." - Harrison's Principles of Internal Medicine, 22e
A 60 year old hypertensive male has presented with weakness and inability to move his right upper and lower extremities since last 2 hours. After admission in nearby hospital, clinical examination revealed increased muscle tone, exaggerated tendon jerks and extensor plantar response on his right side. i) What can be the probable diagnosis? ii) Explain the reason behind the increased muscle tone and exaggerated tendon jerks in this patient. iii) Why the planter response is altered here? iv) Describe the corticospinal tract with a suitable diagram.1+4+3+5+2
Clinical Case Answer: Left-Sided Stroke / UMN Lesion
i. Probable Diagnosis (1 mark)
- 60-year-old hypertensive male (major risk factor for stroke)
- Acute onset weakness of right upper and lower extremities (right hemiplegia) = contralateral to the lesion, since the corticospinal tract crosses at the pyramidal decussation
- Increased tone + exaggerated jerks + extensor plantar = classic upper motor neuron (UMN) syndrome
- Presentation within 2 hours = acute stroke
ii. Increased Muscle Tone and Exaggerated Tendon Jerks (4 marks)
Mechanism of Increased Muscle Tone (Spasticity)
"Spasticity is caused by damage to descending inhibitory pathways that travel closely with the corticospinal tract. Loss of these descending inhibitory influences may lead to increased excitability of motor neurons in the anterior horn, resulting in brisk reflexes and increased tone." - Neuroanatomy through Clinical Cases, 3rd Ed.
Mechanism of Exaggerated Tendon Jerks (Hyperreflexia)
- Muscle spindle → Ia afferent → Spinal cord → Alpha motor neuron → Muscle contraction
| Normal | UMN Lesion |
|---|---|
| Descending inhibition keeps reflex arc under control | Descending inhibition is LOST |
| Alpha MN threshold is higher | Alpha MN is hyperexcitable |
| Gamma MN activity is modulated | Gamma MN activity is increased → spindles hypersensitive |
| Tendon tap → normal response | Same tap → exaggerated response = hyperreflexia |
iii. Why the Plantar Response is Altered (Extensor Plantar / Babinski Sign) (3 marks)
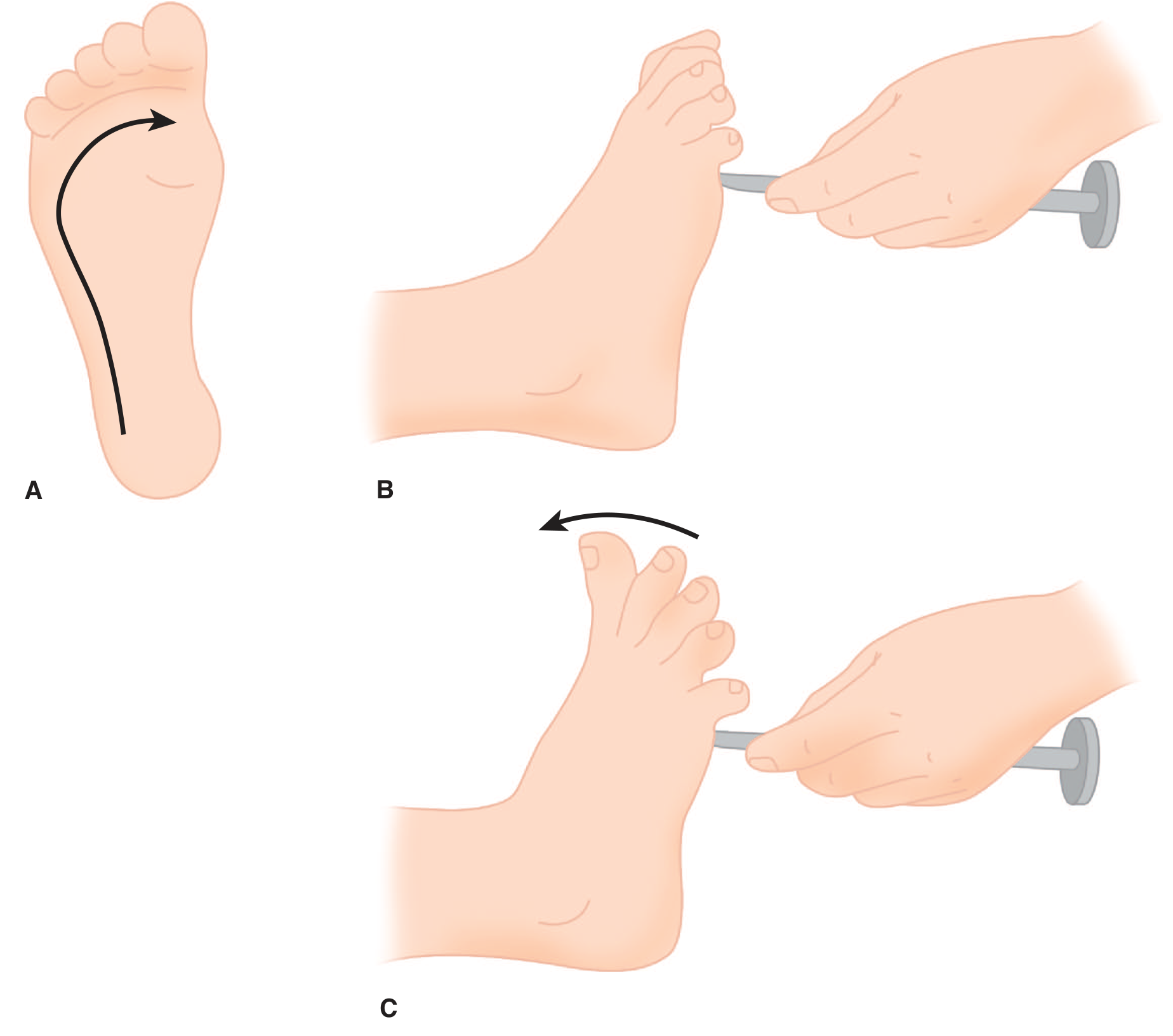
Normal Plantar Response
Altered (Extensor) Plantar Response - Babinski Sign
-
The corticospinal tract normally exerts tonic inhibitory control over spinal flexor withdrawal (nocifensive) reflex programs in the spinal cord.
-
When the corticospinal tract is damaged, this inhibitory control is released (disinhibited).
-
The primitive nociceptive flexor withdrawal reflex (also called "triple flexion response") is unmasked - this is a phylogenetically ancient protective spinal reflex.
-
The hallmark of this reflex is that what appears to be "extension" of the great toe is actually part of a limb withdrawal pattern: the big toe dorsiflexes (extends) while the ankle dorsiflexes and hip/knee flex - this is the body withdrawing the limb from a noxious stimulus.
-
The other toes fan outward (abduct) - completing the Babinski sign.
"The extension movement of the great toe is a component of a larger synergistic flexion or shortening reflex of the leg... These spinal flexion reflexes, of which the Babinski sign is the most characteristic, are present because of disinhibition or release of motor programs of spinal origin." - Adams and Victor's Principles of Neurology, 12th Ed.
iv. Corticospinal Tract - Description with Diagrams (5 marks)
Definition
Origin - Upper Motor Neurons
| Source | Brodmann Area | Contribution |
|---|---|---|
| Primary motor cortex (precentral gyrus) | Area 4 | >50% of fibers |
| Premotor and supplementary motor areas | Area 6 | Planning/initiation |
| Somatosensory cortex (postcentral gyrus) | Areas 3, 1, 2, 5, 7 | Sensory modulation of movement |
- Neurons are large layer V pyramidal cells
- ~3% are giant Betz cells - the largest neurons in the human nervous system
- Somatotopic organization follows the motor homunculus: face lateral, hand/arm middle, trunk and leg medial (dipping into longitudinal fissure)
Course of the Corticospinal Tract
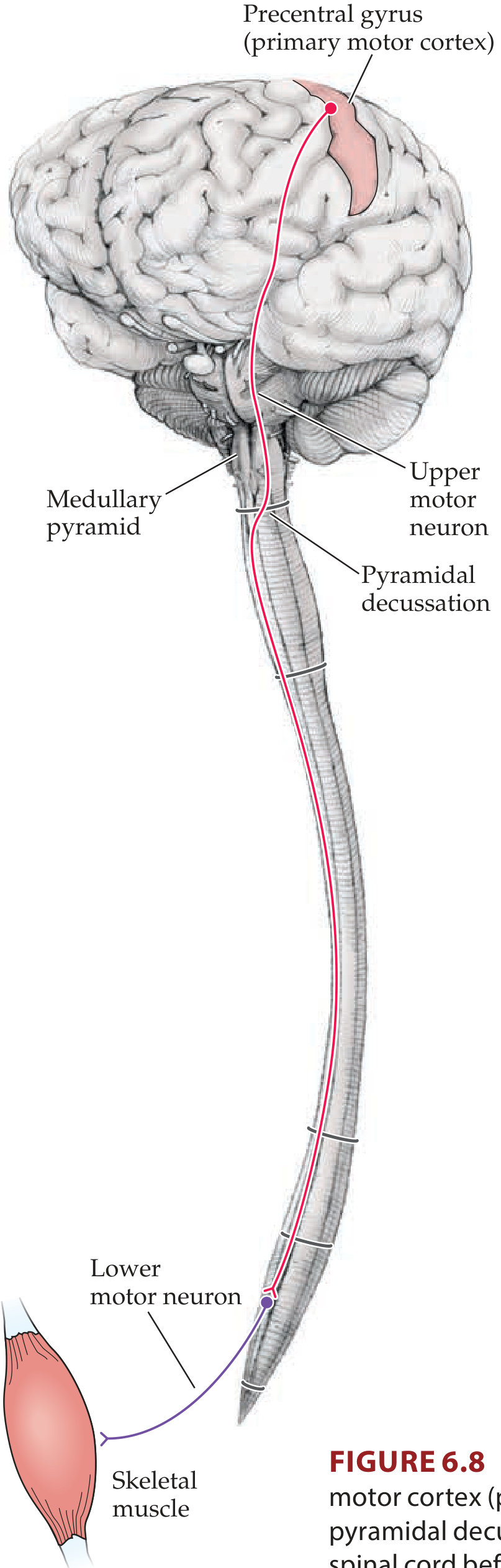
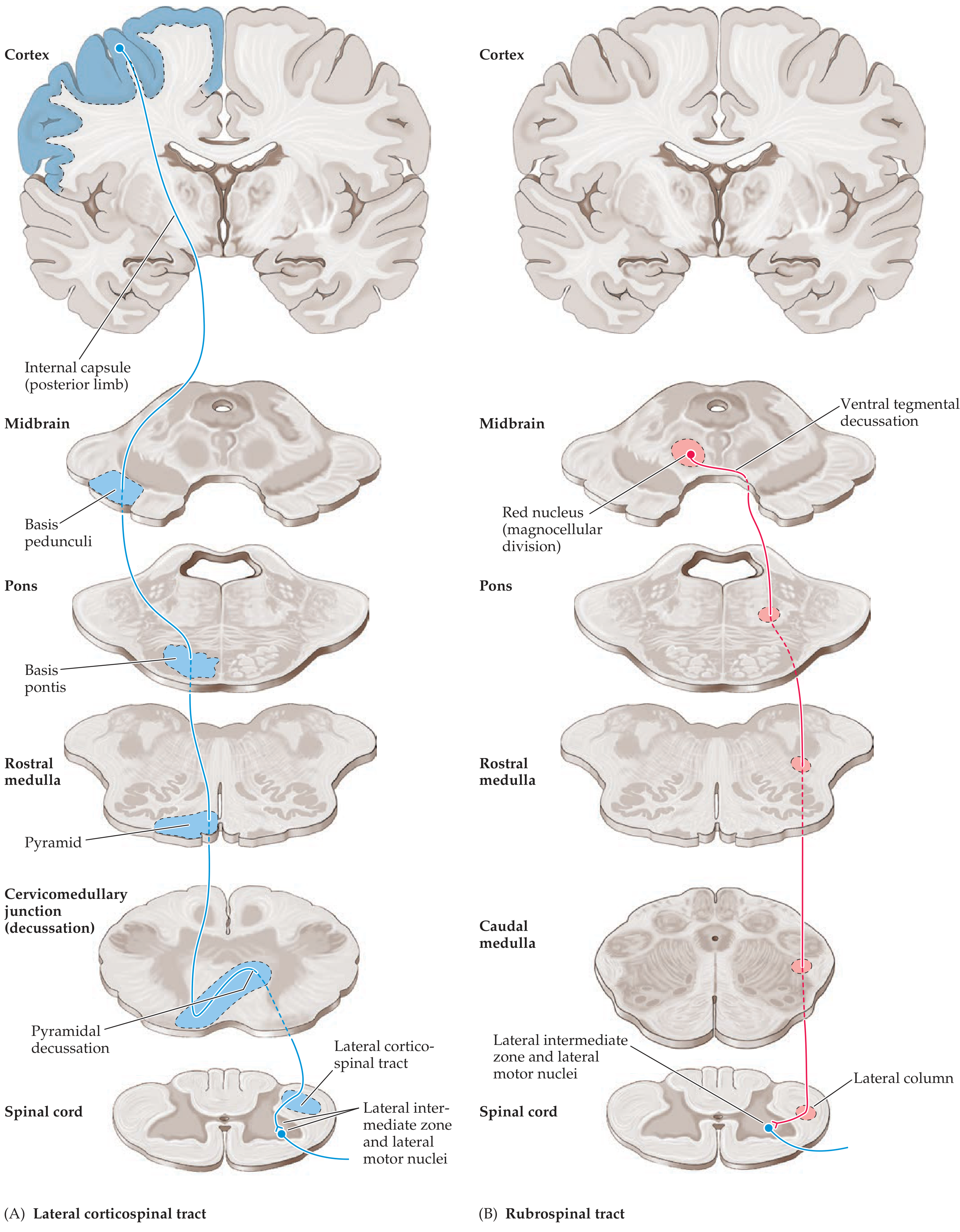
| Level | Anatomical Location | Key Point |
|---|---|---|
| Cerebral cortex | Precentral gyrus (area 4, 6) | Origin - UMN cell bodies |
| Corona radiata | Fan-shaped white matter in cerebral hemispheres | Fibers converge downward |
| Internal capsule | Posterior limb | Compact fibers: face anterior, arm middle, leg posterior |
| Cerebral peduncles (midbrain) | Middle 1/3 of basis pedunculi | Face medial → leg lateral arrangement |
| Pons | Basis pontis | Fibers scattered into fascicles by transverse pontine fibers |
| Medulla | Medullary pyramids (ventral surface) | This is why the tract is also called the "pyramidal tract" |
| Pyramidal decussation | Cervicomedullary junction (foramen magnum) | ~85% of fibers cross to contralateral side |
| Spinal cord | Lateral corticospinal tract (lateral white column) | Remaining ~15% stay ipsilateral = anterior corticospinal tract |
| Spinal anterior horn | Synapse on lower motor neurons (LMN) and interneurons | Final common pathway to muscle |
Key Points for This Case
LEFT Motor Cortex (Area 4)
↓
Left Corona Radiata
↓
LEFT Posterior Limb of Internal Capsule ← LESION HERE (stroke)
↓
Left Cerebral Peduncle
↓
Left Medullary Pyramid
↓
Pyramidal Decussation (85% cross)
↓
RIGHT Lateral Corticospinal Tract
↓
RIGHT Anterior Horn LMNs
↓
RIGHT Upper + Lower Limb Muscles → WEAKNESS
Summary of UMN vs LMN Signs
| Feature | UMN Lesion (this patient) | LMN Lesion |
|---|---|---|
| Tone | Increased (spasticity) | Decreased (flaccidity) |
| Reflexes | Exaggerated (hyperreflexia) | Diminished/absent |
| Plantar response | Extensor (Babinski +ve) | Flexor (normal) |
| Atrophy | Absent (mild disuse only) | Prominent |
| Fasciculations | Absent | Present |
| Distribution | Face + arm + leg (if internal capsule) | Only muscles of affected LMN |
.A 60 year old male,reported difficulty in initiating any motor activity like walking ,brushing his teeth etc.Doctors also noted that,while he is sitting,there was tremor in his hand and this tremor stopped while doing any activity.It was also noted that there is no change in facial expression along with the change of emotion.On CNS examination,it was revealedthere is hypertonia with Cog wheel rigidity,pill rollingtremor in his hand and festinant gait,Cerebellar,sensory,cortical amnd higher functions were normal. a.What is your provisional diagnosis? b.Give the pathophysiological basis of this disease with diagram. c.What is the Physiological basis of hypokinesia? d.What is the physiological basis of tremor?
Clinical Case Answer: Parkinson's Disease
a. Provisional Diagnosis
| Feature Reported | Parkinsonian Sign |
|---|---|
| Difficulty initiating motor activity (walking, brushing) | Akinesia / Bradykinesia |
| Resting tremor in hand that stops during activity | Resting (pill-rolling) tremor |
| No change in facial expression despite change in emotion | Hypomimia (mask-like facies) |
| Hypertonia with cogwheel rigidity | Extrapyramidal rigidity |
| Festinant gait | Classic shuffling, accelerating gait of PD |
| Normal cerebellar, sensory, cortical and higher functions | Rules out cerebellar ataxia, sensory ataxia, cortical dementia |
b. Pathophysiological Basis with Diagram
Primary Lesion
Normal Basal Ganglia Circuit
Cortex → Striatum (GABA/Substance P) → inhibits GPi → GPi releases thalamus → Thalamus (VA/VL) excites Cortex → Movement facilitated
Cortex → Striatum (GABA/enkephalin) → inhibits GPe → GPe releases STN → STN excites GPi → GPi inhibits thalamus → Movement suppressed
- Acts on D1 receptors on direct pathway neurons → excites them (↑ movement facilitation)
- Acts on D2 receptors on indirect pathway neurons → inhibits them (↓ movement suppression)
- Net result = dopamine promotes voluntary movement via both pathways
In Parkinson's Disease - Loss of Dopamine
| Pathway | Change in PD | Consequence |
|---|---|---|
| Direct pathway | ↓ D1 stimulation → striatum LESS inhibits GPi | GPi becomes overactive |
| Indirect pathway | ↓ D2 inhibition → striatum LESS inhibits GPe → GPe LESS inhibits STN → STN overactive → STN MORE excites GPi | GPi becomes even more overactive |
| Net result | GPi excessively inhibits VA/VL thalamus | Thalamo-cortical drive falls → hypokinesia |
↓ Dopamine (SNpc degeneration)
↓
Direct pathway ↓ + Indirect pathway ↑
↓
GPi (globus pallidus interna) OVERACTIVE
↓
VA/VL Thalamus OVER-INHIBITED
↓
Motor Cortex UNDER-STIMULATED (especially SMA)
↓
AKINESIA / BRADYKINESIA / HYPOKINESIA
"Depletion of dopamine in Parkinson's disease closes the funnel that feeds activity to cortical area SMA via the basal ganglia and VL thalamus." - Neuroscience: Exploring the Brain, 5th Ed.
c. Physiological Basis of Hypokinesia
Step-by-step mechanism:
- Dopamine normally stimulates D1 receptors on striatal neurons of the direct pathway
- Without dopamine, D1 stimulation ↓ → direct pathway neurons fire less
- Less GABA released onto GPi → GPi is less inhibited → GPi fires more
- Dopamine normally inhibits D2 receptors on indirect pathway striatal neurons
- Without dopamine, D2 inhibition is lost → indirect pathway neurons fire more
- More GABA released onto GPe → GPe is more inhibited → GPe fires less
- Less GPe inhibition on STN → STN fires more
- More STN excitation of GPi → GPi fires even more
- An overactive GPi sends excessive GABA-ergic inhibitory output to the VA/VL nuclei of the thalamus
- Thalamo-cortical relay neurons are suppressed
- The supplementary motor area (SMA) receives reduced thalamic input
- SMA is critically important for self-initiated (internally cued) movements - e.g., deciding to start walking or brushing teeth
- With reduced SMA activation, voluntary movement initiation fails → hypokinesia / akinesia
- The SMA is impaired for internally-generated, self-paced movement
- Externally-cued movements (responding to a visual cue on the floor, or marching to music) can be relatively preserved because they bypass the basal ganglia via the cerebellum
- Without proper stride length regulation, the patient takes increasingly rapid, short shuffling steps to compensate for a forward-displaced centre of gravity → festinant (hastening) gait
"Enhanced conduction through the indirect pathway leads to hypokinesia by increasing pallidothalamic inhibition... In Parkinson disease, a loss of dopaminergic input from the substantia nigra diminishes activity in the direct pathway and increases activity in the indirect pathway; the net effect is to increase inhibition of the thalamic nuclei and to reduce excitation of the cortical motor system." - Adams and Victor's Principles of Neurology, 12th Ed.
d. Physiological Basis of Tremor
Classic Features:
- "Pill-rolling" tremor of thumb and fingers
- Suppressed during voluntary movement (action)
- Worsens with stress or distraction
- Disappears during sleep
Mechanism - Oscillatory Loop Hypothesis:
Summary - Tremor Circuit:
↓ Dopamine
↓
STN overactive → rhythmic burst firing (4-6 Hz)
↓
GPi oscillates
↓
Thalamus (VA/VL) oscillates
↓
Motor cortex driven rhythmically
↓
Alternating agonist/antagonist contraction
↓
RESTING TREMOR (pill-rolling, 4-6 Hz)
↓
Stopped by voluntary movement (sensory feedback + cerebellar override)
Summary Table: Key Pathophysiological Mechanisms
| Feature | Mechanism |
|---|---|
| Akinesia / Hypokinesia | ↓ Dopamine → overactive GPi → over-inhibited thalamus → ↓ SMA activation |
| Cogwheel Rigidity | ↓ Dopamine → altered reticulospinal/basal ganglia output → increased α and γ MN tone; superimposed tremor creates "cog" feel |
| Resting Tremor (pill-rolling) | STN-GPi-thalamo-cortical oscillatory loop at 4-6 Hz; stops with voluntary movement |
| Festinant gait | SMA dysfunction → impaired stride initiation + length; forward lean leads to accelerating short steps |
| Hypomimia | Loss of dopaminergic drive to facial motor circuits (corticobulbar + basal ganglia) → reduced spontaneous facial expression |
Physiological Basis of Tremor (3 Marks)
Physiological Basis of Tremor in Parkinson's Disease (3 Marks)
Definition and Character
Physiological Mechanism
Step-by-Step Basis:
Why Tremor Stops During Voluntary Movement?
- The motor cortex generates a strong, purposeful command that overrides the oscillatory thalamic input
- Active limb movement generates sensory (proprioceptive) feedback that disrupts the re-entrant oscillatory loop
- The intact cerebellum provides real-time error correction and damping during movement
Summary Diagram:
↓ Dopamine (SNpc degeneration)
↓
STN overactive → synchronous rhythmic bursts (4-6 Hz)
↓
GPi oscillates (4-6 Hz)
↓
VA/VL Thalamus → rhythmic rebound firing
↓
Motor Cortex → pulsatile motor commands
↓
Alternating agonist/antagonist contractions
↓
RESTING TREMOR - "pill-rolling" (4-6 Hz)
↓ (voluntary movement)
Sensory feedback + cortical override → TREMOR STOPS
Types of Tremor - Comparison for Context
| Feature | Parkinsonian (Resting) | Essential (Postural) | Cerebellar (Intention) |
|---|---|---|---|
| Frequency | 4-6 Hz | 5-10 Hz | 2-4 Hz |
| When present | At rest | Holding posture | During movement toward target |
| Stops with | Voluntary movement | Nothing (persists on action) | N/A (worsens on action) |
| Location | Hands, jaw, lips (not head) | Hands, head, voice | Limbs |
| Structure involved | Basal ganglia-thalamic loop | Cerebello-thalamic circuit | Cerebellum/superior cerebellar peduncle |