Ankle joint Wirh figure
Reading File
Finding Sources
Searching the Web
ankle joint anatomy bones ligaments movements
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
I now have comprehensive content and all the key figures. Let me compile the full answer.
Ankle Joint (Talocrural Joint)
Source: Gray's Anatomy for Students, pp. 744-746
Type and Classification
The ankle joint (also called the talocrural joint) is a synovial hinge joint. It primarily permits dorsiflexion and plantarflexion of the foot on the leg.
Bones / Articular Surfaces
Three bones form the joint:
| Component | Structure formed |
|---|---|
| Tibia (inferior surface) | Roof of the socket |
| Medial malleolus (tibia) | Medial wall of the socket |
| Lateral malleolus (fibula) | Lateral wall of the socket (longer side) |
| Talus (trochlear surface) | Fits into the bracket-shaped socket |
The distal fibula is firmly anchored to the tibia by strong tibiofibular ligaments, creating a deep bracket-shaped socket that accepts the upper expanded body of the talus. All articular surfaces are covered by hyaline cartilage.
Fig. 6.104 - Ankle Joint (Gray's Anatomy for Students):
(A) Anterior view, right foot plantarflexed; (B) Posterior schematic; (C) Superior view of talus showing articular surface shape
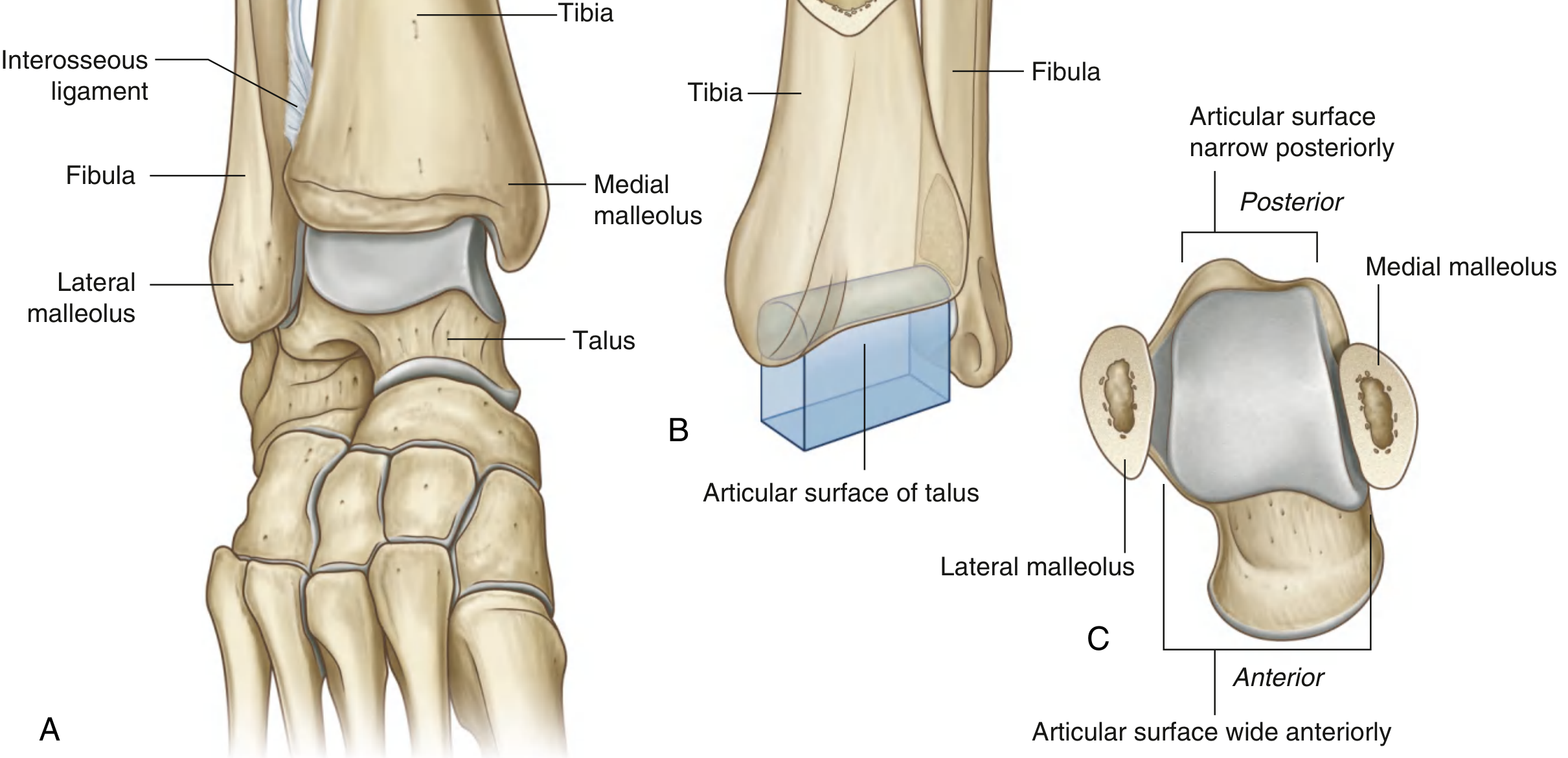
Key point on stability: When viewed from above, the talar articular surface is wider anteriorly than posteriorly. Therefore, the joint is most stable in dorsiflexion (wider part locks into the mortise) and least stable in plantarflexion (narrower part - more susceptible to sprains).
Joint Capsule
- Synovial membrane: attaches around the margins of the articular surfaces
- Fibrous membrane: overlies the synovial membrane and attaches to adjacent bones
- The anterior and posterior capsule are relatively thin; the medial and lateral ligaments provide the main stability
Ligaments
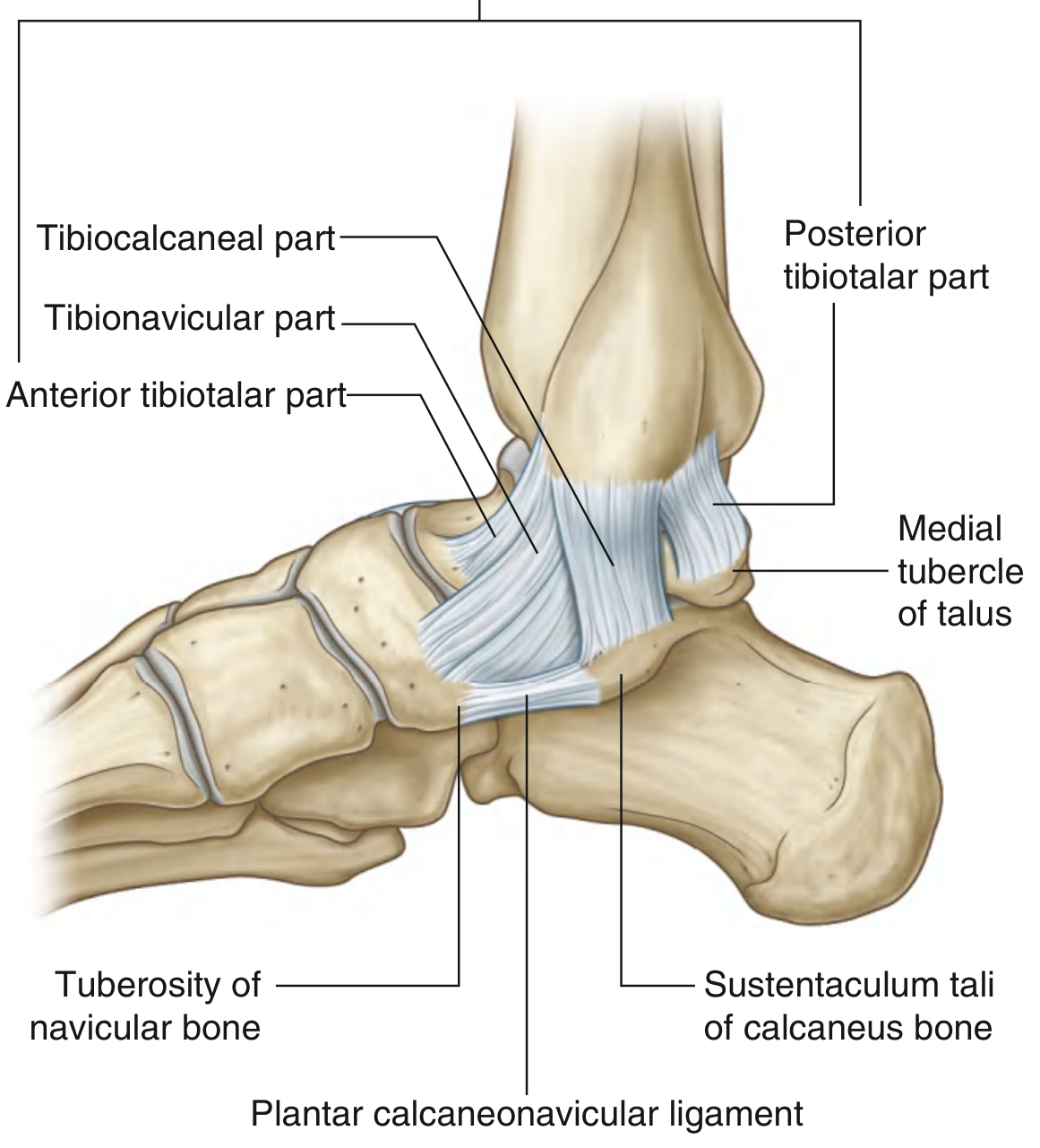
Medial Ligament (Deltoid Ligament)
The deltoid ligament is large, strong, and triangular in shape. Its apex attaches to the medial malleolus above; its broad base attaches below to a line from the navicular tuberosity anteriorly to the medial tubercle of the talus posteriorly.
It has four parts:
| Part | Attachment below |
|---|---|
| Tibionavicular | Tuberosity of navicular + plantar calcaneonavicular (spring) ligament |
| Tibiocalcaneal | Sustentaculum tali of calcaneus |
| Posterior tibiotalar | Medial side and medial tubercle of talus |
| Anterior tibiotalar | Medial surface of talus (deep layer) |
Fig. 6.105 - Medial (Deltoid) Ligament, Right Foot:
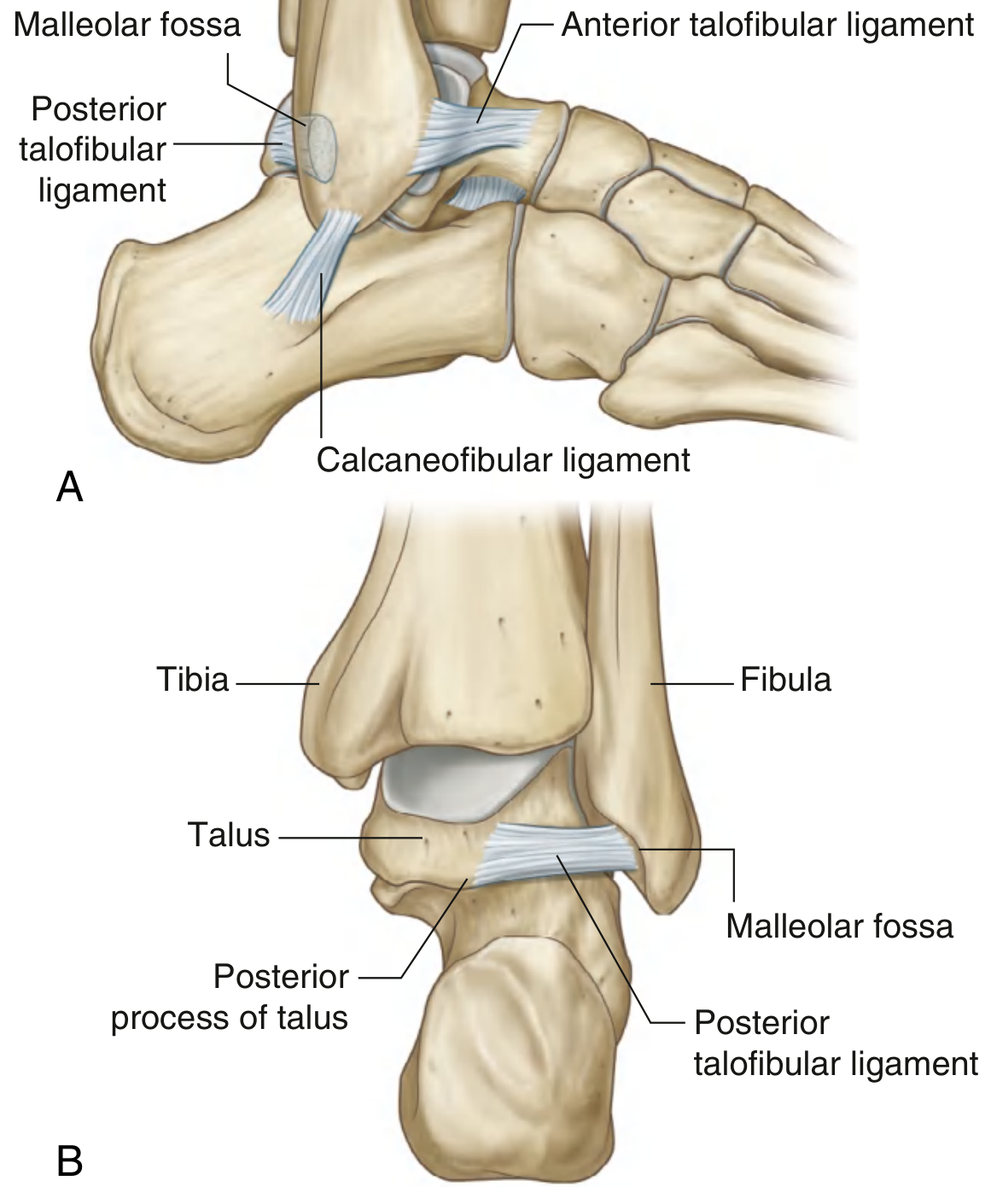
Lateral Ligament
The lateral ligament is composed of three separate ligaments:
| Ligament | From | To | Direction |
|---|---|---|---|
| Anterior talofibular (ATFL) | Anterior margin of lateral malleolus | Adjacent talus | Horizontal / anteriorly |
| Posterior talofibular (PTFL) | Malleolar fossa (medial side of lateral malleolus) | Posterior process of talus | Horizontal, backward and medially |
| Calcaneofibular (CFL) | Malleolar fossa (posteromedial lateral malleolus) | Tubercle on lateral calcaneus | Posteroinferiorly |
Fig. 6.106 - Lateral Ligament of the Ankle Joint:
(A) Lateral view, right foot; (B) Posterior view, right foot
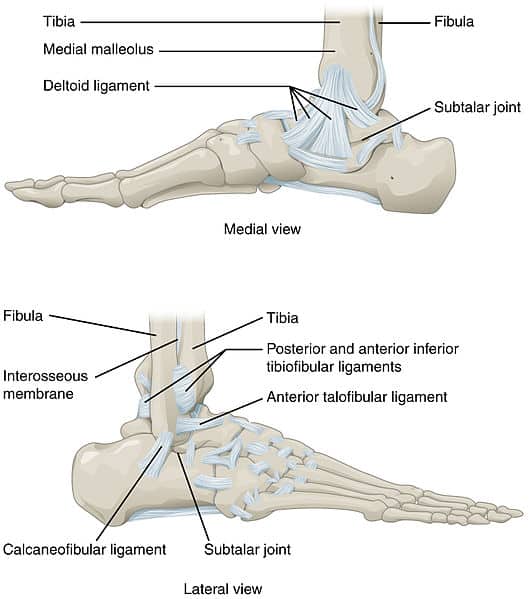
Medial vs. Lateral views (TeachMeAnatomy)
Movements
| Movement | Definition | Range |
|---|---|---|
| Dorsiflexion | Foot pulled toward shin | ~20° |
| Plantarflexion | Foot pointed downward | ~50° |
Inversion, eversion, supination, and pronation occur primarily at the subtalar and talocalcaneonavicular joints, NOT at the ankle joint proper.
Muscles producing movements:
| Movement | Muscles |
|---|---|
| Dorsiflexion | Tibialis anterior, extensor hallucis longus, extensor digitorum longus, fibularis tertius |
| Plantarflexion | Gastrocnemius, soleus, plantaris, tibialis posterior, flexor digitorum longus, flexor hallucis longus |
Nerve Supply
- Deep peroneal (fibular) nerve - anteriorly
- Tibial nerve - posteriorly
- Superficial peroneal nerve and sural nerve - contribute laterally
Blood Supply
- Anterior tibial artery (dorsalis pedis) - anterior aspect
- Posterior tibial artery - posterior aspect
- Fibular (peroneal) artery - lateral aspect
- All three vessels form an anastomotic network around the joint
Stability
The ankle is stabilized by:
- The deep bony mortise (bracket socket of tibia + fibula)
- The medial deltoid ligament - strongest, resists eversion forces
- The three lateral ligaments - resist inversion; ATFL is weakest and most commonly injured
- Surrounding tendons and muscles
Clinical note: The lateral ligament complex (especially the ATFL) is the most frequently injured structure in the ankle, accounting for ~85% of all ankle sprains, as the deltoid ligament is much stronger and the ankle is prone to inversion injuries.
Clinical Correlations
Ottawa Ankle Rules
A radiograph is needed if ankle pain is accompanied by:
- Bone tenderness along the distal 6 cm of the posterior tibia or tip of the medial malleolus
- Bone tenderness along the distal 6 cm of the posterior fibula or tip of the lateral malleolus
- Inability to bear weight for four steps immediately after injury and in the emergency department
Fracture of the Talus
The talus has a precarious blood supply - the main supply enters through the tarsal sinus from the posterior tibial artery. Fractures of the talar neck interrupt this supply, making the body of the talus susceptible to avascular necrosis (osteonecrosis).
Ankle Fractures
The ankle joint and surrounding structures form a fibro-osseous ring in the coronal plane. Any force that disrupts the ring on one side often causes disruption on the opposite side as well - so a visible fracture on X-ray should always raise suspicion of associated ligamentous injury.
Gray's Anatomy for Students, pp. 744-748
This is a shared conversation. Sign in to Orris to start your own chat.