Operations for umbilical hernias, hernias of the linea alba, and Spigelian hernias.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive material from Bailey & Love and Fischer's Mastery of Surgery. Let me compile the full answer.
Operations for Umbilical, Linea Alba (Epigastric), and Spigelian Hernias
1. Umbilical Hernia
Anatomy and Pathology
The umbilical defect is present at birth but normally closes within a week as the umbilical cord stump heals. If this is delayed, neonatal herniation results. In adults the umbilical ring may reopen when the midline raphe is stretched or thinned by pregnancy, obesity, or liver disease with ascites. Current guidelines consider any hernia in the immediate vicinity of the umbilicus (including the formerly termed "paraumbilical" variety) as an umbilical hernia.
Small hernias may contain only extraperitoneal fat; larger ones contain small or large bowel. Because the neck is narrow relative to the sac, they are prone to irreducibility, obstruction, and strangulation.

Umbilical Hernia in Children
- Occurs in up to 10% of infants; higher incidence in premature and Black infants
- Appears within weeks of birth; classic conical shape on crying
- Strangulation is extremely uncommon under age 3
- Treatment: Conservative under age 2 - 95% resolve spontaneously. Surgery if it persists beyond 2 years
Surgical technique (children): A small curved incision is made immediately below the umbilicus. The neck is defined, opened, and contents reduced. The sac is closed and excess excised. The defect in the linea alba is closed with interrupted slowly absorbable sutures.
Open Umbilical Hernia Repair (Adults)
The approach depends on defect size:
| Defect Size | Technique |
|---|---|
| < 1 cm | Simple suture repair (if fascia not under tension); or darn suture (non-absorbable monofilament criss-crossed across defect) |
| Up to 2 cm | Mayo repair ("waistcoat over trousers") |
| > 2 cm | Mesh repair strongly advised |
Mayo repair (for defects up to 2 cm):
- Transverse incision over the hernia
- Hernia sac dissected, opened, contents reduced
- Peritoneum closed
- Defect extended transversely in the linea alba
- Fascial edges closed in an overlapping style - superior flap placed on top ("waistcoat over trousers")
- Non-absorbable sutures used
- Redundant skin excised for cosmesis
Current evidence advises mesh for all defects >2 cm and even for smaller defects, due to high recurrence rates with tissue-only repair.
Laparoscopic Umbilical Hernia Repair
- A camera port and two working ports are placed laterally on the abdominal wall, well away from the defect
- Contents are reduced by traction and external pressure
- The falciform ligament above and median umbilical fold below may need to be taken down to create a smooth surface for mesh placement
- A disc of non-adherent (antiadhesive-coated) mesh designed for intraperitoneal use is introduced and centred on the defect
- Fixed to the peritoneum and posterior rectus sheaths using staples, tacks, or sutures
Advantages: Fewer wound complications, permits large mesh pieces, preferred in obese patients, those with concomitant rectus divarication, and those with multiple ventral defects.
Disadvantages: Requires specialised equipment; expensive intraperitoneal mesh; risks include bowel adhesion, erosion, fistulation, and severe pain (mimicking peritonitis) for 24-48 hours.
Mesh Placement Options (Open)
- Onlay position - on top of the fascia (creates large subcutaneous flaps, higher SSI risk)
- Preperitoneal position - dissection into preperitoneal plane, 3-5 cm overlap circumferentially; no fixation sutures needed (intra-abdominal pressure holds mesh); flat polypropylene sheet suitable
- Intraperitoneal position - requires mesh with antiadhesive barrier; useful when peritoneum tears easily
Special Circumstances
- Pregnancy-related hernias: Advise weight loss and abdominal exercise first; avoid surgery before or during pregnancy
- Liver cirrhosis (Child's B/C): Very high perioperative mortality; if surgery is needed, use fine continuous sutures to minimise post-operative ascites leakage; mesh is relatively contraindicated
Emergency Repair of Umbilical Hernia
- Incarceration/strangulation frequent due to narrow fibrous neck
- Most performed open
- In established strangulation: avoid mesh (infection risk too high); perform suture repair; definitive mesh repair at a later date if necessary
- Multiloculated hernias may have strangulated bowel in one component while other areas appear soft
2. Epigastric Hernia (Hernia of the Linea Alba)
Anatomy and Pathology
Epigastric hernias arise through the midline raphe (linea alba) anywhere between the xiphoid process and the umbilicus. The defect begins as a transverse split, producing an elliptical opening usually <1 cm in diameter. Contents are typically extraperitoneal fat that gradually enlarges in a mushroom shape in the subcutaneous plane. Rarely, a peritoneal sac forms, and bowel involvement is uncommon.
More than one hernia may coexist - the most common cause of apparent "recurrence" is failure to identify a second defect at original repair.
Clinical Features
- Typically in fit, healthy men, or older overweight individuals, postmenopausal women
- Can be very painful despite small size - fatty contents become "nipped," causing partial strangulation
- Often locally tender; may not be reducible
- May resemble a lipoma; cough impulse variable
Treatment
- Very small hernias may disappear spontaneously (infarction of the fat)
- Small-to-moderate hernias without a peritoneal sac: repair only if sufficiently symptomatic
- Hernias containing bowel: always repair
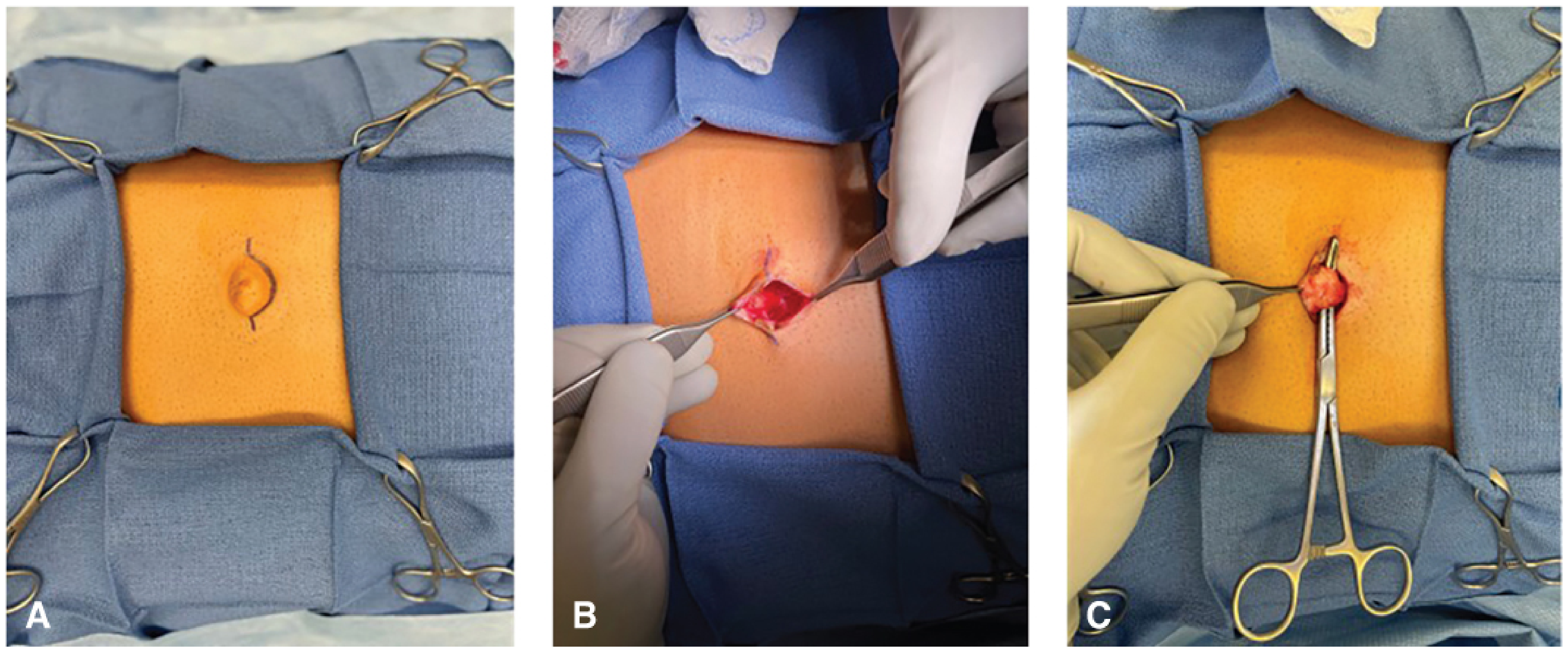
Surgery - Open
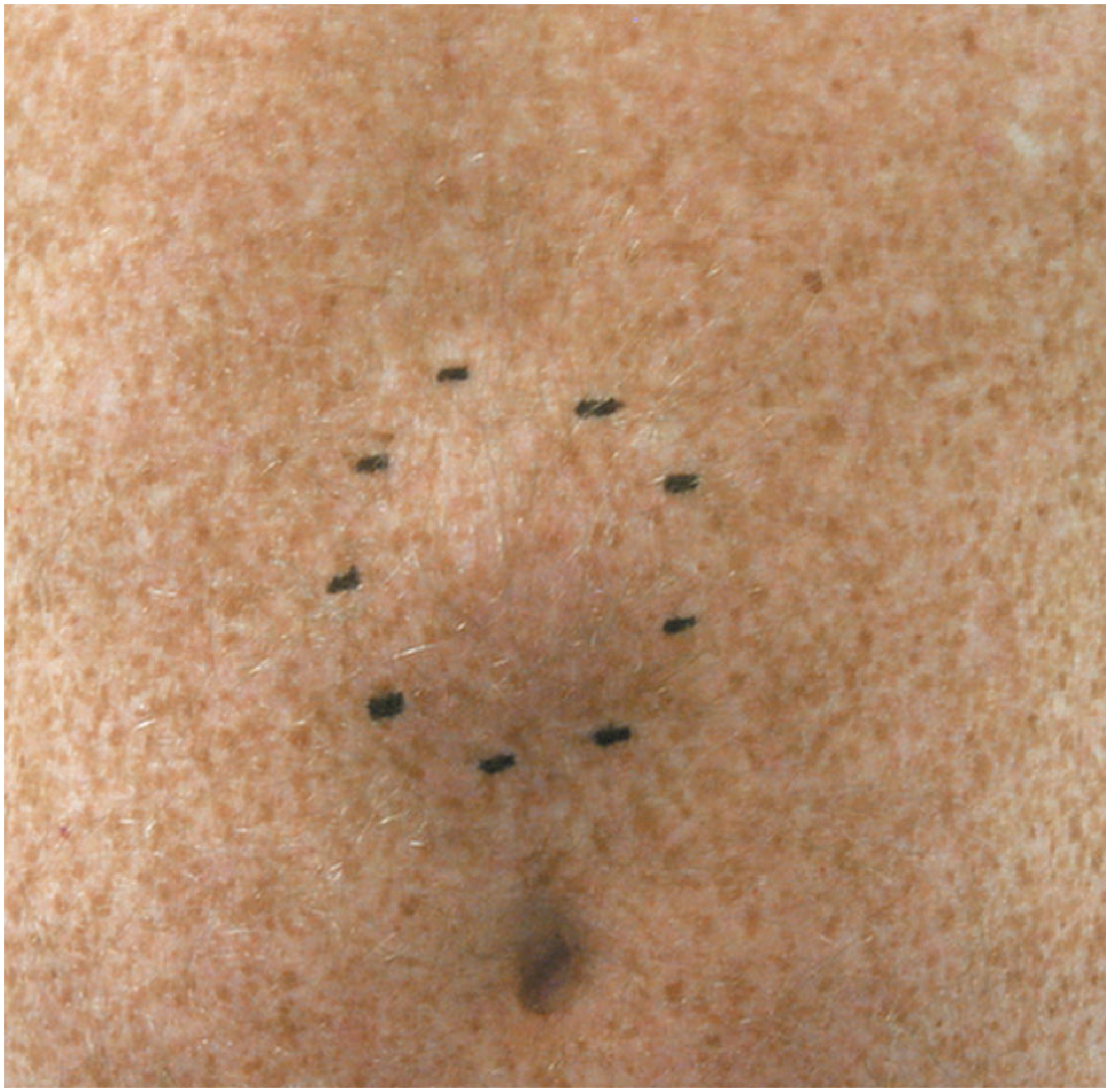
- Vertical or transverse incision directly over the swelling, down to the linea alba
- Protruding extraperitoneal fat is pushed back through the defect or excised (beware a small vessel in the hernia contents causing troublesome bleeding)
- Small defects (<2 cm): Closed with non-absorbable sutures (adults) or absorbable sutures (children)
- Larger defects / peritoneal sac present: Surgical approach identical to umbilical mesh repair
- Mesh recommended for defects >2 cm; can be placed in onlay, preperitoneal, or intraperitoneal position (same principles as umbilical mesh repair)
From Fischer's Mastery: The fascia is cleared circumferentially for 1-2 cm and reapproximated in interrupted fashion with slowly absorbable or permanent suture.
Surgery - Laparoscopic
- Very similar to laparoscopic umbilical hernia repair
- The defect is hidden behind the falciform ligament, which must first be taken down from the undersurface of the abdominal wall
- It is critical to fully reduce the fatty contents - simply placing mesh under the linea alba will leave a palpable lump if extraperitoneal fat is not reduced
3. Spigelian Hernia
Anatomy and Pathology
Spigelian hernias are uncommon but probably underdiagnosed. They affect men and women equally and are most common in the elderly; rare cases have been described in infants (incomplete mesenchymal differentiation).
The hernia arises through a defect in the aponeurosis of transversus abdominis (Spigelian fascia) at the lateral border of the rectus sheath. It may then advance through the internal oblique to spread out deep to the external oblique aponeurosis - an interstitial hernia. Most appear below the level of the umbilicus near the edge of the rectus sheath, but may occur anywhere along the Spigelian line.
Important note: A common misconception is that they protrude below the arcuate line due to deficiency of the posterior rectus sheath - in fact, the defect is almost always above the arcuate line.
Clinical Features
| Patient Group | Presentation |
|---|---|
| Young patients | Intermittent pain from fat-pinching; no visible lump (external oblique intact); similar to epigastric hernia |
| Older patients | Reducible swelling at the edge of rectus sheath; symptoms of intermittent obstruction |
Diagnosis: CT confirms the diagnosis. Ultrasound is advantageous as it can be performed with the patient upright - no defect may be visible when the patient is lying down.
Treatment
Surgery is recommended in all cases because the narrow, fibrous neck predisposes to strangulation (high risk of complications).
Open Repair
- A skin crease incision is made over the hernia
- No abnormality is visible until the external oblique aponeurosis is opened
- The sac and contents are reduced and dealt with
- The small defect in the Spigelian fascia is repaired by suture or mesh placed deep to the external oblique aponeurosis
- The plane of mesh can be extended medially into the posterior rectus sheath if required
- The external oblique aponeurosis is closed over the mesh
Laparoscopic Repair
- Useful when no sac is palpable
- In young patients with only extraperitoneal fat: no hernia will be seen from within the peritoneum; the peritoneum can be incised to explore the extraperitoneal plane, with the small defect closed by suture or mesh
- When an intraperitoneal sac is present: two main options:
- IPOM (intraperitoneal onlay mesh) - being used less frequently due to intraperitoneal mesh risks
- TAPP (transabdominal preperitoneal) - now more commonly preferred
Summary Comparison
| Feature | Umbilical | Epigastric (Linea Alba) | Spigelian |
|---|---|---|---|
| Location | Through umbilical ring | Linea alba, xiphoid to umbilicus | Lateral rectus border (Spigelian fascia) |
| Contents | Fat, omentum, bowel | Mainly extraperitoneal fat | Fat (young), peritoneal sac (elderly) |
| Defect size | Variable | Usually <1 cm | Small, fibrous neck |
| Strangulation risk | High (narrow neck) | Low-moderate | High (narrow fibrous neck) |
| Diagnosis | Clinical | Clinical | CT or upright ultrasound |
| Suture repair | Defects <2 cm (Mayo for 1-2 cm) | Defects <2 cm | Primary closure for small defects |
| Mesh | Defects >2 cm; all adults ideally | Defects >2 cm / sac present | Routinely placed deep to ext. oblique |
| Laparoscopic option | Yes (IPOM) | Yes (IPOM) | Yes (TAPP preferred) |
| Emergency mesh | Avoid if strangulation present | Avoid if strangulation | Avoid if strangulation |
Sources: Bailey and Love's Short Practice of Surgery, 28th Edition, pp. 1094-1097; Fischer's Mastery of Surgery, 8th Edition, pp. 5906-5911
This is a shared conversation. Sign in to Orris to start your own chat.