Diagnosis management and prescription for a patient with carpal tunnel syndrome. Must include the background like metabolic disease or long-term compression over flexor retinaculum!
Reading File
Finding Sources
Finding Sources
Searching PubMed
"carpal tunnel syndrome"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compose the full clinical response.
Carpal Tunnel Syndrome (CTS): Background, Diagnosis, Management & Prescription
1. Background and Anatomy
The carpal tunnel is a rigid osseofibrous channel at the wrist bounded by the carpal bones (forming the floor and sides) and the flexor retinaculum (transverse carpal ligament, TCL) forming the palmar "roof." Passing through this tunnel are the median nerve (the most palmar structure) and nine flexor tendons (FDS x4, FDP x4, FPL x1).
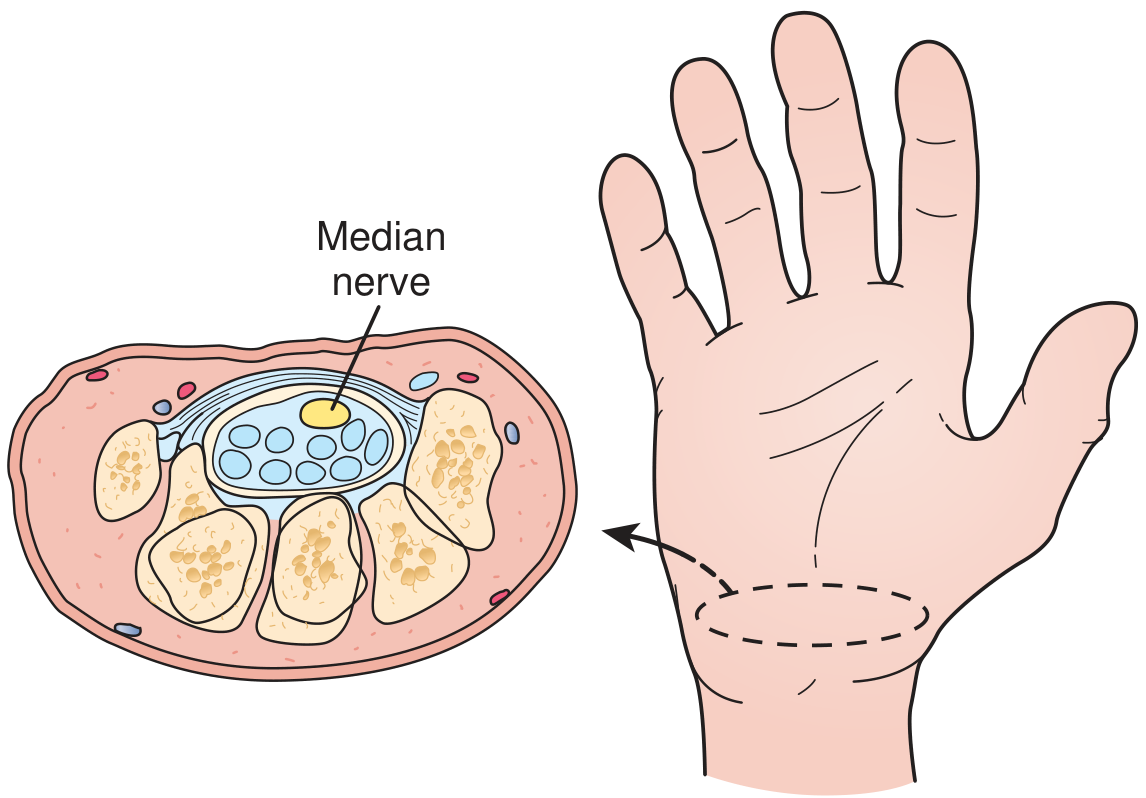
Cross-section of the carpal tunnel. Nine flexor tendons and the median nerve pass through the tunnel, which is bounded on three sides by carpal bones and volarly by the transverse carpal ligament. - Textbook of Family Medicine 9e, p. 821
CTS is the most common compressive mononeuropathy, affecting up to 10% of the U.S. population, twice as common in women, and most prevalent in those aged 30-60 years. Carpal tunnel pressure above 20-30 mmHg impedes epineurial blood flow and impairs nerve function. - Campbell's Operative Orthopaedics 15e
2. Etiological Background (Metabolic & Mechanical)
Causes fall into several overlapping categories. The etiology is idiopathic in most cases, but the following systemic and mechanical factors are well established:
A. Metabolic / Systemic Disease
| Category | Conditions |
|---|---|
| Fluid balance / hormonal | Hypothyroidism, pregnancy, menopause, eclampsia, renal failure, long-term hemodialysis |
| Neuropathic | Diabetes mellitus (peripheral neuropathy), alcoholism, double-crush syndrome |
| Inflammatory | Rheumatoid arthritis, gout, nonspecific tenosynovitis, infection |
| Autoimmune / infiltrative | Amyloidosis (infiltration of the TCL), lupus erythematosus, scleroderma, multiple sclerosis, Paget disease |
| Endocrine/structural | Acromegaly (bony overgrowth narrows tunnel), lysosomal storage disease |
Key point: Bradley and Daroff's Neurology states that pregnancy, diabetes, rheumatoid arthritis, hypothyroidism, sarcoidosis, acromegaly, and amyloid infiltration should be screened with blood studies in ALL newly diagnosed CTS patients. - Bradley and Daroff's Neurology in Clinical Practice, p. 549
B. Long-term Compression / Mechanical Factors (Over the Flexor Retinaculum)
- Repetitive forceful wrist and finger flexion/extension - occupational or hobby-related (e.g., assembly line workers, typists, musicians)
- Habitual sleeping with wrist in acute flexion - sustained wrist posture chronically compresses the tunnel
- Direct pressure on the carpal tunnel (e.g., handlebar pressure, vibratory tool use)
- Wrist fractures (Colles fracture, scaphoid fracture) or dislocations (lunate volar dislocation) increasing tunnel contents
- Space-occupying lesions: ganglion cysts, lipomas, hypertrophic synovium, hematoma
- Stenosing flexor tenosynovitis thickening the tendon sheaths within the tunnel
- Campbell's Operative Orthopaedics 15e, Box 82.1
3. Clinical Presentation
Symptoms
- Paresthesia and numbness in the palmar surface of the thumb, index, long, and radial half of the ring finger (median nerve sensory distribution)
- Symptoms typically worse at night and may wake the patient - relieved by "flick" maneuver (shaking/elevating the hand)
- Diffuse deep aching or throbbing pain radiating up the forearm (may misleadingly extend to shoulder)
- Thenar muscle atrophy and weakness of thumb opposition/abduction (APB, opponens pollicis) in advanced disease
- Note: the palmar cutaneous branch leaves the median nerve proximal to the TCL, so thenar skin sensation is often preserved despite CTS - a useful diagnostic clue
Physical Examination Findings
| Finding | Notes |
|---|---|
| Tinel's sign | Tap over wrist flexor retinaculum → electric tingling into the median nerve distribution. Most specific but least sensitive |
| Phalen's maneuver | Sustained wrist flexion x60 sec → numbness/paresthesia. Most sensitive (74%), false-positive ~25% |
| Durkan (Carpal Compression) test | Direct compression over TCL x30 sec. Most diagnostically useful: sensitivity 87%, specificity 90% - more accurate than Tinel or Phalen |
| Thenar atrophy | APB wasting in advanced/chronic cases |
| Two-point discrimination >5 mm | Indicates significant sensory fiber loss |
4. Diagnostic Scoring: CTS-6
| Finding | Points |
|---|---|
| Numbness predominantly in median nerve distribution | 3.5 |
| Nocturnal symptoms | 4.0 |
| Thenar atrophy or weakness | 5.0 |
| Positive Phalen test | 5.0 |
| Loss of two-point discrimination (>5 mm) | 4.5 |
| Positive Tinel sign | 4.0 |
Score ≥12: Sensitivity 95%, Specificity 91% - equivalent to EMG/NCS but without the cost or discomfort. - Campbell's Operative Orthopaedics 15e, Table 82.1
5. Investigations
Electrodiagnostic Studies (EMG/NCS) - Gold Standard for Confirmation
- Distal motor latency >4.5 ms - abnormal
- Sensory latency >3.5 ms - abnormal
- EMG: increased insertional activity, fibrillations at rest, decreased motor recruitment in APB
- 90% sensitive, 60% specific. May be normal in symptomatic patients (up to 25% false negative)
- Indicated before surgical intervention
Ultrasound
- Cross-sectional area (CSA) of median nerve >10 mm² at the pisiform level is diagnostic
- High-resolution US: sensitivity 73% using cutoff of 9.4 mm² at carpal tunnel inlet
- Useful when NCS is equivocal; increasingly preferred as first-line imaging
MRI
- NOT routinely recommended for CTS diagnosis
- Reserved for rare cases with suspected mass lesions or structural abnormality
Blood Work (Workup for Underlying Cause)
Order in all newly diagnosed patients:
- TSH (hypothyroidism)
- Fasting glucose / HbA1c (diabetes mellitus)
- Renal function panel (CKD, dialysis-related)
- Rheumatoid factor / anti-CCP (rheumatoid arthritis)
- Serum protein electrophoresis / urine protein (amyloidosis / multiple myeloma)
- IGF-1 / GH if acromegaly suspected
- Pregnancy test if appropriate
6. Management
Predictors of Nonoperative Treatment Failure (Box 82.3)
If ≥3 of these are present, conservative therapy is likely to fail:
- Age >50 years
- Duration >10 months
- Constant (not intermittent) paresthesia
- Stenosing flexor tenosynovitis
- Positive Phalen test in <30 seconds
Step 1: Conservative (First-Line, Mild-Moderate Symptoms)
Activity Modification
- Identify and minimize repetitive wrist flexion/extension at work or home
- Ergonomic workplace assessment - wrist support pads, keyboard height
- Avoid habitual sleeping with wrist in flexion
Wrist Splinting
- Neutral wrist splint (0° extension), worn especially at night
- Effective for relieving nocturnal symptoms; most benefit in mild-to-moderate CTS
- Can also be worn during provoking activities
Nerve Gliding Exercises
- Routinely prescribed; evidence supports symptom relief when combined with splinting
Step 2: Pharmacological Management
Corticosteroid Injection (into the carpal tunnel)
- Methylprednisolone (or triamcinolone) injected into the carpal tunnel
- Provides reliable short-term symptom relief; useful as diagnostic tool (90% who get temporary relief respond to surgery)
- Long-term benefit in only ~10% of patients
- CAUTION: Inject palmar/ulnar to the palmaris longus tendon - never directly into the nerve
Oral Corticosteroids
- Short course oral prednisolone: evidence for short-term benefit
- Not a long-term solution
NSAIDs / Analgesics
- Evidence shows NSAIDs are no more effective than placebo for CTS symptom relief
- May be used for associated tenosynovitis or background inflammatory arthritis
Diuretics
- May provide short-term benefit in fluid-overload states (pregnancy, renal failure)
Step 3: Surgical Management (Moderate-Severe, or Failed Conservative)
Carpal Tunnel Release (CTR) - division of the flexor retinaculum (TCL) to decompress the median nerve. Excellent long-term outcomes.
Two Main Techniques
| Technique | Notes |
|---|---|
| Open CTR (standard or mini-palm) | Longitudinal incision just ulnar to midline of ring finger, 2-3 cm from distal wrist crease. Direct visualization ensures nerve safety. Most widely practiced |
| Endoscopic CTR | 1-2 small portal incisions; faster return to work, less scar tenderness. Meta-analysis (PMID 38768022) shows equivalent long-term outcomes vs. open; endoscopic generally preferred per Goldman-Cecil |
Surgical indications:
- Failure of conservative therapy after adequate trial (typically 3-6 months)
- Significant thenar atrophy or progressive motor weakness
- Severe or constant paresthesia (high CTS-6, prolonged NCS latencies)
Caution in elderly (>70 years) and advanced nerve compression: surgical release may not achieve complete symptom relief; thenar atrophy resolves slowly if at all.
Treatment Algorithm (from Campbell's Operative Orthopaedics 15e)
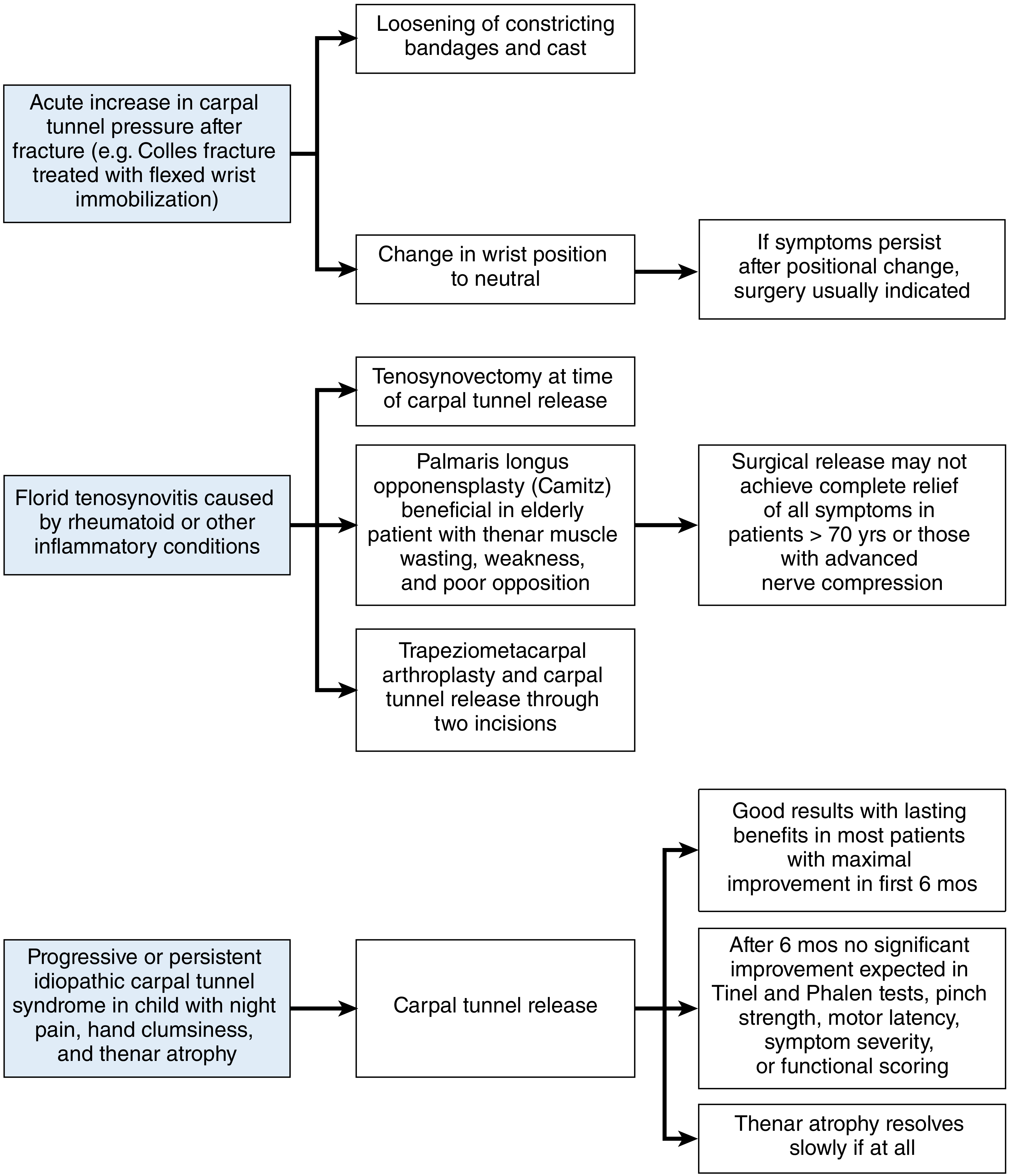
Treatment algorithm for CTS based on etiology. Acute post-fracture CTS warrants cast loosening and positional change; florid tenosynovitis (RA) often needs concurrent tenosynovectomy; idiopathic progressive CTS proceeds to carpal tunnel release. - Campbell's Operative Orthopaedics 15e, Figure 82.1
7. Prescription Summary
CONSERVATIVE PHASE:
1. Neutral wrist splint – wear nightly; can use during provoking activities
2. Nerve gliding exercises – daily programme, refer to hand therapist
3. Ergonomic assessment – workplace wrist positioning
INJECTION (moderate symptoms or diagnostic):
4. Methylprednisolone acetate 40 mg (1 mL) + 1% lidocaine 1 mL
→ Ultrasound-guided injection into carpal tunnel (palmar-ulnar to palmaris longus)
→ May repeat once if partial relief; limit to 2-3 total injections
PHARMACOLOGICAL ADJUNCTS:
5. Prednisolone 20 mg oral once daily x10-14 days (for acute flares)
[NSAIDs – not recommended; no better than placebo for CTS]
6. Treat underlying cause:
- Hypothyroidism → Levothyroxine titrated to TSH 0.5-2.0 mIU/L
- Diabetes → Optimize glycemic control (HbA1c <7%)
- RA → DMARDs per rheumatology; consider concurrent tenosynovectomy if surgery needed
- Renal failure / dialysis amyloidosis → dialysis optimization; early surgery referral
SURGICAL REFERRAL (if ≥3 failure predictors, or progressive motor signs):
7. Carpal tunnel release – endoscopic or open mini-palm technique
(preoperative NCS mandatory)
8. Special Situations
| Scenario | Management |
|---|---|
| Pregnancy | Splinting + local injection; usually resolves post-delivery |
| Hypothyroid CTS | Thyroid replacement first - may resolve CTS without surgery |
| Diabetic CTS | NCS may underestimate severity; surgical outcome still good |
| Dialysis / amyloid CTS | Early CTR recommended; do not delay - amyloid rarely responds to conservative care |
| Post-Colles fracture CTS | Loosen cast, change wrist position to neutral; if persists → urgent surgery |
| RA with tenosynovitis | CTR + concurrent tenosynovectomy ± opponensplasty (elderly with thenar wasting) |
Recent Evidence
- Global CTS prevalence meta-analysis (PMID 39672798) - 2024 Systematic Review confirming CTS as highly prevalent globally, supporting proactive screening.
- Endoscopic vs. open CTR umbrella review (PMID 38768022) - 2024 meta-analysis confirms endoscopic approach is generally preferred with faster recovery.
- Ultrasound-guided nerve hydrodissection meta-analysis (PMID 39894044) - 2025 network meta-analysis supports hydrodissection as a nonsurgical option in selected patients.
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Goldman-Cecil Medicine International Edition; Bradley and Daroff's Neurology in Clinical Practice; Textbook of Family Medicine 9e; Tintinalli's Emergency Medicine
Generate a prescription template (PDF) for CTS management by severity level
Reading File
Running Command
ls -la /home/daytona/workspace/ 2>/dev/null && mkdir -p /home/daytona/workspace/…
Writing File
~/cts-prescription/generate_cts_rx.py
"""
CTS Prescription Template PDF Generator
Uses reportlab for professional clinical layout
"""
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import mm, cm
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether
)
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_RIGHT, TA_JUSTIFY
from reportlab.platypus import PageBreak
from reportlab.lib.colors import HexColor
import os
OUTPUT_PATH = "/home/daytona/workspace/cts-prescription/CTS_Prescription_Template.pdf"
# ── Colour palette ──────────────────────────────────────────────────────────
C_DARK_BLUE = HexColor("#1a3a5c") # header, section titles
C_MED_BLUE = HexColor("#2e6da4") # sub-headers, accents
C_MILD_GREEN = HexColor("#e8f5e9") # mild severity bg
C_MOD_YELLOW = HexColor("#fffde7") # moderate severity bg
C_SEV_RED = HexColor("#fce4ec") # severe severity bg
C_LIGHT_GRAY = HexColor("#f5f7fa") # alternating row
C_MID_GRAY = HexColor("#90a4ae") # secondary text
C_WHITE = colors.white
C_BLACK = colors.black
C_BORDER = HexColor("#b0bec5")
# ── Build document ───────────────────────────────────────────────────────────
doc = SimpleDocTemplate(
OUTPUT_PATH,
pagesize=A4,
rightMargin=18*mm, leftMargin=18*mm,
topMargin=14*mm, bottomMargin=18*mm,
title="Carpal Tunnel Syndrome – Prescription Template",
author="Orris Medical AI"
)
W = A4[0] - 36*mm # usable width
styles = getSampleStyleSheet()
# Custom paragraph styles
def make_style(name, parent="Normal", **kw):
return ParagraphStyle(name, parent=styles[parent], **kw)
hdr_title = make_style("HdrTitle", fontSize=17, textColor=C_WHITE,
fontName="Helvetica-Bold", leading=22, alignment=TA_CENTER)
hdr_sub = make_style("HdrSub", fontSize=9, textColor=HexColor("#cfe4ff"),
fontName="Helvetica", leading=13, alignment=TA_CENTER)
sec_title = make_style("SecTitle", fontSize=11, textColor=C_WHITE,
fontName="Helvetica-Bold", leading=15, alignment=TA_LEFT,
leftIndent=4)
sev_label = make_style("SevLabel", fontSize=10, textColor=C_DARK_BLUE,
fontName="Helvetica-Bold", leading=14)
body = make_style("Body", fontSize=8.5, leading=13, textColor=C_BLACK)
body_bold = make_style("BodyBold", fontSize=8.5, leading=13,
textColor=C_DARK_BLUE, fontName="Helvetica-Bold")
small = make_style("Small", fontSize=7.5, leading=11, textColor=HexColor("#546e7a"))
rx_item = make_style("RxItem", fontSize=8.5, leading=13,
leftIndent=8, firstLineIndent=-8)
note_style = make_style("Note", fontSize=7.8, leading=11.5,
textColor=HexColor("#37474f"), fontName="Helvetica-Oblique")
footer_s = make_style("Footer", fontSize=7, textColor=C_MID_GRAY,
alignment=TA_CENTER)
# ── Helper: coloured section banner ─────────────────────────────────────────
def section_banner(text, bg=C_DARK_BLUE, width=None):
w = width or W
return Table(
[[Paragraph(text, sec_title)]],
colWidths=[w],
style=TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 8),
])
)
def severity_banner(text, bg, text_color=C_DARK_BLUE):
st = make_style(f"SevBan_{text}", fontSize=11, textColor=text_color,
fontName="Helvetica-Bold", leading=16, alignment=TA_LEFT)
return Table(
[[Paragraph(text, st)]],
colWidths=[W],
style=TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 10),
("BOX", (0,0), (-1,-1), 0.8, C_BORDER),
])
)
def rx_table(rows, col_widths=None):
"""Render a 2-column key/value table for prescriptions."""
cw = col_widths or [50*mm, W - 50*mm]
data = []
for label, val, color in rows:
data.append([
Paragraph(f"<b>{label}</b>", body_bold),
Paragraph(val, body)
])
style = TableStyle([
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 6),
("RIGHTPADDING", (0,0), (-1,-1), 6),
("GRID", (0,0), (-1,-1), 0.4, C_BORDER),
])
# Alternating row backgrounds
for i, (_, _, c) in enumerate(rows):
bg = c if c else (C_LIGHT_GRAY if i % 2 == 0 else C_WHITE)
style.add("BACKGROUND", (0, i), (-1, i), bg)
return Table(data, colWidths=cw, style=style, hAlign="LEFT")
def drug_box(lines, bg=C_WHITE):
"""A bordered box listing drug entries."""
rows = [[Paragraph(l, body)] for l in lines]
t = Table(rows, colWidths=[W],
style=TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("BOX", (0,0), (-1,-1), 0.8, C_MED_BLUE),
("INNERGRID", (0,0), (-1,-1), 0.3, C_BORDER),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 10),
])
)
return t
# ═══════════════════════════════════════════════════════════════════════════════
# CONTENT
# ═══════════════════════════════════════════════════════════════════════════════
story = []
# ── HEADER ───────────────────────────────────────────────────────────────────
header_data = [[
Paragraph("CARPAL TUNNEL SYNDROME", hdr_title),
],[
Paragraph("Clinical Prescription Template · Stratified by Severity Level", hdr_sub),
]]
header = Table(header_data, colWidths=[W],
style=TableStyle([
("BACKGROUND", (0,0), (-1,-1), C_DARK_BLUE),
("TOPPADDING", (0,0), (0,0), 10),
("BOTTOMPADDING", (0,1), (0,1), 10),
("LEFTPADDING", (0,0), (-1,-1), 6),
("BOX", (0,0), (-1,-1), 1.5, C_MED_BLUE),
])
)
story.append(header)
story.append(Spacer(1, 4*mm))
# ── PATIENT DETAILS BOX ──────────────────────────────────────────────────────
story.append(section_banner("▸ PATIENT & CLINICIAN DETAILS"))
story.append(Spacer(1, 1*mm))
pt_fields = [
["Patient Name:", "_______________________________", "Date:", "____________"],
["Age / Sex:", "____________ / ____________", "MRN/ID:", "____________"],
["Clinician:", "_______________________________", "Signature:", "____________"],
["Facility:", "_______________________________", "Stamp:", ""],
]
pt_tbl = Table(pt_fields,
colWidths=[28*mm, 60*mm, 22*mm, 60*mm],
style=TableStyle([
("FONTNAME", (0,0), (-1,-1), "Helvetica"),
("FONTNAME", (0,0), (0,-1), "Helvetica-Bold"), # labels bold
("FONTNAME", (2,0), (2,-1), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,-1), 8.5),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 4),
("GRID", (0,0), (-1,-1), 0.4, C_BORDER),
("BACKGROUND", (0,0), (-1,-1), C_LIGHT_GRAY),
])
)
story.append(pt_tbl)
story.append(Spacer(1, 3*mm))
# ── ASSESSMENT SECTION ───────────────────────────────────────────────────────
story.append(section_banner("▸ CLINICAL ASSESSMENT"))
story.append(Spacer(1, 1*mm))
assess_rows = [
("Dominant Hand", "Right / Left / Bilateral", None),
("CTS-6 Score", "_______ /26 (≥12 = high probability CTS)", None),
("Phalen Test", "Positive / Negative — onset at ______ seconds", None),
("Tinel Sign", "Positive / Negative", None),
("Durkan Test", "Positive / Negative", None),
("Thenar Atrophy", "None / Mild / Moderate / Severe", None),
("2-Point Discrimination", "_____ mm (>5 mm = abnormal)", None),
("Symptom Duration", "_______ months", None),
("Symptom Pattern", "Intermittent / Constant", None),
("NCS / EMG", "Not done / Pending / Done: DML _____ ms, Sensory latency _____ ms", None),
("Ultrasound CSA", "Not done / Done: _____ mm² at pisiform level", None),
("Underlying Cause", "Idiopathic / DM / Hypothyroid / RA / Pregnancy / Amyloid / CKD / Other: _________", None),
]
story.append(rx_table(assess_rows, col_widths=[55*mm, W-55*mm]))
story.append(Spacer(1, 3*mm))
# ── SEVERITY CLASSIFICATION ──────────────────────────────────────────────────
story.append(section_banner("▸ SEVERITY CLASSIFICATION"))
story.append(Spacer(1, 1*mm))
sev_data = [
[Paragraph("<b>Severity</b>", body_bold),
Paragraph("<b>Clinical Features</b>", body_bold),
Paragraph("<b>NCS Findings</b>", body_bold),
Paragraph("<b>Circled Level</b>", body_bold)],
[Paragraph("<b>MILD</b>", make_style("M", fontSize=8.5, textColor=HexColor("#2e7d32"), fontName="Helvetica-Bold")),
Paragraph("Intermittent paresthesia, no atrophy, nocturnal symptoms only, normal grip strength", body),
Paragraph("Mildly prolonged sensory latency; normal or borderline motor latency", body),
Paragraph("MILD", make_style("M2", fontSize=9, alignment=TA_CENTER, fontName="Helvetica-Bold", textColor=HexColor("#2e7d32")))],
[Paragraph("<b>MODERATE</b>", make_style("Mo", fontSize=8.5, textColor=HexColor("#e65100"), fontName="Helvetica-Bold")),
Paragraph("Frequent paresthesia, daytime symptoms, mild thenar weakness, positive Phalen <30 s", body),
Paragraph("Prolonged DML (>4.5 ms) and/or sensory latency (>3.5 ms)", body),
Paragraph("MODERATE", make_style("Mo2", fontSize=9, alignment=TA_CENTER, fontName="Helvetica-Bold", textColor=HexColor("#e65100")))],
[Paragraph("<b>SEVERE</b>", make_style("S", fontSize=8.5, textColor=HexColor("#b71c1c"), fontName="Helvetica-Bold")),
Paragraph("Constant paresthesia, thenar atrophy, objective sensory loss, grip weakness, symptoms >10 months", body),
Paragraph("Markedly prolonged latencies; fibrillations / positive waves in APB on EMG", body),
Paragraph("SEVERE", make_style("S2", fontSize=9, alignment=TA_CENTER, fontName="Helvetica-Bold", textColor=HexColor("#b71c1c")))],
]
sev_tbl = Table(sev_data, colWidths=[24*mm, 70*mm, 54*mm, 22*mm],
style=TableStyle([
("BACKGROUND", (0,0), (-1,0), C_DARK_BLUE),
("TEXTCOLOR", (0,0), (-1,0), C_WHITE),
("BACKGROUND", (0,1), (-1,1), C_MILD_GREEN),
("BACKGROUND", (0,2), (-1,2), C_MOD_YELLOW),
("BACKGROUND", (0,3), (-1,3), C_SEV_RED),
("GRID", (0,0), (-1,-1), 0.5, C_BORDER),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 6),
("ALIGN", (3,0), (3,-1), "CENTER"),
("BOX", (3,1), (3,1), 1.5, HexColor("#2e7d32")),
("BOX", (3,2), (3,2), 1.5, HexColor("#e65100")),
("BOX", (3,3), (3,3), 1.5, HexColor("#b71c1c")),
])
)
story.append(sev_tbl)
story.append(Spacer(1, 4*mm))
# ══════════════════════════════════════════════════════════════════════════════
# PAGE 2 START — Prescription by severity
# ══════════════════════════════════════════════════════════════════════════════
story.append(PageBreak())
# ── PAGE 2 MINI HEADER ───────────────────────────────────────────────────────
mini_hdr = Table([[Paragraph("CTS PRESCRIPTION — BY SEVERITY LEVEL",
make_style("MH", fontSize=12, fontName="Helvetica-Bold", textColor=C_WHITE, alignment=TA_CENTER))]],
colWidths=[W],
style=TableStyle([
("BACKGROUND", (0,0), (-1,-1), C_DARK_BLUE),
("TOPPADDING", (0,0), (-1,-1), 7),
("BOTTOMPADDING", (0,0), (-1,-1), 7),
])
)
story.append(mini_hdr)
story.append(Spacer(1, 3*mm))
# ────────────────────────────────────────────────────────────────────────────
# MILD CTS
# ────────────────────────────────────────────────────────────────────────────
story.append(KeepTogether([
severity_banner("🟢 MILD CTS — Intermittent symptoms, no motor deficit", C_MILD_GREEN),
Spacer(1, 2*mm),
section_banner("Non-Pharmacological", bg=HexColor("#43a047"), width=W),
]))
story.append(Spacer(1, 1*mm))
mild_nonpharm = [
("<b>1.</b> Neutral wrist splint",
"Wear nightly (6–8 h). May also wear during provoking activities. "
"Splint should hold wrist at 0° (neutral), not extended or flexed.", None),
("<b>2.</b> Activity modification",
"Avoid sustained wrist flexion/extension. Ergonomic review of keyboard/workstation. "
"Wrist rests during typing. Reduce vibratory tool use.", None),
("<b>3.</b> Nerve gliding exercises",
"Daily programme × 10 repetitions each. Refer to hand therapist if available. "
"Tendon gliding + median nerve mobilisation sequence.", None),
]
story.append(rx_table(mild_nonpharm, col_widths=[40*mm, W-40*mm]))
story.append(Spacer(1, 2*mm))
story.append(section_banner("Pharmacological", bg=HexColor("#43a047"), width=W))
story.append(Spacer(1, 1*mm))
mild_pharm_lines = [
"💊 <b>Rx 1 — Corticosteroid Injection</b> (first-line if splinting fails at 4–6 weeks)",
" Drug: Methylprednisolone acetate 40 mg (1 mL) + 1% Lidocaine HCl 1 mL",
" Route: Intracarpal (palmar approach, ulnar to palmaris longus tendon)",
" Technique: Ultrasound-guided preferred; needle directed distally at 30–45° angle",
" Frequency: Single injection; may repeat once after 4–6 weeks if partial response",
" Max: 2–3 total injections — do NOT inject directly into the median nerve",
"",
"💊 <b>Rx 2 — Oral Prednisolone</b> (if injection declined or for acute flare)",
" Prednisolone 20 mg orally once daily × 10–14 days (taper not required for short course)",
" Take with food to reduce GI irritation",
"",
"⚠️ <b>NSAIDs:</b> Not recommended — evidence shows no benefit over placebo for CTS symptoms",
" (May be used adjunctively for coexisting tenosynovitis at clinician's discretion)",
]
story.append(drug_box(mild_pharm_lines, bg=HexColor("#f1f8e9")))
story.append(Spacer(1, 2*mm))
story.append(section_banner("Investigations / Workup for Underlying Cause", bg=HexColor("#43a047"), width=W))
story.append(Spacer(1, 1*mm))
mild_ix_lines = [
"□ TSH (hypothyroidism) □ Fasting glucose + HbA1c (diabetes)",
"□ Renal function / eGFR (CKD) □ RF / anti-CCP (rheumatoid arthritis)",
"□ Pregnancy test (if applicable) □ Consider ESR, CRP, ANA if autoimmune suspected",
]
story.append(drug_box(mild_ix_lines, bg=HexColor("#f1f8e9")))
story.append(Spacer(1, 2*mm))
story.append(Paragraph(
"📅 <b>Follow-up:</b> Review at 4–6 weeks. If no improvement with splint + injection → upgrade to moderate protocol.",
note_style))
story.append(Spacer(1, 4*mm))
# ────────────────────────────────────────────────────────────────────────────
# MODERATE CTS
# ────────────────────────────────────────────────────────────────────────────
story.append(KeepTogether([
severity_banner("🟡 MODERATE CTS — Frequent symptoms, mild motor signs", C_MOD_YELLOW),
Spacer(1, 2*mm),
section_banner("Non-Pharmacological", bg=HexColor("#f9a825"), width=W),
]))
story.append(Spacer(1, 1*mm))
mod_nonpharm = [
("<b>1.</b> Neutral wrist splint",
"Full-time splinting for 4–6 weeks (day + night), then reassess. "
"Removable thermoplastic splint preferred.", None),
("<b>2.</b> Workplace ergonomics",
"Formal occupational therapy referral. Workstation redesign, modified duties if required.", None),
("<b>3.</b> Nerve gliding exercises",
"Twice daily. Include tendon gliding, nerve mobilisation, and opposition strengthening.", None),
("<b>4.</b> Treat underlying cause",
"Optimise thyroid replacement, glycaemic control, RA disease-modifying therapy, "
"or diuresis (pregnancy/renal).", None),
]
story.append(rx_table(mod_nonpharm, col_widths=[40*mm, W-40*mm]))
story.append(Spacer(1, 2*mm))
story.append(section_banner("Pharmacological", bg=HexColor("#f9a825"), width=W))
story.append(Spacer(1, 1*mm))
mod_pharm_lines = [
"💊 <b>Rx 1 — Corticosteroid Injection (First-line)</b>",
" Methylprednisolone acetate 40 mg + 1% Lidocaine 1 mL — intracarpal, as above",
" If 90% improvement → continues conservative; if partial → plan surgical referral",
"",
"💊 <b>Rx 2 — Oral Prednisolone (bridge or injection not feasible)</b>",
" Prednisolone 25 mg once daily × 14 days; reduce to 12.5 mg × 7 days, then stop",
"",
"💊 <b>Rx 3 — Treat underlying metabolic disease (examples):</b>",
" Hypothyroidism: Levothyroxine — start 25–50 mcg/day; titrate to TSH 0.5–2.0 mIU/L",
" Diabetes mellitus: Optimise HbA1c to <7%; add or adjust antidiabetic agent",
" Rheumatoid arthritis: Continue/escalate DMARDs per rheumatology; consider MTX ± biologic",
" Pregnancy: Neutral splint + single injection safe; most cases resolve post-partum",
" CKD / dialysis: Optimise dialysis adequacy; early surgical referral (amyloid-related CTS)",
"",
"💊 <b>Neuropathic pain adjunct</b> (if burning/dysaesthetic component prominent):",
" Gabapentin 100–300 mg at night; titrate cautiously. Or Amitriptyline 10 mg nocte.",
" Use with caution in elderly; monitor for sedation.",
]
story.append(drug_box(mod_pharm_lines, bg=HexColor("#fffde7")))
story.append(Spacer(1, 2*mm))
story.append(section_banner("Investigations", bg=HexColor("#f9a825"), width=W))
story.append(Spacer(1, 1*mm))
mod_ix_lines = [
"□ NCS / EMG — mandatory before surgical referral (DML, sensory latency, APB EMG)",
"□ Wrist ultrasound — median nerve CSA (cutoff >10 mm² at pisiform)",
"□ Blood: TSH, HbA1c, RF/anti-CCP, renal panel, FBC, SPEP if amyloid suspected",
"□ Wrist X-ray — if post-traumatic or arthropathy suspected",
]
story.append(drug_box(mod_ix_lines, bg=HexColor("#fffde7")))
story.append(Spacer(1, 2*mm))
story.append(Paragraph(
"📅 <b>Follow-up:</b> 4–6 weeks. If ≥3 failure predictors present (age >50, duration >10 months, "
"constant paresthesia, stenosing tenosynovitis, Phalen <30 s) → refer for surgery.",
note_style))
story.append(Spacer(1, 4*mm))
# ────────────────────────────────────────────────────────────────────────────
# SEVERE CTS (page 3)
# ────────────────────────────────────────────────────────────────────────────
story.append(PageBreak())
# Mini repeat header
story.append(mini_hdr)
story.append(Spacer(1, 3*mm))
story.append(KeepTogether([
severity_banner("🔴 SEVERE CTS — Constant symptoms, thenar atrophy, motor deficit", C_SEV_RED),
Spacer(1, 2*mm),
section_banner("Immediate Management", bg=HexColor("#c62828"), width=W),
]))
story.append(Spacer(1, 1*mm))
sev_immediate = [
("<b>URGENT surgical referral</b>",
"Refer to hand surgery / orthopaedic surgery for carpal tunnel release (CTR). "
"Thenar atrophy and motor weakness indicate irreversible nerve damage risk.", None),
("<b>Cease provoking activities</b>",
"Modified duties or temporary work cessation if occupation involves repetitive wrist use.", None),
("<b>Full-time neutral wrist splint</b>",
"Continue while awaiting surgery to limit further compression.", None),
("<b>Corticosteroid injection</b>",
"May provide temporary relief and confirms diagnosis (90% who respond will benefit from surgery). "
"Do NOT delay surgical referral awaiting injection response.", None),
]
story.append(rx_table(sev_immediate, col_widths=[45*mm, W-45*mm]))
story.append(Spacer(1, 2*mm))
story.append(section_banner("Surgical Options", bg=HexColor("#c62828"), width=W))
story.append(Spacer(1, 1*mm))
sev_surg_lines = [
"🔪 <b>Option 1 — Open Carpal Tunnel Release (standard / mini-palm)</b>",
" Longitudinal incision distal to wrist crease, ulnar to ring finger midline (~2–3 cm)",
" Division of flexor retinaculum (TCL) under direct vision; nerve safety confirmed before release",
" Preferred when anatomy uncertain, revision case, or concurrent tenosynovectomy needed",
"",
"🔪 <b>Option 2 — Endoscopic CTR (ECTR)</b>",
" 1–2 portal technique; faster return to function, less pillar pain",
" Equivalent long-term outcomes to open CTR (meta-analysis 2024, PMID 38768022)",
" Generally preferred when straightforward anatomy",
"",
"⚕️ <b>Special surgical considerations by underlying cause:</b>",
" RA / tenosynovitis: CTR + concurrent tenosynovectomy; if thenar atrophy + poor opposition",
" → Camitz palmaris longus opponensplasty (especially in elderly patients)",
" Post-Colles fracture: Loosen cast → change wrist to neutral; if persists → urgent CTR",
" Dialysis amyloid: Bilateral staged CTR; do not delay — amyloid does not respond conservatively",
" Age >70 / advanced compression: Counsel that thenar atrophy may not fully resolve post-CTR",
]
story.append(drug_box(sev_surg_lines, bg=HexColor("#ffebee")))
story.append(Spacer(1, 2*mm))
story.append(section_banner("Pre-operative Investigations", bg=HexColor("#c62828"), width=W))
story.append(Spacer(1, 1*mm))
sev_ix_lines = [
"□ NCS / EMG — mandatory (DML >4.5 ms, sensory latency >3.5 ms; fibrillations in APB on EMG)",
"□ Wrist ultrasound (median nerve CSA) if NCS equivocal",
"□ FBC, coagulation (INR/APTT), renal/liver function, blood glucose",
"□ Wrist X-ray (PA + lateral) — assess carpal anatomy, osteophytes, fracture deformity",
"□ MRI — only if space-occupying lesion (ganglion, lipoma, tumour) suspected",
"□ Anaesthetic review if indicated (comorbidities)",
]
story.append(drug_box(sev_ix_lines, bg=HexColor("#ffebee")))
story.append(Spacer(1, 2*mm))
story.append(Paragraph(
"📅 <b>Post-operative follow-up:</b> Wound review at 10–14 days. Maximum improvement expected within "
"first 6 months post-CTR. Sensory recovery precedes motor recovery. Physiotherapy for grip strengthening "
"and scar management. Thenar atrophy resolves slowly and may be incomplete.",
note_style))
story.append(Spacer(1, 4*mm))
# ────────────────────────────────────────────────────────────────────────────
# UNDERLYING CAUSE TREATMENT QUICK REFERENCE
# ────────────────────────────────────────────────────────────────────────────
story.append(section_banner("▸ TREATMENT OF UNDERLYING CAUSE — QUICK REFERENCE"))
story.append(Spacer(1, 1*mm))
cause_data = [
[Paragraph("<b>Condition</b>", body_bold),
Paragraph("<b>Target / Goal</b>", body_bold),
Paragraph("<b>First-line Treatment</b>", body_bold),
Paragraph("<b>Notes</b>", body_bold)],
[Paragraph("Hypothyroidism", body),
Paragraph("TSH 0.5–2.0 mIU/L", body),
Paragraph("Levothyroxine 25–100 mcg/day PO", body),
Paragraph("CTS may resolve with euthyroid state alone", small)],
[Paragraph("Diabetes mellitus", body),
Paragraph("HbA1c <7%", body),
Paragraph("Optimise antidiabetic regimen per guidelines", body),
Paragraph("NCS may underestimate severity; surgical outcome still favourable", small)],
[Paragraph("Rheumatoid arthritis", body),
Paragraph("DAS28 remission", body),
Paragraph("Methotrexate ± biologic DMARD", body),
Paragraph("Concurrent tenosynovectomy at CTR", small)],
[Paragraph("Pregnancy", body),
Paragraph("Symptom control", body),
Paragraph("Neutral splint; single intracarpal steroid injection if needed", body),
Paragraph("Usually resolves post-partum; avoid surgery unless severe", small)],
[Paragraph("CKD / Dialysis amyloid", body),
Paragraph("Symptom control; prevent progression", body),
Paragraph("Optimise dialysis; early CTR referral", body),
Paragraph("Amyloid infiltration of TCL does not respond to conservative care", small)],
[Paragraph("Acromegaly", body),
Paragraph("Normalise IGF-1 / GH", body),
Paragraph("Somatostatin analogue (octreotide) or surgery", body),
Paragraph("CTS from bony tunnel narrowing; CTR often required regardless", small)],
[Paragraph("Obesity", body),
Paragraph("BMI <30", body),
Paragraph("Lifestyle modification; bariatric referral if BMI >40", body),
Paragraph("Weight loss may reduce tunnel pressure and fluid retention", small)],
]
cause_tbl = Table(cause_data, colWidths=[28*mm, 28*mm, 62*mm, 52*mm],
style=TableStyle([
("BACKGROUND", (0,0), (-1,0), C_DARK_BLUE),
("TEXTCOLOR", (0,0), (-1,0), C_WHITE),
("GRID", (0,0), (-1,-1), 0.4, C_BORDER),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 5),
("ROWBACKGROUNDS", (0,1), (-1,-1), [C_WHITE, C_LIGHT_GRAY]),
])
)
story.append(cause_tbl)
story.append(Spacer(1, 4*mm))
# ────────────────────────────────────────────────────────────────────────────
# CLINICIAN NOTES BOX
# ────────────────────────────────────────────────────────────────────────────
story.append(section_banner("▸ CLINICIAN NOTES"))
story.append(Spacer(1, 1*mm))
notes_lines = ["" for _ in range(5)]
notes_data = [[Paragraph("____________________________________________________________________________________"
"____________________________________________________________________________________",
small)] for _ in range(5)]
notes_tbl = Table(notes_data, colWidths=[W],
style=TableStyle([
("BACKGROUND", (0,0), (-1,-1), C_LIGHT_GRAY),
("BOX", (0,0), (-1,-1), 0.8, C_BORDER),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 2),
("LEFTPADDING", (0,0), (-1,-1), 8),
])
)
story.append(notes_tbl)
story.append(Spacer(1, 4*mm))
# ── FOOTER ───────────────────────────────────────────────────────────────────
story.append(HRFlowable(width=W, thickness=0.5, color=C_BORDER))
story.append(Spacer(1, 2*mm))
story.append(Paragraph(
"Sources: Campbell's Operative Orthopaedics 15e | Goldman-Cecil Medicine | Bradley and Daroff's Neurology | "
"Textbook of Family Medicine 9e | Tintinalli's Emergency Medicine · Generated by Orris Medical AI · May 2026",
footer_s
))
story.append(Paragraph(
"⚠ This template is a clinical aide-memoire. All prescriptions must be verified by a licensed clinician. "
"Doses should be adjusted for individual patient factors including renal/hepatic function, age, weight and comorbidities.",
make_style("Disclaimer", fontSize=7, textColor=HexColor("#b71c1c"), alignment=TA_CENTER, leading=10)
))
# ── BUILD ────────────────────────────────────────────────────────────────────
doc.build(story)
print(f"PDF generated: {OUTPUT_PATH}")
Running Command
cd /home/daytona/workspace/cts-prescription && python generate_cts_rx.py
Running Command
ls -lh /home/daytona/workspace/cts-prescription/CTS_Prescription_Template.pdf
Your PDF is ready. Download it here:
CTS Prescription Template
PDF Document · PDF
Here's what's included across the 3-page PDF:
Page 1 — Patient & Assessment
- Patient/Clinician details fillable fields (name, age, MRN, date, signature, stamp)
- Clinical assessment form - CTS-6 score, Phalen/Tinel/Durkan results, thenar atrophy grade, NCS/EMG values, ultrasound CSA, symptom duration and pattern, and underlying cause checkboxes
- Severity classification table - colour-coded (green/yellow/red) with clinical features and NCS criteria for Mild / Moderate / Severe; includes a "circle your level" column
Page 2 — Mild & Moderate Prescriptions
- Mild CTS: Neutral splint protocol, nerve gliding, ergonomics; methylprednisolone 40 mg intracarpal injection with technique notes; oral prednisolone as alternative; note that NSAIDs are not recommended; baseline metabolic workup checklist
- Moderate CTS: Full-time splinting, occupational therapy referral; injection protocol + surgical decision rule (90% responders → surgery); gabapentin/amitriptyline option for neuropathic pain; disease-specific treatment lines for hypothyroidism, DM, RA, pregnancy, CKD; NCS/EMG + ultrasound investigations
Page 3 — Severe Prescription + Reference Tables
- Severe CTS: Urgent surgical referral pathway; open mini-palm CTR technique; endoscopic CTR option; special intraoperative considerations by cause (RA tenosynovectomy, Camitz opponensplasty, dialysis amyloid, post-fracture)
- Underlying cause quick-reference table - 8 conditions (hypothyroidism, DM, RA, pregnancy, CKD/amyloid, acromegaly, obesity) with treatment targets and first-line agents
- Clinician free-text notes area; source citations and clinical disclaimer footer
This is a shared conversation. Sign in to Orris to start your own chat.