Urinary bladder for mbbs 10 marks question
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive 10-mark MBBS answer. Let me compile it.
Urinary Bladder - MBBS 10 Marks Answer
1. Introduction
The urinary bladder is a hollow, distensible, muscular organ that serves as a temporary reservoir for urine. It is located in the lesser pelvis, posterior to the pubic symphysis. Its size, shape, and position vary depending on the volume of urine it contains.
- Capacity: Normally ~500 mL; the urge to void begins at ~300 mL
- When empty: bowl-shaped, lies entirely in the pelvis
- When full: ovoid, apex rises above the pubic symphysis into the abdomen
2. Gross Anatomy
Parts of the Urinary Bladder:
| Part | Description |
|---|---|
| Apex | Anterosuperior tip; gives attachment to the median umbilical ligament (remnant of urachus) |
| Body | The main bulk of the bladder |
| Fundus (Base) | Posterior and inferior; receives the two ureters |
| Neck | Inferior part; continuous with the urethra |
Trigone of the Bladder:
- A smooth triangular region on the internal floor of the bladder
- Bounded by the two ureteric orifices superolaterally and the internal urethral orifice inferiorly
- The mucosa here is firmly attached to the underlying muscle - no folds form even when empty
- Derived embryologically from the mesonephric ducts (unlike the rest of the bladder)
- Clinically important: most common site for bladder tumours and infections
Relations:
- Anterior: pubic symphysis and retropubic space (cave of Retzius)
- Superior: covered by peritoneum; small intestine rests on it when full
- Posterior (male): rectovesical pouch, seminal vesicles, vas deferens, rectum
- Posterior (female): uterovesical pouch, uterus, anterior vaginal wall
- Inferior: prostate gland (male); urogenital diaphragm (female)
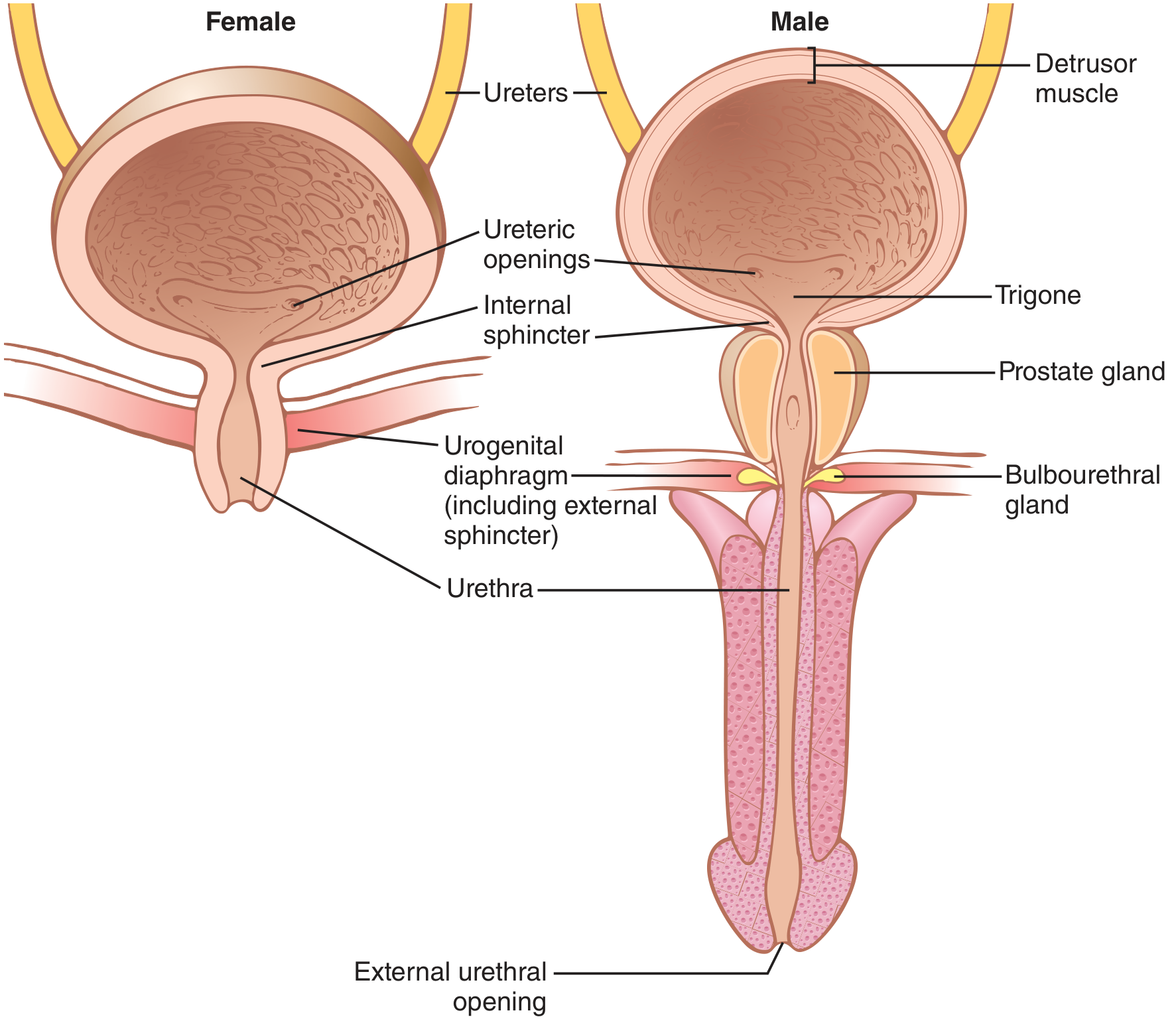
Fig. 1 - Anatomy of the urinary bladder and urethra in males and females (Guyton & Hall Textbook of Medical Physiology)
3. Microanatomy (Histology)
The bladder wall has four layers (from inside out):
a) Mucosa
- Lined by transitional epithelium (urothelium) - typically 4-6 cells thick when empty, 2-3 cells thick when distended
- The surface cells are large, dome-shaped "umbrella cells" or "facet cells"
- Lamina propria: loose connective tissue beneath the epithelium
- The mucosa forms folds (rugae) when the bladder is empty; these disappear when full
- Exception - Trigone: no muscularis mucosae or submucosal layer; mucosa is flat and firmly adherent
b) Submucosa
- Loose connective tissue; allows the mucosa to fold and unfold
c) Muscularis (Detrusor Muscle)
- Three indistinct layers of smooth muscle - inner and outer longitudinal, middle circular
- Collectively called the detrusor muscle
- At the bladder neck, the circular layer forms the involuntary internal urethral sphincter
- At the trigone: only two layers (continuation of the ureteric musculature)
d) Serosa / Adventitia
- The superior surface and part of the posterior surface are covered by peritoneum (serosa)
- The rest is covered by adventitia (fibrous connective tissue)
4. Nerve Supply (Innervation)
The bladder has a dual autonomic supply plus somatic control:
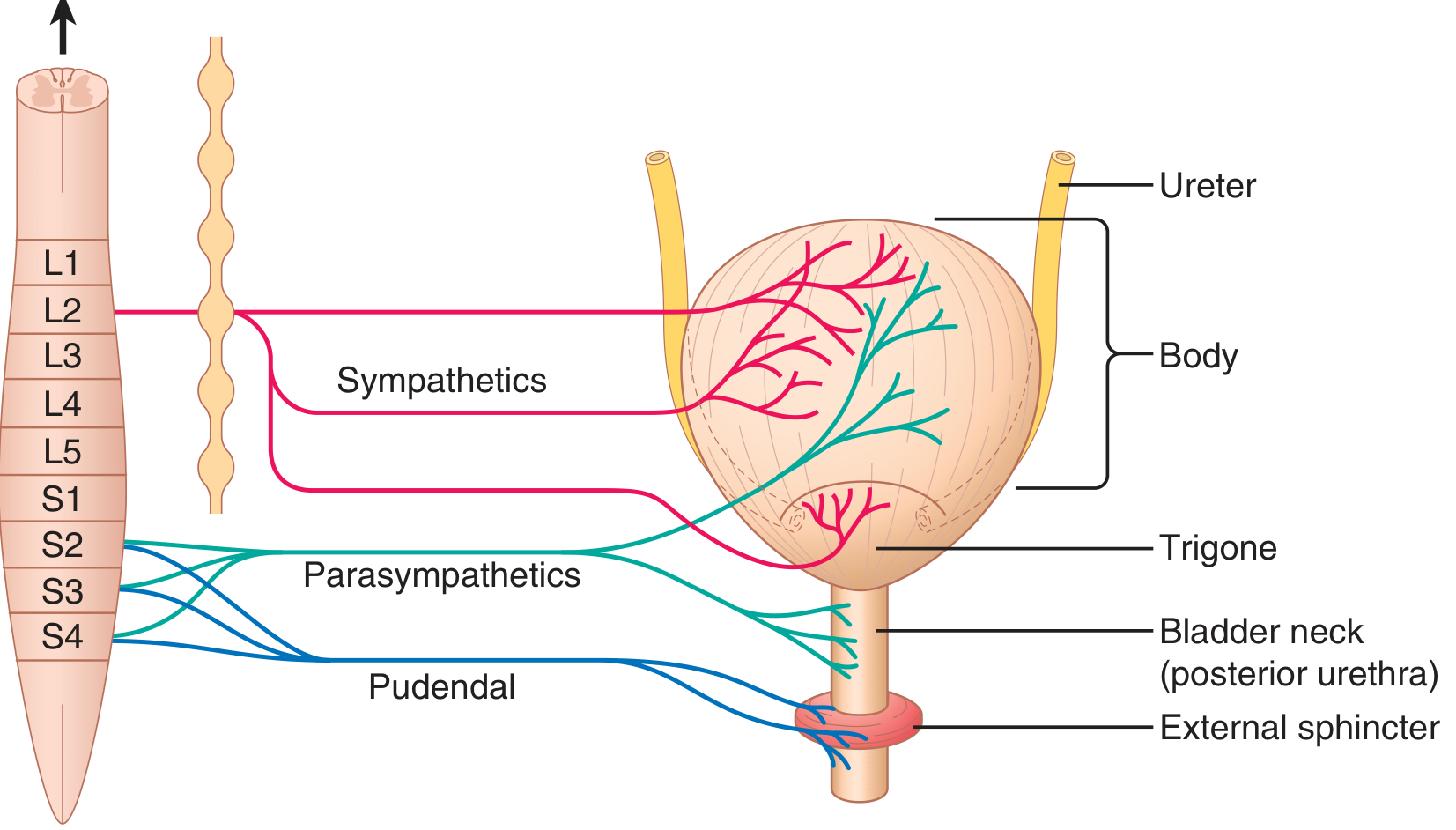
Fig. 2 - Innervation of the urinary bladder (Guyton & Hall)
| Nerve | Origin | Neurotransmitter | Effect |
|---|---|---|---|
| Sympathetic (hypogastric nerve) | L1-L2 via hypogastric plexus | Noradrenaline | β₃ receptors → relax detrusor; α₁ receptors → contract internal sphincter (filling/storage) |
| Parasympathetic (pelvic splanchnic nerves) | S2-S4 | Acetylcholine (+ NO) | M3 receptors → contract detrusor; NO → relax internal sphincter (micturition) |
| Somatic (pudendal nerve) | S2-S4 | Acetylcholine | Nicotinic receptors → tonic contraction of external (voluntary) sphincter |
| Afferent/Sensory | S2-S4 (via pelvic nerves) | - | Carries stretch signals from bladder wall to spinal cord |
Key point: During storage, sympathetic dominates (detrusor relaxed, sphincter contracted). During voiding, parasympathetic dominates (detrusor contracts, sphincter relaxes).
5. Blood Supply
-
Arterial supply:
- Superior vesical artery - from the umbilical artery (a branch of the internal iliac artery) - supplies the superior and anterosuperior parts
- Inferior vesical artery - from the internal iliac artery - supplies the fundus and neck (in males also supplies the prostate)
- Additional small branches from the obturator, inferior gluteal, and (in females) uterine and vaginal arteries
-
Venous drainage:
- The vesical venous plexus surrounds the fundus of the bladder
- Drains into the internal iliac veins
6. Lymphatic Drainage
- Superior bladder: external iliac nodes
- Inferolateral and neck: internal iliac nodes
- Trigone: external and internal iliac nodes
7. Embryological Development
The urinary bladder develops from the vesical part of the urogenital sinus, which itself arises from the ventral portion of the cloaca after it is divided by the urorectal septum (at ~4-7 weeks of development).
Key steps:
- The cloaca is divided by the descending urorectal septum into the urogenital sinus (ventral) and the rectum (dorsal)
- The urogenital sinus has three parts: vesical (upper), pelvic (middle), phallic (lower)
- The vesical part expands to form most of the bladder; its epithelium is derived from endoderm; the muscular wall is from splanchnic mesenchyme
- The bladder is initially continuous superiorly with the allantois, which later obliterates to form the urachus, then the median umbilical ligament in adults
- The trigone is formed by incorporation of the distal mesonephric (Wolffian) ducts into the posterior bladder wall - hence it has a different embryological origin than the rest of the bladder
Clinical correlations of embryology:
- Patent urachus - if urachus fails to close, urine drips from the umbilicus
- Urachal cyst - partial obliteration leaves a midline cyst
- Extrophy of bladder - failure of mesodermal migration leads to an exposed bladder on the anterior abdominal wall
8. Physiology - Micturition Reflex
Cystometrogram pattern:
- At 0-50 mL: pressure rises to 5-10 cmH₂O
- At 50-300 mL: pressure stays nearly constant (intrinsic wall tone)
- Beyond 300-400 mL: pressure rises sharply; urgent desire to void
Steps of the micturition reflex:
- Bladder fills → stretch receptors in the wall (especially posterior urethra) are activated
- Afferent signals travel via pelvic nerves to the sacral spinal cord (S2-S4) and also ascend to the pontine micturition center (PMC)
- Parasympathetic efferents fire → detrusor contracts via M3 receptors (ACh)
- Simultaneously: sympathetic inhibited (detrusor relaxes its basal tone), internal sphincter opens (NO release)
- Somatic pudendal inhibition → external sphincter relaxes
- The reflex is self-regenerating - once initiated, stretch signals increase further, amplifying the contraction until voiding is complete
- Voluntary control is exerted via higher cortical centres through the PMC - cortex can inhibit or facilitate the reflex
Abnormalities:
- Spinal cord lesion above sacral cord → automatic (uninhibited) bladder - reflexive voiding, no voluntary control
- Sacral cord/pelvic nerve lesion → autonomous (atonic) bladder - overflow incontinence, large residual urine
9. Clinical Correlations
| Condition | Relevance |
|---|---|
| Suprapubic catheterization | When bladder is full, it rises above pubic symphysis - can be punctured transabdominally without entering peritoneal cavity |
| Vesicoureteric reflux | Failure of the oblique intravesical course of ureters → urine refluxes back to kidney during voiding |
| Trigonitis / Bladder carcinoma | Trigone is most common site due to stasis and carcinogen exposure; transitional cell carcinoma most common type |
| Detrusor overactivity | Involuntary detrusor contractions → urgency/urge incontinence |
| Neurogenic bladder | Upper motor neuron (spastic) or lower motor neuron (flaccid) lesions affecting micturition reflex |
Summary Table
| Feature | Details |
|---|---|
| Location | Lesser pelvis, posterior to pubic symphysis |
| Capacity | ~500 mL (desire to void at ~300 mL) |
| Lining epithelium | Transitional epithelium (urothelium) |
| Main muscle | Detrusor muscle (3 layers of smooth muscle) |
| Arterial supply | Superior & inferior vesical arteries (from internal iliac) |
| Venous drainage | Vesical venous plexus → internal iliac veins |
| Lymphatics | External and internal iliac nodes |
| Sympathetic | L1-L2 via hypogastric nerve (storage) |
| Parasympathetic | S2-S4 via pelvic splanchnic nerves (micturition) |
| Somatic | S2-S4 via pudendal nerve (external sphincter) |
| Embryology | Vesical part of urogenital sinus; trigone from mesonephric ducts |
Sources:
- Guyton and Hall Textbook of Medical Physiology, Chapter 26
- Histology: A Text and Atlas (Gartner & Hiatt), Chapter on Urinary System
- Color Atlas of Human Anatomy, Vol. 2 - Internal Organs (Thieme)
- The Developing Human: Clinically Oriented Embryology (Moore & Persaud), Chapter 12
Urinary bladder anatomy for mbbs 10 marks
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have comprehensive, detailed anatomy content with great diagrams. Let me compile the full 10-mark anatomy answer.
Urinary Bladder - Anatomy (MBBS 10 Marks)
1. Introduction
The urinary bladder is a hollow, distensible, musculomembranous organ that acts as a temporary reservoir for urine. It is situated in the lesser (true) pelvis, behind the pubic symphysis, in the subperitoneal connective tissue. Its size, shape, and relations vary considerably depending on the volume of urine it contains and the sex of the individual.
- Capacity: ~500 mL (normal); desire to void begins at ~300 mL
- Empty state: Tetrahedral, bowl-shaped, lies entirely in the pelvis
- Full state: Ovoid; apex rises above the pubic symphysis into the lower abdomen
2. Parts of the Urinary Bladder
The bladder has four parts:
| Part | Location | Key Feature |
|---|---|---|
| Apex | Anterosuperior tip | Gives attachment to the median umbilical ligament (remnant of urachus) leading to the umbilicus |
| Body | Main bulk of the organ | Constitutes the largest part |
| Fundus (Base) | Posteroinferior | Directed downward and backward; the two ureters enter here |
| Neck | Inferiormost | Continuous below with the urethra; contains the internal urethral orifice |
3. Surfaces of the Urinary Bladder
The empty bladder has four surfaces:
- Superior surface - covered by peritoneum; in contact with coils of small intestine and sigmoid colon
- Two inferolateral surfaces - lie against the pelvic fascia and the obturator internus and levator ani muscles; no peritoneum covers these
- Posterior surface (base/fundus) - directed backward; related to seminal vesicles, vas deferens, and rectum in males; uterus and vagina in females
4. Relations
In the Male:
| Surface/Direction | Relation |
|---|---|
| Anterior | Retropubic space (of Retzius), pubic symphysis |
| Superior | Peritoneum; coils of small intestine, sigmoid colon |
| Posterior | Rectovesical pouch (peritoneum), seminal vesicles, ampullae of ductus deferens, ureters, rectum |
| Inferior (neck) | Prostate gland |
| Inferolateral | Levator ani, obturator internus |
In the Female:
| Surface/Direction | Relation |
|---|---|
| Anterior | Retropubic space, pubic symphysis |
| Superior | Vesicouterine pouch (peritoneum), uterus |
| Posterior | Anterior vaginal wall (base), cervix and lower uterus (superior) |
| Inferior (neck) | Urogenital diaphragm |
| Inferolateral | Levator ani, obturator internus |
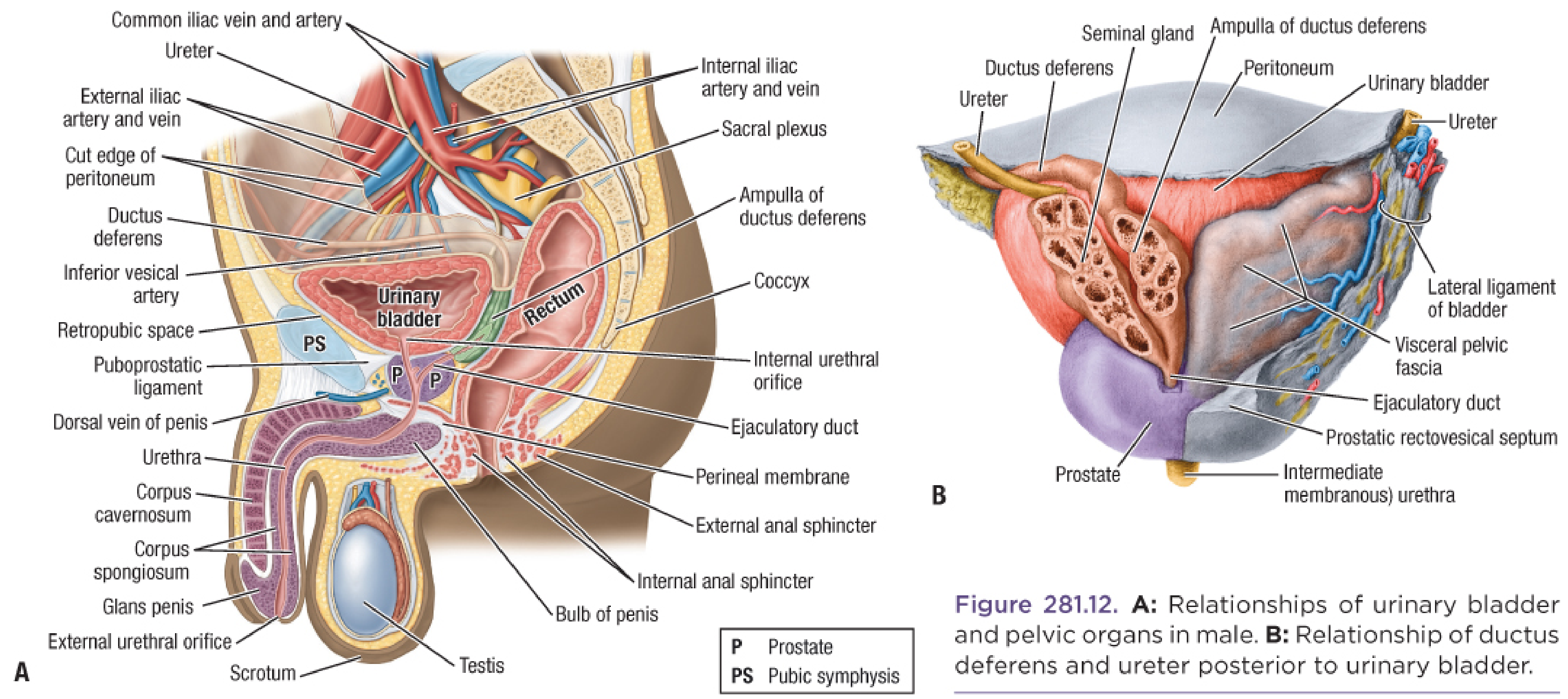
Fig. 1 - Relations of the male urinary bladder and pelvic organs (Fischer's Mastery of Surgery)
5. Interior of the Bladder
When opened from the front, the interior shows:
Rugae (Mucosal Folds)
- The mucosa of most of the bladder forms irregular folds (rugae) when empty because it is loosely attached to the underlying muscle
- The rugae disappear completely when the bladder is distended
Trigone of the Bladder
The trigone is the most important internal landmark:
- A smooth, triangular area on the base (fundus) of the bladder
- Bounded by three orifices:
- Two ureteric orifices (superolateral corners) - where the ureters enter the bladder obliquely
- Internal urethral orifice (inferior apex) - where the urethra begins
- The interureteric fold (bar of Mercier) is a raised ridge connecting the two ureteric orifices - this is the superior boundary of the trigone
- The mucosa of the trigone is always smooth and firmly attached to the underlying muscle - no rugae form here
- The trigone is derived from the mesonephric ducts (different embryological origin from rest of bladder)
Uvula of the Bladder (Male Only)
- A small conical elevation at the internal urethral orifice produced by the underlying median lobe of the prostate
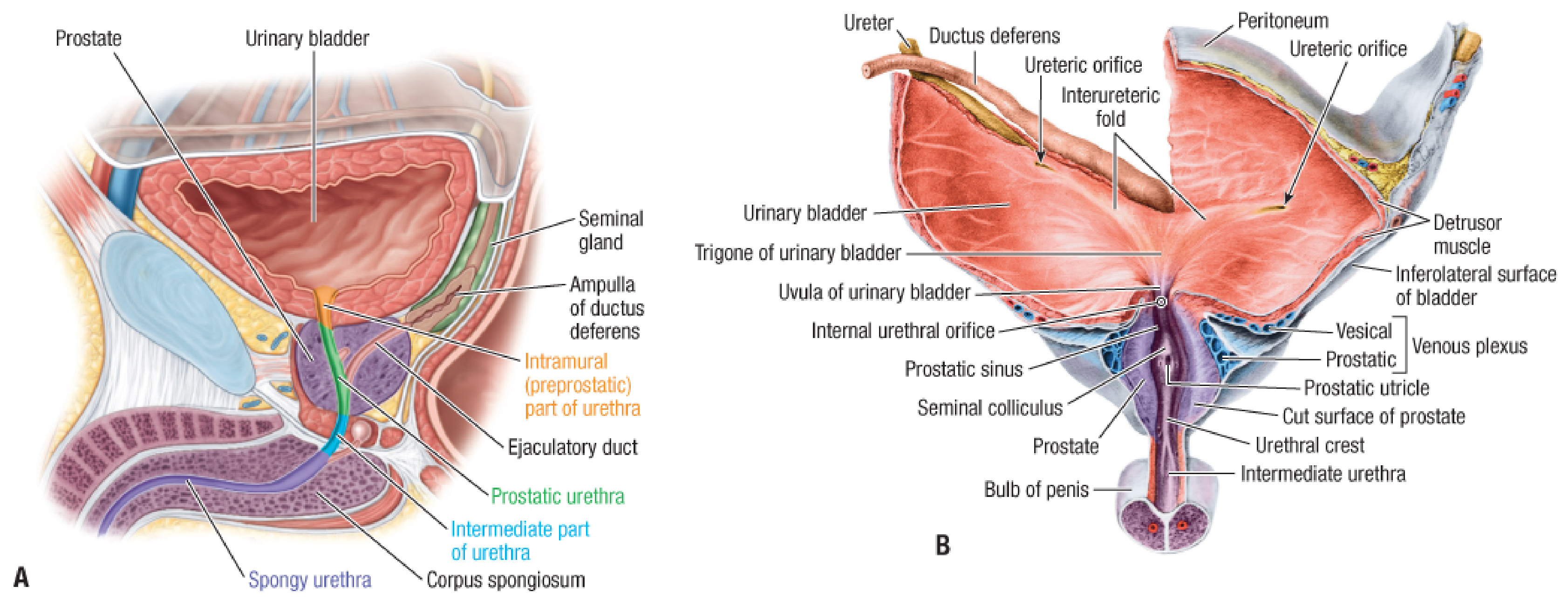
Fig. 2 - Interior of urinary bladder and prostate showing trigone, uvula, and internal features (Fischer's Mastery of Surgery)
6. Coats (Layers) of the Bladder Wall
From inside outward:
a) Mucosa
- Lined by transitional epithelium (urothelium)
- Rests on lamina propria (loose connective tissue)
- Forms rugae everywhere except the trigone
- Trigone exception: no muscularis mucosae or submucosa - mucosa is flat and non-folding
b) Submucosa
- Loose areolar connective tissue
- Allows the mucosa to fold and glide over the muscular layer
- Absent at the trigone
c) Muscularis (Detrusor Muscle)
- Three layers of smooth muscle - inner longitudinal, middle circular, outer longitudinal
- The three layers are not distinct and interdigitate with each other (unlike the GI tract)
- Collectively called the detrusor muscle
- At the bladder neck, the circular fibers condense to form the internal urethral sphincter (involuntary smooth muscle)
- At the trigone, the musculature is a continuation of the smooth muscle of the ureters (only two layers)
d) Serosa / Adventitia
- Serosa (peritoneum): covers only the superior surface and the upper part of the posterior surface
- Adventitia (fibrous connective tissue): covers all other surfaces
7. Blood Supply
Arteries (all branches of the Internal Iliac Artery):
| Artery | Origin | Supply |
|---|---|---|
| Superior vesical artery | From the patent part of the umbilical artery | Superior and anterosuperior bladder, distal ureter |
| Inferior vesical artery | Directly from the anterior division of the internal iliac artery (or vaginal artery in females) | Fundus, neck, trigone; also supplies prostate and seminal vesicles in males |
| Additional small branches | Obturator, inferior gluteal, uterine, vaginal arteries | Supplementary supply |
Veins:
- The vesical venous plexus surrounds the fundus and inferolateral surfaces
- Drains into the internal iliac veins
- In males, the vesical plexus is continuous with the prostatic venous plexus
- In females, it is continuous with the vaginal venous plexus
8. Lymphatic Drainage
| Region of Bladder | Drains To |
|---|---|
| Superior and anterosuperior | External iliac nodes |
| Inferolateral and neck | Internal iliac (hypogastric) nodes |
| Trigone | External and internal iliac nodes |
| Posterior wall | Obturator nodes |
Clinical note: For radical cystectomy in bladder cancer, pelvic lymph node dissection must include external iliac, internal iliac, and obturator node groups.
9. Nerve Supply
| Nerve | Origin | Function |
|---|---|---|
| Parasympathetic (pelvic splanchnic nerves) | S2-S4 sacral cord | Motor to detrusor (via M3 muscarinic receptors) - mediates micturition |
| Sympathetic (hypogastric nerve) | L1-L2 via hypogastric plexus | Relaxes detrusor (β₃), contracts internal sphincter (α₁) - mediates storage |
| Somatic (pudendal nerve) | S2-S4 | Controls external urethral sphincter (voluntary) |
| Afferent/sensory | S2-S4 via pelvic nerves | Carries stretch and pain signals to spinal cord |
10. Peritoneal Relations and Ligaments
- The peritoneum reflects from the anterior abdominal wall onto the superior surface of the bladder only, then passes backwards onto the uterus (female) or rectum (male), forming the vesicouterine pouch or rectovesical pouch respectively
- The anterior and lateral walls of the bladder are extraperitoneal
- Ligaments of the bladder:
- Median umbilical ligament (urachus) - apex to umbilicus
- Lateral umbilical ligaments (obliterated umbilical arteries) - lateral walls to umbilicus
- Puboprostatic ligaments (male) / Pubovesical ligaments (female) - neck to pubis
- Lateral ligaments of bladder - from posterolateral bladder to pelvic wall (contain the inferior vesical vessels)
11. Applied Anatomy (Clinical Points)
| Application | Basis |
|---|---|
| Suprapubic catheterization / cystostomy | When full, bladder rises above pubic symphysis - can be punctured transabdominally above the pubis without entering the peritoneal cavity |
| Vesicoureteric reflux | Ureters enter the bladder obliquely through the detrusor muscle (intramural segment ~2 cm); this valve-like mechanism prevents reflux; failure → recurrent UTIs and pyelonephritis |
| Bladder carcinoma | Most commonly arises in the trigone and lateral walls; transitional cell carcinoma (urothelial carcinoma) is the most common type |
| Injury in pelvic fracture | Bladder rupture - extraperitoneal (more common, involving the base) or intraperitoneal (involving the superior surface) |
| Haematuria after catheterization | The trigone is the most sensitive area; catheter tip irritation causes bleeding |
| Bladder neck obstruction (males) | Enlargement of the prostate directly compresses the bladder neck/internal urethral orifice |
| Cystoscopy landmarks | The trigone and interureteric bar are the key landmarks for locating ureteric orifices during cystoscopy |
Quick Revision Summary
POSITION: Lesser pelvis, behind pubic symphysis (full → rises above pubis)
CAPACITY: ~500 mL; desire to void at ~300 mL
PARTS: Apex, Body, Fundus (base), Neck
COATS: Mucosa (TCC) → Submucosa → Detrusor muscle → Serosa/Adventitia
TRIGONE: Between 2 ureteric orifices + internal urethral orifice; always smooth
ARTERIES: Superior + Inferior vesical (branches of internal iliac artery)
VEINS: Vesical venous plexus → Internal iliac veins
LYMPHATICS: External iliac, internal iliac, obturator nodes
NERVES: Para S2-S4 (micturition); Symp L1-L2 (storage); Pudendal S2-S4 (ext. sphincter)
PERITONEUM: Covers only superior surface and upper posterior surface
Sources:
- Color Atlas of Human Anatomy, Vol. 2 - Internal Organs (Thieme), p. 405
- Fischer's Mastery of Surgery, 8th ed., Chapter 281
- Sabiston Textbook of Surgery, 21st ed., Chapter on Bladder and Prostate
- Bailey & Love's Short Practice of Surgery, 28th ed., Applied Anatomy of the Bladder
- Histology: A Text and Atlas (Gartner & Hiatt), Chapter on Urinary System
This is a shared conversation. Sign in to Orris to start your own chat.