Acute appendicitis surgery topic with proper understanding with photos in simple language
Reading File
Finding Sources
Finding Sources
Searching the Web
acute appendicitis surgery overview anatomy pathophysiology treatment 2024
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Searching the Web
laparoscopic appendectomy surgical steps trocar placement diagram 2024
Loading Image
Loading Image
I have all the content I need. Now let me compile a comprehensive, well-organized response.
Acute Appendicitis & Appendectomy - A Complete Guide
1. What is the Appendix?
The appendix (vermiform appendix = "worm-shaped") is a small, hollow, finger-like tube about 9 cm long and 0.6 cm wide. It hangs off the beginning of the large intestine (cecum) in the right lower abdomen.
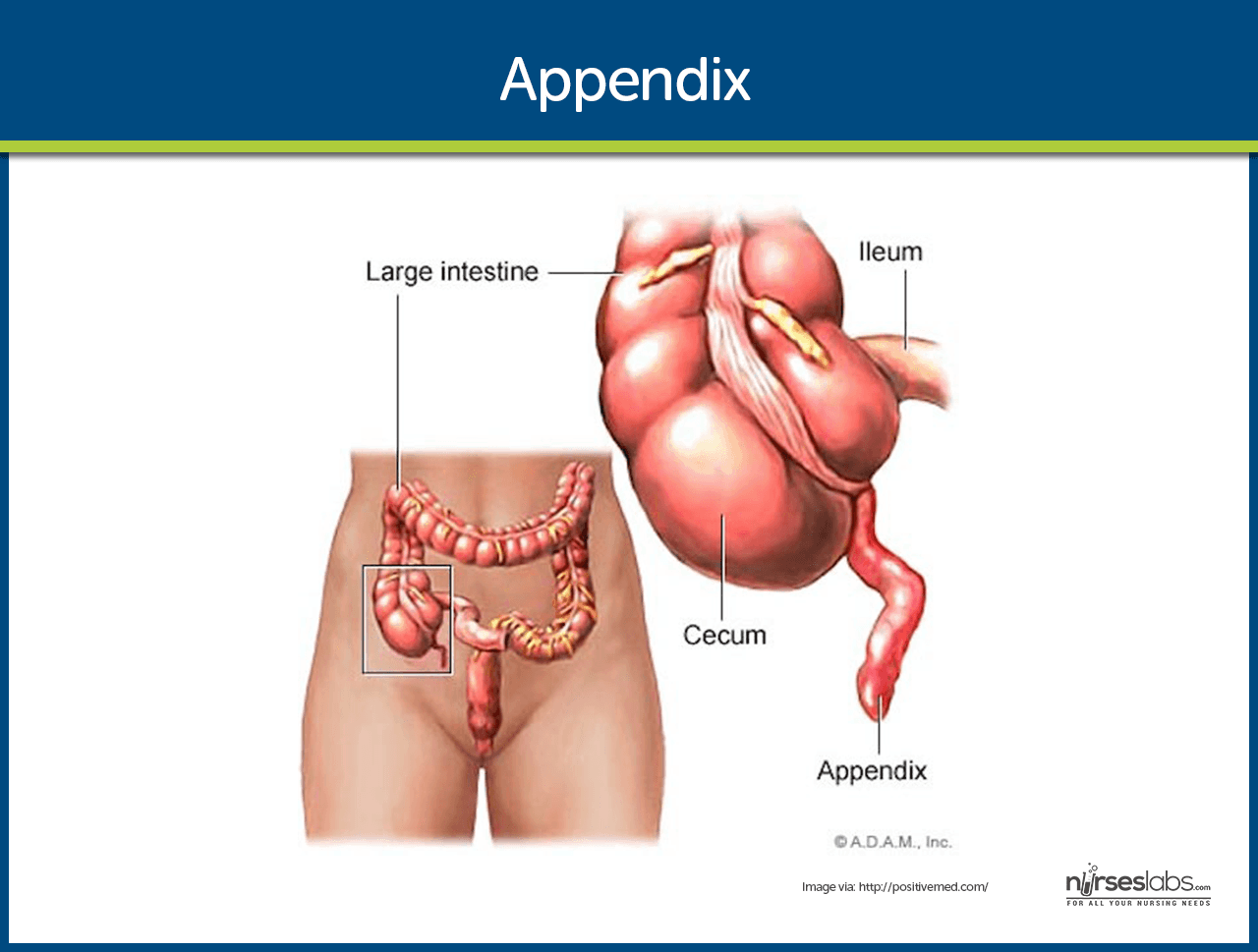
Key anatomy facts:
- It arises from the cecum where the three taenia coli converge
- Blood supply comes from the appendiceal artery, a branch of the ileocolic artery
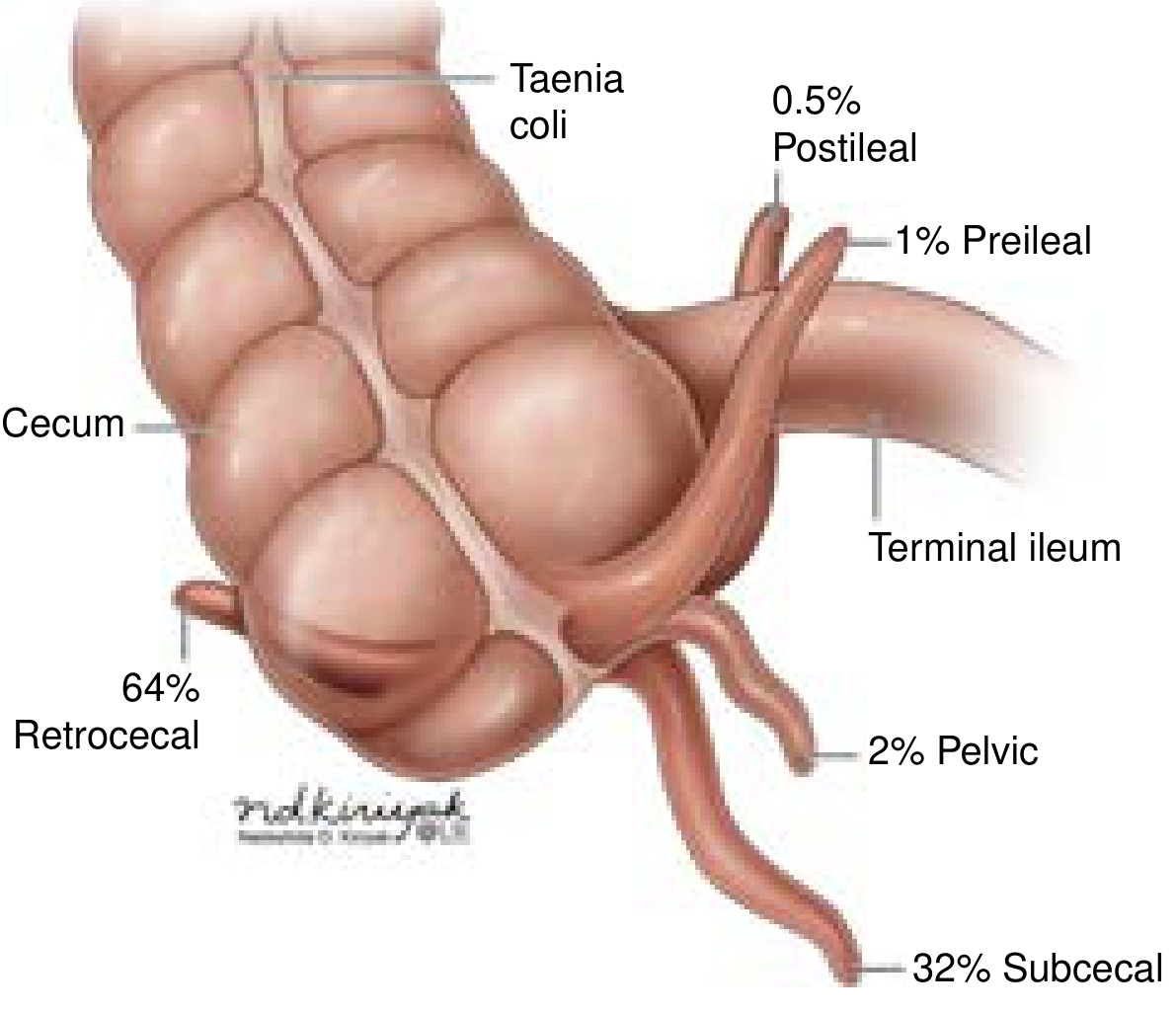
- Its tip can point in different directions - most commonly retrocecal (64%), subcecal (32%), pelvic (2%), or preileal/postileal positions. This is why pain location can vary between patients.
2. What is Acute Appendicitis?
Acute appendicitis = sudden inflammation of the appendix. It is the most common cause of emergency abdominal surgery worldwide.
- Global incidence: 100-150 per 100,000 people per year
- Lifetime risk: 7-10%
- In the USA: ~400,000 cases per year; 16-40% are perforated at diagnosis
3. What Causes It? (Pathophysiology)
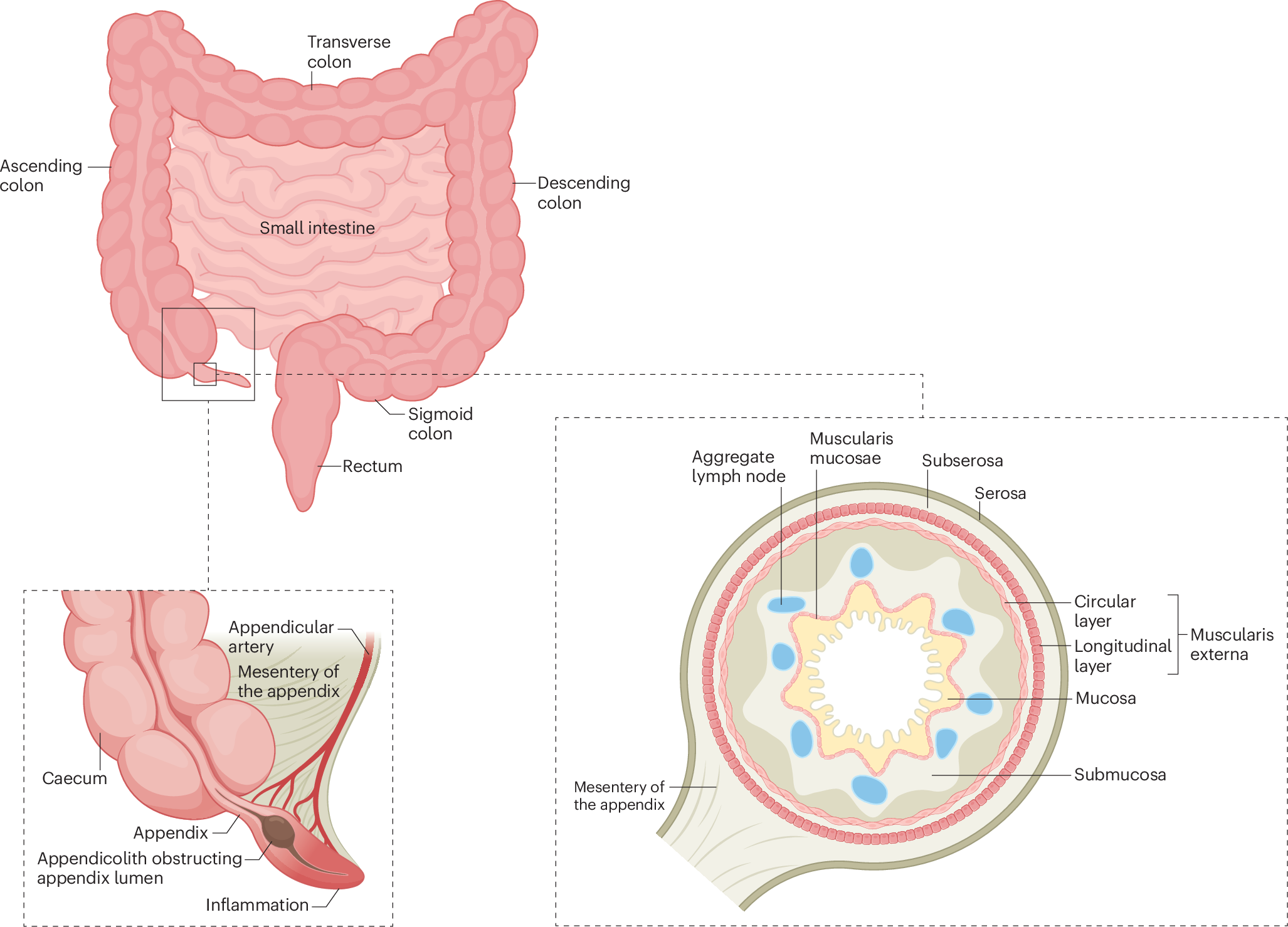
The root cause is blockage of the appendix lumen, which triggers a cascade:
Obstruction → Bacterial overgrowth → Mucus buildup → Distension
↓
Venous congestion → Arterial blockage → Ischemia → Gangrene
↓
PERFORATION + ABSCESS
Common causes of obstruction:
| Cause | Details |
|---|---|
| Fecalith / appendicolith | Hardened stool - most common |
| Lymphoid hyperplasia | Enlarged lymph nodes (common in children after infection) |
| Parasites | Pinworms, etc. |
| Tumor / neoplasm | Rare cause in adults |
| Foreign body | Very rare |
Bacteria involved: E. coli, Bacteroides fragilis, Klebsiella, Streptococcus, Pseudomonas
- Current Surgical Therapy 14e, p. 324
4. Symptoms - What Does It Feel Like?
The classic progression:
Step 1 - Vague belly button / upper abdominal pain (visceral pain as appendix distends)
Step 2 - Nausea, vomiting, loss of appetite
Step 3 - Pain shifts to the right lower abdomen (RLQ) - now somatic/peritoneal pain
Step 4 - Fever, tenderness, inability to move without pain
Key Physical Signs
| Sign | What You Do | What It Means |
|---|---|---|
| McBurney's point tenderness | Press 1/3 of the way from right hip bone to belly button | Classic RLQ tenderness |
| Rovsing's sign | Press on the left side - pain felt on the right | Peritoneal irritation |
| Psoas sign | Extend right hip - causes pain | Retrocecal appendix |
| Obturator sign | Internally rotate right hip - causes pain | Pelvic appendix |
| Rebound tenderness | Press then release quickly - worse pain on release | Peritonitis |
| Guarding | Involuntary muscle stiffening | Advanced inflammation |
5. How Is It Diagnosed?
Diagnosis uses a combination of history, examination, blood tests, and imaging.
Blood Tests
- WBC (leukocytosis) - elevated in ~80% of cases
- CRP (C-reactive protein) - elevated, useful with WBC
- Negative urine culture (rules out UTI)
- Negative pregnancy test (rules out ectopic)
The Alvarado Score (MANTRELS)
A simple scoring system used to estimate risk:
| Feature | Points |
|---|---|
| Migration of pain to RLQ | 1 |
| Anorexia | 1 |
| Nausea/vomiting | 1 |
| RLQ tenderness | 2 |
| Rebound tenderness | 1 |
| Elevated temperature | 1 |
| Leukocytosis (WBC>10k) | 2 |
| Total | 10 |
- Score 1-4: Low risk (likely not appendicitis)
- Score 5-6: Intermediate (consider imaging)
- Score 7-10: High risk (likely appendicitis, consider surgery)
Imaging
| Modality | Use | Notes |
|---|---|---|
| Ultrasound (US) | First-line (children, pregnant women) | No radiation; operator-dependent |
| CT scan (abdomen/pelvis) | Gold standard for adults | Most accurate, ~98% sensitivity |
| MRI | Pregnant patients when US inconclusive | No radiation, but slower |
CT findings of appendicitis: Appendix diameter >6 mm, wall thickening, periappendiceal fat stranding, fecalith, abscess
6. Treatment
Option A: Antibiotics Alone (Non-Operative Management / NOM)
For uncomplicated appendicitis (not perforated, no fecalith):
- Recent studies show antibiotics can be effective as primary treatment
- Success rate ~70-80% at 1 year; 20-30% eventually need appendectomy
- Antibiotic of choice: piperacillin-tazobactam (IV), then oral step-down
Option B: Surgery (Appendectomy) - Definitive Treatment
Surgery remains the standard definitive treatment for acute appendicitis, especially for:
- Perforated appendicitis
- Abscess formation
- Failed antibiotic therapy
- Fecalith present on imaging
7. The Surgery - Appendectomy
There are two approaches:
A. Laparoscopic Appendectomy (Preferred, Modern Approach)
What it is: Minimally invasive surgery using a camera and small instruments through tiny holes (ports/trocars) in the abdomen.
Steps:
- Anesthesia - General anesthesia (patient is fully asleep)
- Positioning - Patient lies flat (supine); may tilt left-side-down during surgery for better view
- Port placement - Three small cuts (~5-12 mm):
- Port 1: At the belly button (camera/umbilical port, 12 mm)
- Port 2: Left lower abdomen (5 mm working port)
- Port 3: Right lower abdomen or suprapubic (5 mm working port)
- Insufflation - CO₂ gas pumped in to inflate the abdomen (12-15 mmHg) so the surgeon can see
- Find the appendix - Follow the cecum to where the taenia coli converge
- Divide the mesoappendix - Using a stapler or energy device (Ligasure), the blood vessels are cut
- Divide the appendix base - Stapler or Endoloop tie used to close and cut the appendix off
- Remove the appendix - Placed in a bag and pulled out through the belly button port
- Irrigate - If infected fluid is present, it is washed out
- Close - Small cuts are sutured/stapled closed
Advantages of laparoscopic approach:
- Smaller scars
- Less pain after surgery
- Faster recovery (home in 1-2 days typically)
- Lower wound infection rate
- Better visibility for diagnosis
B. Open Appendectomy (Traditional Approach)
Used when:
- Laparoscopy not available
- Severe perforation with difficult anatomy
- Dense adhesions
Steps:
- General anesthesia
- A 3-4 cm incision at McBurney's point (right lower quadrant) - this is called a Lanz incision or gridiron incision
- Muscles are split (not cut) to reach the peritoneum
- Appendix is identified and delivered into the wound
- Mesoappendix is ligated and divided
- Appendix base is tied and divided
- Stump may be inverted with a purse-string suture
- Layers closed in sequence
8. Perforated vs. Uncomplicated Appendicitis
| Feature | Uncomplicated | Perforated |
|---|---|---|
| Appendix wall | Intact | Hole/rupture present |
| Duration of symptoms | <48-72 hours usually | Often >72 hours |
| WBC | Mildly elevated | Very high |
| Fever | Low-grade | High fever |
| Abdominal exam | Localized RLQ tenderness | Diffuse tenderness, rigid abdomen |
| Treatment | Laparoscopic appendectomy OR antibiotics | Emergency surgery + IV antibiotics |
| Complications | Low | High - abscess, peritonitis, sepsis |
9. Special Situations
Appendiceal Abscess / Phlegmon
- When the appendix perforates and the body walls it off
- Treatment: Interval approach - IV antibiotics + possible CT-guided drainage, then interval appendectomy 6-8 weeks later
- This avoids operating in a "dirty" inflamed field
Pregnancy
- Most common surgical emergency in pregnancy
- Appendix is displaced upward as the uterus grows (but less than classically taught - only moves >25% in late pregnancy)
- Ultrasound first; MRI if inconclusive; CT if needed and life is at risk
- Surgery is safe at any trimester; laparoscopy is safe in first and second trimester
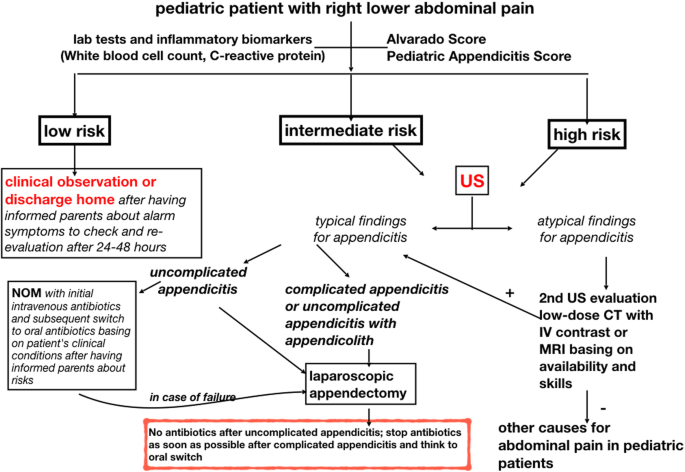
Children
- Perforation is much more common in children (up to 40-70% at presentation)
- Because children cannot describe pain well and diagnosis is delayed
- Pediatric Appendicitis Score (PAS) is used alongside Alvarado
10. Postoperative Care & Complications
Recovery (Typical)
- Laparoscopic: Home in 1-2 days; back to normal activities in 1-2 weeks
- Open: Home in 2-4 days; back to normal in 2-4 weeks
- Diet: Clear liquids first, then regular diet as tolerated
- Pain: Managed with oral medications (NSAIDs + paracetamol)
Possible Complications
| Complication | When | Notes |
|---|---|---|
| Wound infection | Days 3-7 | More common with perforated cases |
| Abscess (intra-abdominal) | Days 5-14 | Treated with drainage ± antibiotics |
| Ileus (bowel slowdown) | Days 1-3 | Usually resolves with walking and time |
| Bleeding | Intraoperative | Rare with laparoscopy |
| Bowel injury | Intraoperative | Very rare |
| Negative appendectomy | At surgery | Appendix found to be normal (~5-15%) |
| Stump appendicitis | Months later | Very rare - inflamed appendix stump |
Overall mortality rate: 0.09-0.24% (very safe surgery)
11. Summary Diagram - The Full Picture
Normal Appendix
|
OBSTRUCTION (fecalith/lymphoid tissue)
|
Bacteria multiply + mucus builds up
|
Distension → Periumbilical pain + nausea
|
Venous congestion → Ischemia
|
Pain moves to RLQ (McBurney's point)
|
NECROSIS → GANGRENE
|
PERFORATION → Peritonitis / Abscess / Sepsis
|
SURGERY (Appendectomy) or IV Antibiotics
Quick Reference Card
| Feature | Details |
|---|---|
| Most common age | 10-30 years (but any age) |
| Most common in | Males slightly > females |
| First symptom | Periumbilical / central abdominal pain |
| Classic sign | McBurney's point tenderness |
| Best imaging | CT scan (adults); Ultrasound (children/pregnant) |
| Surgery type | Laparoscopic appendectomy (preferred) |
| Surgery time | ~30-60 minutes |
| Hospital stay | 1-3 days (uncomplicated) |
| Recovery | 1-2 weeks (laparoscopic) |
| If untreated | Perforation, peritonitis, sepsis, death |
Sources: Current Surgical Therapy 14e (Mahdi & Pegoli); Rosen's Emergency Medicine 9e; Gray's Anatomy for Students; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.