Acute decompensated heart failure
Reading File
Finding Sources
Searching PubMed
"acute decompensated heart failure" AND management
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of Acute Decompensated Heart Failure (ADHF):
Acute Decompensated Heart Failure (ADHF)
Definition & Epidemiology
ADHF is a heterogeneous clinical syndrome resulting from the confluence of decreased cardiac performance, renal dysfunction, and altered vascular compliance — severe enough to necessitate hospitalization. It carries a high burden:
- In-hospital mortality: ~5%
- 1-year mortality: ~20%
- Readmission within 6 months: ~50%
- Combined adverse events at 12 months (CV death, HF hospitalization, MI, stroke, sudden death): ~50%
Precipitating Factors
Identifying the trigger is the first principle of management:
| Category | Examples |
|---|---|
| Medication non-adherence | Missed diuretics, dietary salt excess |
| Drugs that worsen HF | NSAIDs, thiazolidinediones, TNF inhibitors, certain antidepressants, cancer therapies |
| Ischemia | Coronary artery disease (investigate invasively or noninvasively) |
| Arrhythmias | Atrial fibrillation, ventricular tachycardia → cardioversion, ablation |
| Valvular disease | Readily identified on echocardiography |
| Infection / PE | Sepsis, pulmonary thromboembolism |
Clinical Phenotypes & Management Framework
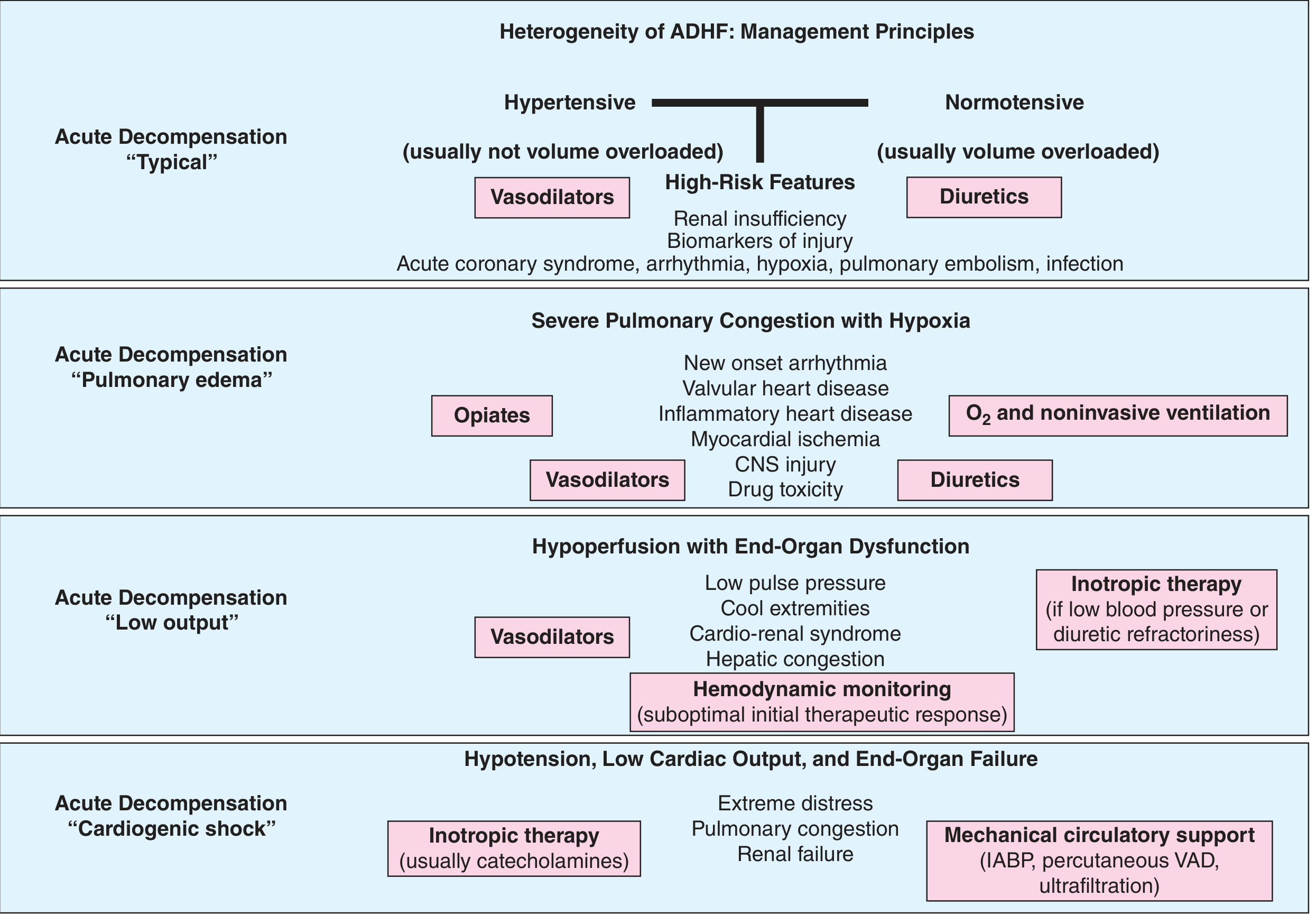
Figure: ADHF phenotypes with associated treatments — Harrison's Principles of Internal Medicine 22E
| Phenotype | Key Features | Primary Treatment |
|---|---|---|
| Hypertensive | Elevated BP, usually NOT volume overloaded | IV vasodilators (nitroglycerin, nitroprusside, nesiritide) |
| Normotensive (volume overloaded) | Typical congestion, edema | IV loop diuretics |
| Pulmonary edema | Severe hypoxia, congestion | O₂ + noninvasive ventilation, vasodilators, diuretics, opiates |
| Low-output | Cool extremities, low pulse pressure, cardiorenal syndrome | Vasodilators ± inotropes; hemodynamic monitoring |
| Cardiogenic shock | Hypotension, end-organ failure, extreme distress | Catecholamines (inotropes) + mechanical circulatory support (IABP, percutaneous VAD, ultrafiltration) |
Volume Management
IV Loop Diuretics
- First-line for congestion relief; essential when oral absorption is impaired
- Bolus vs. continuous infusion: No clear difference in clinical trials (DOSE trial)
- High vs. low dose: No significant difference in symptom scores, though high dose improved decongestion
- Sequential nephron blockade: Add thiazide (metolazone or chlorothiazide) for diuretic resistance — increases risk of hypokalemia
- Acetazolamide + loop diuretic (ADVOR trial): Greater decongestion but no reduction in readmissions or mortality
- Torsemide vs. furosemide: TRANSFORM-HF showed no mortality/morbidity advantage despite better oral bioavailability
Endpoints for euvolemia: Normalized JVP, cleared pulmonary rales, resolution of S3 gallop, peripheral edema, ascites; predischarge BNP/NT-proBNP predicts postdischarge risk
IV Vasodilators
- Nitroglycerin, nitroprusside, nesiritide (recombinant BNP)
- Counteract neurohormonal activation (sympathetic tone, angiotensin II, aldosterone, endothelin, AVP)
- Most useful in hypertensive phenotype
Ultrafiltration (Aquapheresis)
- Controlled fluid removal with electrolyte-neutral effect
- CARRESS-HF trial: No superiority over stepped pharmacologic care; higher adverse events
- Reserved for diuretic-refractory cases
Pulmonary Artery Catheter — When to Use
Routine use is not recommended. Restrict to:
- Low-output HF or cardiogenic shock needing vasopressor/mechanical support
- Diuretic-resistant or refractory cases
- Cardiorenal dysfunction where goals are unclear
- Known/suspected pulmonary arterial hypertension
High-risk markers: BUN >43 mg/dL, SBP <115 mmHg, creatinine >2.75 mg/dL, elevated BNP/troponin
Cardiorenal Syndrome
- Occurs in ~30% of hospitalized ADHF patients
- Not simply reduced renal perfusion — neurohormonal, elevated intraabdominal pressure, and renal venous congestion all contribute
- Worsening GFR with diuresis does not necessarily worsen prognosis if decongestion is achieved
- Severe low-output state: short-term inotropic therapy or mechanical support to bridge to definitive therapy
Inotropic & Vasopressor Therapy
- Dobutamine (β₁ agonist): increases contractility; first-line inotrope in low-output HF
- Dopamine: dose-dependent effects; lower doses renal/vasodilatory, higher doses vasopressor
- Milrinone (PDE inhibitor): combined inotropic + vasodilatory; useful in β-blocker–treated patients
- Norepinephrine/vasopressin: reserved for cardiogenic shock with refractory hypotension
- Levosimendan: calcium sensitizer with inotropic and vasodilatory properties; approved in many countries (not US)
Discharge & Transition Therapy
Key evidence-based strategies at discharge:
| Trial | Intervention | Result |
|---|---|---|
| PIONEER-HF | Sacubitril-valsartan (ARNI) vs. enalapril pre-discharge | Greater NT-proBNP reduction; lower death + readmission at 8 weeks |
| EMPULSE | Empagliflozin (SGLT-2i) pre-discharge | Improved hierarchical clinical composite at 90 days |
| STRONG-HF | Intensive post-discharge follow-up + rapid uptitration of GDMT | Lower death + readmission at 180 days (regardless of EF) |
Before discharge: Patient education on fluid/salt restriction, daily weights, symptom recognition, early follow-up (within 7 days reduces readmission)
Failed or Disappointing Therapies
- Rolofylline (adenosine A1 antagonist): no benefit in PROTECT trial
- Tolvaptan (vasopressin-2 antagonist): no mortality/morbidity benefit in EVEREST trial
- Bosentan (endothelin antagonist): worsened HFrEF
- Moxonidine (central sympatholytic): worsened outcomes
Recent Evidence (2024–2025)
- Prehospital lung ultrasound for diagnosing ADHF: high diagnostic accuracy (SR/MA, PMID 38522242)
- Subcutaneous furosemide: emerging role in outpatient HF management (SR, PMID 39352583)
- Restricted sodium intake during hospitalization: SR/MA shows no clear mortality benefit (PMID 40450575)
Sources: Harrison's Principles of Internal Medicine 22E (2025), Brenner & Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.