Read this article and explain mechanism of action in picture formats of how Passive ultrasonic irrigation and Diode Laser Irrigation Techniques helps in Smear Layer Removal, Sealer Penetration
cd /home/daytona/workspace/attachments/53066e0a-e709-4935-80f2-8511f4af0d2c/ && python3 -c " from pypdf import PdfReader reader = PdfReader('AZ1.pdf') print(f'Pages: {len(reader.pages)}') text = '' for i, page in enumerate(reader.pages): text += f'\n\n=== PAGE {i+1} ===\n' text += page.extract_text() or '' print(text[:8000]) "
cd /home/daytona/workspace/attachments/53066e0a-e709-4935-80f2-8511f4af0d2c/ && python3 -c " from pypdf import PdfReader reader = PdfReader('AZ1.pdf') text = '' for i, page in enumerate(reader.pages): text += f'\n\n=== PAGE {i+1} ===\n' text += page.extract_text() or '' print(text[8000:]) "
A detailed educational medical diagram titled "Passive Ultrasonic Irrigation (PUI) - Mechanism of Action in Smear Layer Removal and Sealer Penetration". The diagram should show a cross-section of a root canal tooth with the following labeled sequential steps arranged in a flowchart/infographic style: Step 1 (top): "Ultrasonic File/Tip Inserted into Irrigant-Filled Canal" - show a thin ultrasonic file tip inside a root canal filled with blue irrigant solution Step 2: "High-Frequency Vibrations (25-30 kHz)" - show acoustic waves radiating from the tip in concentric circles Step 3: "Acoustic Streaming" - arrows showing circular fluid movement patterns around the vibrating tip Step 4: "Cavitation Effect" - small bubbles forming and collapsing near the canal walls, with shockwave arrows pointing at the wall Step 5: "Smear Layer Disruption" - zoomed-in cross-section of canal wall showing smear layer (grey layer) being broken apart, with debris particles floating away. Label: "Organic + inorganic debris and microorganisms removed" Step 6: "Open Dentinal Tubules" - show clean dentinal tubules exposed after smear layer removal, with small circular openings visible Step 7 (bottom): "Sealer Penetration" - show AH Plus sealer (red) flowing deep into open dentinal tubules, with arrows showing sealer entering 40+ micrometers into tubules. Label: "Mechanical interlocking improves bond strength" Include a side panel showing comparison: "With Smear Layer = Blocked tubules, poor sealer bond" vs "Without Smear Layer = Open tubules, deep sealer penetration, better seal". Clean, professional, white background, medical textbook style with clear labels and color-coded stages.
A detailed educational medical diagram titled "980 nm Diode Laser Irrigation - Mechanism of Action in Smear Layer Removal and Sealer Penetration". The diagram should show a root canal cross-section with sequential labeled steps in a flowchart/infographic style: Step 1 (top): "400 µm Fiber Tip Inserted 2mm Short of Working Length" - show a thin laser fiber tip inside root canal filled with EDTA irrigant, with a measurement arrow showing 2mm from apex Step 2: "980 nm Diode Laser Activated at 2W Continuous Mode" - show the fiber tip emitting a red laser beam with wavelength annotation "980 nm" Step 3: "Photothermal Effect" - show heat waves radiating from the fiber tip into the irrigant (orange/red heat halo). Label: "Irrigant temperature rises, increases reactivity" Step 4: "Photomechanical Effect" - show pressure waves (shockwaves) expanding outward from tip into irrigant, pushing fluid laterally. Arrows showing helical/apicocoronal removal movement of the tip Step 5: "Photochemical Activation of EDTA Irrigant" - show EDTA molecules becoming more reactive, dissolving smear layer components. Label: "Enhanced chelation of inorganic smear layer" Step 6: "Smear Layer Dissolution" - zoomed cross-section of canal wall showing the grey smear layer being chemically dissolved, with clean dentin surface revealed Step 7: "Dentin Morphology Changes" - show increased surface irregularities on dentin walls. Label: "Surface roughness aids mechanical adhesion" Step 8 (bottom): "Sealer Penetration" - show AH Plus sealer (orange) flowing into open dentinal tubules with arrows. Label: "Deep penetration into dentinal tubules, improved microleakage resistance and push-out bond strength" Include a small inset box: "Key Parameters: Wavelength 980nm | Power 2W | Tip 400µm | Continuous mode | 10 sec per 1mL irrigant". Clean white background, professional medical illustration style, color-coded numbered steps.
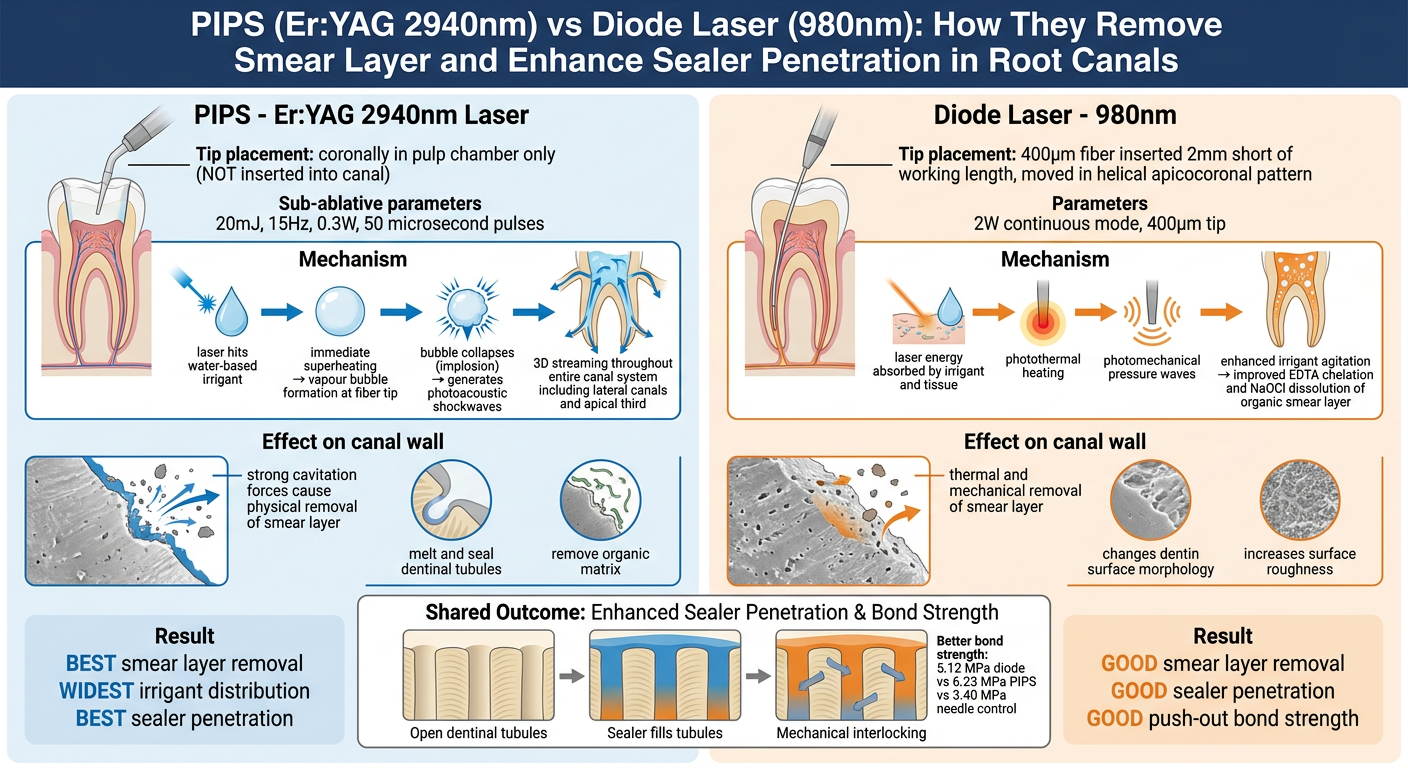
A comprehensive side-by-side comparison infographic titled "PIPS (Er:YAG 2940nm) vs Diode Laser (980nm): How They Remove Smear Layer and Enhance Sealer Penetration in Root Canals". LEFT COLUMN - "PIPS - Er:YAG 2940nm Laser": - Tip placement: coronally in pulp chamber only (NOT inserted into canal) - Sub-ablative parameters: 20mJ, 15Hz, 0.3W, 50 microsecond pulses - Mechanism box showing: laser hits water-based irrigant → immediate superheating → vapour bubble formation at fiber tip → bubble collapses (implosion) → generates photoacoustic shockwaves → 3D streaming throughout entire canal system including lateral canals and apical third - Effect on canal wall: strong cavitation forces cause physical removal of smear layer, melt and seal dentinal tubules, remove organic matrix - Result: BEST smear layer removal, WIDEST irrigant distribution, BEST sealer penetration RIGHT COLUMN - "Diode Laser - 980nm": - Tip placement: 400µm fiber inserted 2mm short of working length, moved in helical apicocoronal pattern - Parameters: 2W continuous mode, 400µm tip - Mechanism box showing: laser energy absorbed by irrigant and tissue → photothermal heating → photomechanical pressure waves → enhanced irrigant agitation → improved EDTA chelation and NaOCl dissolution of organic smear layer - Effect on canal wall: thermal and mechanical removal of smear layer, changes dentin surface morphology, increases surface roughness - Result: GOOD smear layer removal, GOOD sealer penetration, GOOD push-out bond strength BOTTOM: Shared outcome diagram showing: Open dentinal tubules → Sealer fills tubules → Mechanical interlocking → Better bond strength (5.12 MPa diode vs 6.23 MPa PIPS vs 3.40 MPa needle control) White background, clean modern medical infographic style, blue for PIPS column, orange for Diode column.
Diagram 1: Passive Ultrasonic Irrigation (PUI) - Mechanism
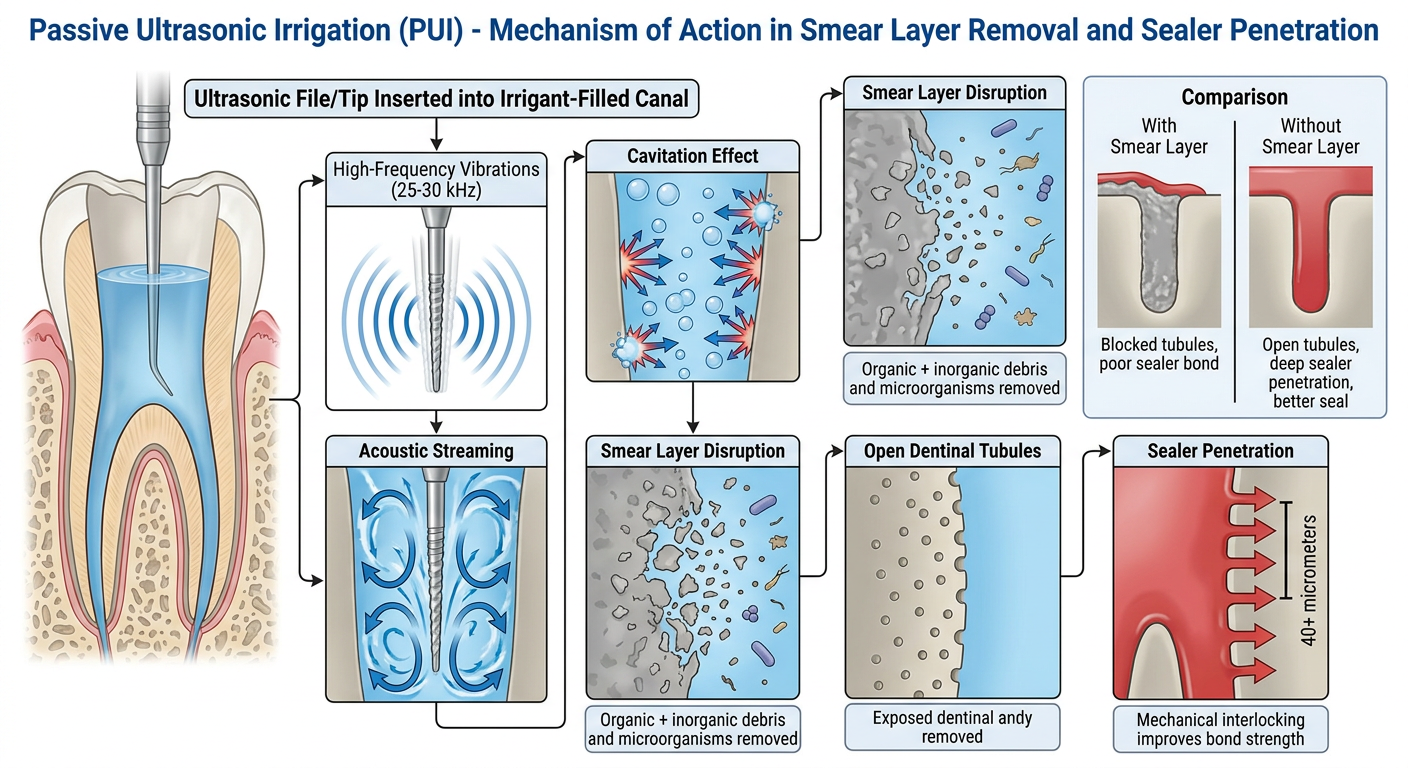
Diagram 2: 980 nm Diode Laser Irrigation - Mechanism
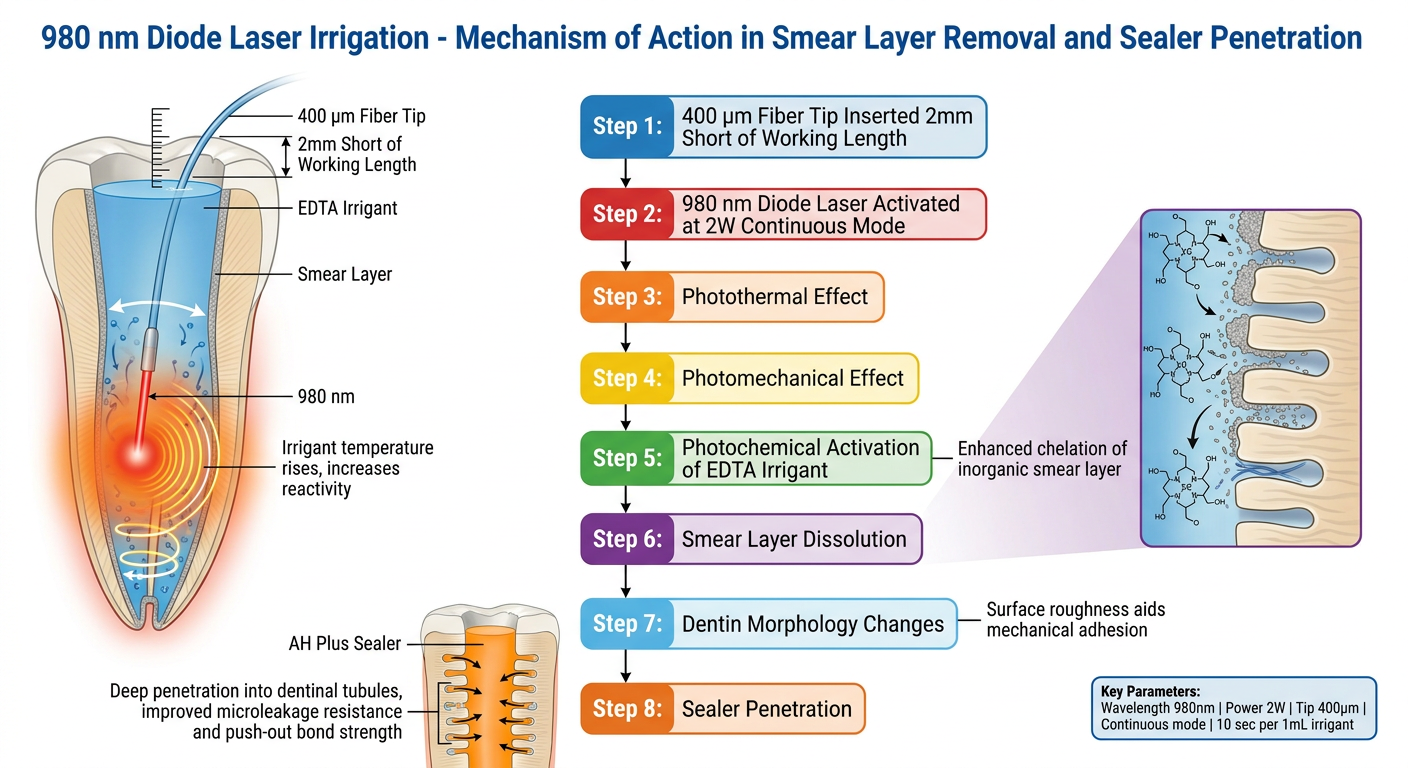
Diagram 3: PIPS (Er:YAG) vs Diode Laser - Side-by-Side Comparison
Mechanism Explained in Detail (from the Article)
Smear Layer - What It Is
- Inorganic dentin debris
- Organic pulp tissue remnants
- Odontoblastic processes
- Microorganisms and their metabolic products
Mechanism 1: Diode Laser Irrigation (980 nm)
| Parameter | Value |
|---|---|
| Wavelength | 980 nm |
| Power | 2 W |
| Mode | Continuous |
| Tip | 400 µm |
| Activation time | 10 sec per 1 mL irrigant (total 40 sec) |
- Photothermal effect - The 980 nm wavelength is absorbed by the irrigant (EDTA/NaOCl), raising its temperature and increasing chemical reactivity.
- Photomechanical effect - Pressure waves radiate outward from the tip, physically agitating the irrigant and pushing it into canal irregularities.
- Enhanced EDTA chelation - Thermal activation accelerates the chelation of inorganic smear layer components by EDTA.
- Dentin morphology changes - Laser irradiation increases surface roughness and irregularities on dentin walls - these micro-irregularities improve mechanical interlocking with sealer.
- Smear layer removal - The combination of chemical and physical effects dissolves and dislodges the smear layer from canal walls and dentinal tubule orifices.
- Sealer penetration - With open tubule orifices and a roughened dentin surface, AH Plus sealer penetrates deeply into dentinal tubules, forming a mechanical lock.
Mechanism 2: PIPS - Photon-Induced Photoacoustic Streaming (Er:YAG 2940 nm)
| Parameter | Value |
|---|---|
| Wavelength | 2940 nm |
| Energy | 20 mJ (sub-ablative) |
| Frequency | 15 Hz |
| Power | 0.3 W |
| Pulse duration | 50 microseconds (super-short) |
| Tip | 400 µm stripped quartz PIPS tip |
- Laser launched into aqueous irrigant - The Er:YAG 2940 nm wavelength is highly absorbed by water (the base of all irrigant solutions).
- Superheating - The irrigant immediately heats beyond its boiling point at the fiber tip.
- Vapour bubble formation - Bubbles form rapidly at the end of the fiber tip.
- Bubble implosion (cavitation) - Bubbles grow to maximum volume, then collapse violently. This collapse is called inertial cavitation.
- Photoacoustic shockwaves - The implosion generates powerful shockwaves that propagate in all three dimensions throughout the root canal system - including the apical third, lateral canals, and isthmi that the tip never physically enters.
- 3D irrigant streaming - Shockwaves drive the irrigant in continuous 3-dimensional streaming throughout the entire canal, including areas unreachable by a needle or fiber tip.
- Smear layer physical removal - The lateral and shear forces from cavitation physically strip the smear layer from canal walls, remove organic matrix, and dislodge debris. Dentinal tubules are opened.
- Sealer penetration - Fully cleared tubule orifices allow AH Plus sealer to penetrate deeply, creating superior mechanical interlocking.
How Smear Layer Removal Leads to Better Sealer Penetration - The Chain
Laser Activation
↓
Smear Layer Removed from Canal Wall
↓
Dentinal Tubule Orifices Opened
↓
Sealer (AH Plus) Penetrates into Tubules
↓
Mechanical Interlocking at Sealer-Dentin Interface
↓
Reduced Microleakage + Higher Push-out Bond Strength
Summary Comparison (from the article)
| Parameter | Side-Vented Needle | Diode (980 nm) | PIPS Er:YAG (2940 nm) |
|---|---|---|---|
| Smear layer removal | Least | Good | Best |
| Dye penetration (mm) | 5.70 | 4.20 | 2.95 |
| Sealer penetration | Minimal into tubules | Good | Very good |
| Push-out bond strength | 3.40 MPa | 5.12 MPa | 6.23 MPa |
| Tip position | 2 mm from apex | 2 mm from apex | Coronal only |
explain diagram in 150 words
Diagram Explanation (150 words)
explain diagram 1 in 150 words
Diagram 1 - Passive Ultrasonic Irrigation (PUI): Explanation (150 words)
explain diagram 2 in 170 words
Diagram 2 - Diode Laser Irrigation (980 nm): Explanation (170 words)
- Photothermal effect - the irrigant heats up, increasing its chemical reactivity and accelerating EDTA's chelation of inorganic smear layer components
- Photomechanical effect - pressure waves radiate outward, physically agitating the irrigant and pushing it into canal irregularities and accessory canals
- Photochemical activation - enhanced dissolution of both organic and inorganic smear layer components
what are different irrigating solutions
endodontic irrigating solutions types mechanisms of action root canal
Endodontic Irrigating Solutions
1. Non-Bactericidal Irrigants
| Solution | Use |
|---|---|
| Normal Saline (0.9% NaCl) | Biocompatible flushing agent; used as final rinse or control in studies |
| Distilled Water | Rarely used; no antimicrobial properties |
| Local Anesthetics | Occasional use; no clinical advantage |
2. Bactericidal Irrigants
Sodium Hypochlorite (NaOCl) - Gold Standard
- Concentrations: 0.5%, 1%, 2.5%, 5.25%, 6%
- Mechanism:
- Saponification - dissolves fatty acids in bacterial cell membranes
- Chloramination - chlorine reacts with amino groups, disrupting cellular proteins
- Neutralization of amino acids - denatures proteins
- High pH (>11) disrupts bacterial enzyme activity
- Unique advantage: Dissolves both vital and necrotic pulp tissue (organic component of smear layer)
- Limitation: Cannot remove the inorganic (mineral) smear layer component; cytotoxic if extruded apically
Chlorhexidine (CHX) - 2%
- Mechanism:
- Positively charged molecule attracted to negatively charged bacterial cell wall phospholipids
- Disrupts osmotic equilibrium → cell lysis and death
- Key advantage: Substantivity - binds to dentin and releases slowly, giving prolonged antimicrobial effect even after rinsing
- Limitation: Cannot dissolve pulp tissue; forms toxic precipitate (parachloroaniline/PCA) when mixed with NaOCl
Hydrogen Peroxide (H₂O₂) - 3%
- Releases nascent oxygen on contact with tissue → effervescent bubbling action
- Mechanically dislodges debris; weak antimicrobial effect
- Largely replaced by more effective agents
Iodine Potassium Iodide (IKI)
- Broad-spectrum antimicrobial; effective against E. faecalis
- Used mainly as intracanal medicament; risk of allergy
3. Chelating Agents (Smear Layer Removers)
EDTA (17%) - Most Widely Used
- Mechanism: Chelates calcium ions from dentin mineral matrix → demineralizes and softens dentin surface → opens dentinal tubule orifices
- Used as final irrigant after NaOCl (NaOCl removes organic, EDTA removes inorganic)
- pH 7.7 (used in the article being studied)
- Enhanced with ultrasonics/laser activation for deeper penetration
Citric Acid (10-50%)
- Chelating and mild antimicrobial properties
- Effective smear layer removal; more biocompatible than EDTA at lower concentrations
MTAD (Mixture of Tetracycline, Acid and Detergent)
- Contains doxycycline + citric acid + Tween 80 (detergent)
- Removes smear layer AND has antimicrobial action
- Effective against E. faecalis
Maleic Acid (7%)
- Comparable smear layer removal to EDTA with less dentin erosion
Tetraclean
- Similar to MTAD; contains lower doxycycline concentration
4. Newer / Herbal / Alternative Irrigants
| Irrigant | Mechanism |
|---|---|
| Ozone (O₃) | Powerful oxidizing agent; antimicrobial; destroys bacterial cell wall |
| Electrochemically Activated Water (EAW) | Produces hypochlorous acid in situ; antimicrobial |
| Neem extract | Plant-based; antibacterial and antifungal |
| Turmeric (Curcumin) | Anti-inflammatory and antimicrobial |
| Propolis | Broad-spectrum antimicrobial; biocompatible |
| Chitosan | Chelating + antimicrobial; biodegradable |
| Photoactivated Disinfection (PAD) | Photosensitizer dye + laser light → singlet oxygen kills bacteria |
Ideal Properties of an Endodontic Irrigant (Zehnder's Criteria)
- Broad-spectrum antimicrobial activity
- Dissolves pulp tissue (organic)
- Removes smear layer (inorganic)
- Inactivates endotoxins
- Non-toxic to periapical tissues
- Non-allergenic
- Does not weaken dentin structure
No single irrigant fulfills all criteria. This is why sequential use of NaOCl + EDTA (as used in the article) is the clinical standard - NaOCl removes organic debris and kills bacteria, while EDTA chelates the inorganic smear layer, together achieving complete smear layer removal and maximum sealer penetration.
Give 10 differences between N-acteyl cyiestine,sodium hypochlorite,EDTA ,saline
N-acetyl cysteine endodontic irrigant properties mechanism smear layer comparison
N-acetyl cysteine root canal irrigation endodontics
10 Differences: N-Acetyl Cysteine vs Sodium Hypochlorite vs EDTA vs Saline
| # | Property | N-Acetyl Cysteine (NAC) | Sodium Hypochlorite (NaOCl) | EDTA (17%) | Saline (0.9% NaCl) |
|---|---|---|---|---|---|
| 1 | Chemical Nature | Thiol-containing amino acid derivative (mucolytic agent) | Strong alkaline oxidizing agent | Polyaminocarboxylic acid (chelating agent) | Isotonic salt solution (inert) |
| 2 | Mechanism of Action | Breaks disulfide bonds in biofilm matrix; free thiol group disrupts bacterial cell wall; inhibits pro-inflammatory cytokines | Saponification + chloramination + protein denaturation; releases hypochlorous acid (HOCl) at high pH | Chelates Ca²⁺ ions from dentin mineral matrix → demineralizes smear layer inorganic component | Mechanical flushing only; no chemical action on bacteria or tissue |
| 3 | Antimicrobial Activity | Moderate; effective against E. faecalis, C. albicans, biofilms; also anti-endotoxin activity | Strong broad-spectrum bactericidal, sporicidal, virucidal | None (not antimicrobial) | None |
| 4 | Smear Layer Removal | Partial - removes organic component + has mild chelating action; recent studies show comparable sealer tubule penetration to EDTA (PMID: 40302832) | Removes organic component only (pulp tissue, collagen) | Removes inorganic component only (mineral/calcium deposits) | No smear layer removal |
| 5 | Tissue Dissolution | Mucolytic - dissolves mucus and organic biofilm matrix; does NOT dissolve pulp tissue like NaOCl | Dissolves both vital and necrotic pulp tissue completely | Minimal tissue dissolution; slight softening of dentin surface | None |
| 6 | Biocompatibility / Toxicity | High biocompatibility; anti-inflammatory; reduces periapical inflammation by inhibiting TNF-α, IL-1β, IL-6 | Cytotoxic to periapical tissues if extruded; causes tissue necrosis, air emphysema; foul smell and taste | Generally biocompatible; excessive use can over-demineralize and weaken dentin | Excellent biocompatibility; completely non-toxic |
| 7 | Effect on Dentin Structure | Mildly softens surface dentin; does NOT significantly alter microhardness at therapeutic concentrations | Reduces dentin microhardness and flexural strength with prolonged use; weakens root structure | Decreases dentin microhardness and increases surface roughness due to calcium chelation; risk of over-erosion of tubules | No effect on dentin structure whatsoever |
| 8 | Sealer Penetration Effect | Improves sealer penetration into dentinal tubules by removing biofilm and opening tubule orifices; comparable to EDTA in recent confocal studies | Poor sealer penetration alone (cannot remove inorganic smear layer blocking tubules) | Best tubule-opening agent; significantly enhances sealer penetration depth when used as final rinse | No improvement; tubules remain blocked by smear layer |
| 9 | Anti-Biofilm / Anti-Endotoxin | Strong anti-biofilm action (breaks extracellular polysaccharide matrix); inactivates bacterial endotoxins (LPS) - PMID: 39469595 | Good anti-biofilm at high concentrations (6% most effective); partially inactivates endotoxins | No anti-biofilm or anti-endotoxin activity | No anti-biofilm or anti-endotoxin activity |
| 10 | Clinical Status & Concentration Used | Emerging/investigational irrigant; typically used at 10 mM concentration; not yet mainstream in clinical endodontics (PMID: 39893616 - systematic review 2025) | Gold standard; most widely used; 2.5% or 5.25% clinically | Standard chelating agent; used at 17% as final irrigant after NaOCl | Used as inert control/final flush; standard saline 0.9% |
Key Clinical Takeaway
NaOCl → dissolves ORGANIC smear layer + kills bacteria
+
EDTA → chelates INORGANIC smear layer + opens tubules
=
Complete smear layer removal + maximal sealer penetration
why NAC is used as a key irrigant instead of Naocl and EDTA
N-acetylcysteine endodontic irrigation biofilm smear layer
why N-acetyl cysteine NAC advantages over NaOCl EDTA endodontic irrigation limitations
Why NAC Is Gaining Interest - Not as a Replacement, But as a Superior Adjunct
The Limitations That Drive Interest in NAC
Problems with NaOCl:
- Highly cytotoxic to periapical tissues if accidentally extruded - causes severe tissue necrosis, pain, swelling, emphysema
- Weakens dentin - causes collagen breakdown, reduces flexural strength and microhardness with prolonged use
- Cannot remove inorganic smear layer (needs EDTA as a partner)
- High surface tension limits penetration into accessory canals and isthmuses
- Unpleasant smell and taste; bleaches clothing; corrodes metal instruments
- Does not fully eliminate biofilms at lower concentrations - only 6% NaOCl is consistently effective against established biofilms
Problems with EDTA:
- No antimicrobial activity whatsoever
- Excessive use causes over-demineralization - erodes dentinal tubule walls, makes dentin structurally weak
- No anti-inflammatory benefit
- Cannot dissolve organic tissue
Why NAC Addresses These Gaps
1. Superior Anti-Biofilm Action
- A study found 200 mg/mL NAC was more effective than 5.25% NaOCl and 2% CHX combined in killing E. faecalis and S. mutans biofilms
- NAC suppresses E. faecalis biofilm development and elimination - the most resilient endodontic pathogen responsible for treatment failures
2. Anti-Inflammatory Properties - Unique to NAC
- Inhibits pro-inflammatory cytokines: TNF-α, IL-1β, IL-6
- Elevates Resolvin E1 and D2 - potent endogenous inflammation-resolving mediators
- Reduces periapical tissue destruction during active infection
- Protects apical stem cells - making it especially valuable in regenerative endodontic procedures (REPs)
3. Antioxidant Protection
4. Better Biocompatibility
| Safety Profile | NaOCl | EDTA | NAC |
|---|---|---|---|
| Cytotoxicity to periapical tissue | High | Low | Very low |
| Dentin weakening | Yes | Yes (over-use) | Minimal |
| Tissue irritation | Severe if extruded | Mild | Minimal |
| Safe concentration window | Narrow | Moderate | Wide |
5. Smear Layer Removal + Sealer Penetration
The Argument: Why NAC Could Serve as a Single-Agent Irrigant
NaOCl EDTA NAC
───────── ───────── ─────────────────────────
Kills bacteria + Chelates smear = Does BOTH + also:
Dissolves pulp layer (inorganic) • Disrupts biofilm matrix
• Anti-inflammatory
• Antioxidant
• Protects stem cells
• Biocompatible
• No dentin weakening
Why NAC Is Still NOT the Standard (Honest Limitations)
| Limitation | Detail |
|---|---|
| No pulp tissue dissolution | Cannot dissolve necrotic pulp - still needs NaOCl for that |
| Limited clinical trials | Most evidence is in-vitro; large RCTs in humans are lacking |
| Concentration not standardized | Studies use 10 mM to 200 mg/mL - no consensus on optimal dose |
| Long-term dentin effects unknown | Not yet fully characterized in vivo |
| Not yet in mainstream guidelines | AAE and ESE have not formally endorsed NAC as a primary irrigant |
Current Clinical Reality
- Adjunct to NaOCl + EDTA in cases with persistent infection
- Primary irrigant in regenerative endodontics (REPs) where stem cell preservation is critical and NaOCl's cytotoxicity is a concern
- Intracanal medicament between appointments in cases of apical periodontitis
COMPRESS THIS IN SHORT-The Limitations That Drive Interest in NAC Problems with NaOCl: Highly cytotoxic to periapical tissues if accidentally extruded - causes severe tissue necrosis, pain, swelling, emphysema Weakens dentin - causes collagen breakdown, reduces flexural strength and microhardness with prolonged use Cannot remove inorganic smear layer (needs EDTA as a partner) High surface tension limits penetration into accessory canals and isthmuses Unpleasant smell and taste; bleaches clothing; corrodes metal instruments Does not fully eliminate biofilms at lower concentrations - only 6% NaOCl is consistently effective against established biofilms Problems with EDTA: No antimicrobial activity whatsoever Excessive use causes over-demineralization - erodes dentinal tubule walls, makes dentin structurally weak No anti-inflammatory benefit Cannot dissolve organic tissue Why NAC Addresses These Gaps 1. Superior Anti-Biofilm Action NAC's free thiol (-SH) group directly breaks the disulfide bonds in the extracellular polymeric substance (EPS) that holds biofilm matrix together. This physically dismantles the biofilm scaffold - something NaOCl and EDTA cannot do as efficiently at safe concentrations. A study found 200 mg/mL NAC was more effective than 5.25% NaOCl and 2% CHX combined in killing E. faecalis and S. mutans biofilms NAC suppresses E. faecalis biofilm development and elimination - the most resilient endodontic pathogen responsible for treatment failures 2. Anti-Inflammatory Properties - Unique to NAC This is NAC's most distinct advantage over all other irrigants: Inhibits pro-inflammatory cytokines: TNF-α, IL-1β, IL-6 Elevates Resolvin E1 and D2 - potent endogenous inflammation-resolving mediators Reduces periapical tissue destruction during active infection Protects apical stem cells - making it especially valuable in regenerative endodontic procedures (REPs) Neither NaOCl nor EDTA offers ANY anti-inflammatory benefit. 3. Antioxidant Protection NAC is a precursor to glutathione - the body's master antioxidant. It neutralizes reactive oxygen species (ROS) generated during infection, reducing oxidative damage to periapical tissues. This property is entirely absent in NaOCl and EDTA. 4. Better Biocompatibility Safety Profile NaOCl EDTA NAC Cytotoxicity to periapical tissue High Low Very low Dentin weakening Yes Yes (over-use) Minimal Tissue irritation Severe if extruded Mild Minimal Safe concentration window Narrow Moderate Wide 5. Smear Layer Removal + Sealer Penetration A 2025 confocal laser scanning microscopy study (PMID: 40302832) comparing NAC, maleic acid and EDTA showed NAC achieved comparable dentinal tubule penetration depth of epoxy resin sealer to EDTA - meaning it can serve the chelating role while simultaneously providing antimicrobial and anti-inflammatory benefits in a single irrigant.
Why NAC? - Compressed Summary
Limitations of Conventional Irrigants
How NAC Fills These Gaps
| Advantage | Mechanism |
|---|---|
| Anti-biofilm | Free -SH group breaks EPS disulfide bonds; 200 mg/mL NAC outperforms 5.25% NaOCl + 2% CHX against E. faecalis |
| Anti-inflammatory | Inhibits TNF-α, IL-1β, IL-6; elevates Resolvins E1/D2 - absent in both NaOCl and EDTA |
| Antioxidant | Glutathione precursor; neutralizes ROS-mediated periapical tissue damage |
| Biocompatible | Very low cytotoxicity, minimal dentin weakening, wide safe concentration window |
| Smear layer removal | Achieves sealer tubule penetration comparable to EDTA (PMID: 40302832, 2025) |
use articles and tell why Sealer penetration was most consistent in the coronal third and least in the apical third across all groups, consistent with existing anatomical and histological knowledge..
sealer penetration dentinal tubules coronal apical third root canal
why sealer penetration least apical third root canal anatomical histological reasons dentinal tubules
Why Sealer Penetration Is Best in the Coronal Third and Worst in the Apical Third
1. Dentinal Tubule Density Decreases Apically
| Root Third | Tubule Density | Implication |
|---|---|---|
| Coronal | ~45,000 tubules/mm² | Maximum entry points for sealer |
| Middle | ~35,000 tubules/mm² | Moderate penetration |
| Apical | ~8,000-20,000 tubules/mm² | Fewer openings; sealer has limited entry |
2. Dentinal Sclerosis is Most Advanced at the Apex
- Sclerotic dentin has reduced permeability - irrigants and sealers cannot physically enter calcified tubules
- This process preferentially affects the apical third first
- A 2025 article in the Journal of Clinical Medicine (PMC12898071) states: "age-related dentinal sclerosis and reduced tubule permeability preferentially develop in the apical portion of the root, further limiting sealer penetration"
3. Cementum-Like Material and Intratubular Mineral Deposits
- Resist chelation by EDTA
- Block tubule orifices even after instrumentation
- Reduce dentin permeability independently of smear layer
4. Canal Diameter Narrows Apically - Irrigant Access Is Limited
- The larger coronal diameter allows free movement of irrigating solutions, better exchange of fresh irrigant, and greater hydraulic pressure against canal walls
- As the canal tapers toward the apex, irrigant flow velocity drops, exchange of fresh solution is minimal, and the vapor lock effect traps air bubbles apically, preventing irrigant from reaching the last 2-3 mm
- A confocal laser scanning microscopy study on chelating agents (PMC9978241) concluded: "decrease in the diameter of the root canal at the apex decreases the access of irrigants, which consequently results in reduction of flow - the apical area remains uncleaned"
5. Instrument Access and Preparation Quality
- Endodontic files follow a taper - preparation is always wider coronally and narrower apically
- Accessory canals, isthmuses, fins, and canal ramifications are most complex and numerous in the apical third (Vertucci's classification)
- Instruments cannot physically contact all apical walls - 20-30% of the apical canal surface remains untouched after instrumentation (Dalton et al.)
- Uninstrumented walls retain smear layer → block tubule orifices → prevent sealer entry
Supporting Evidence Across Studies
| Study | Key Finding |
|---|---|
| PMC12898071, 2025 - Sealer in apical third after irrigation techniques | Less penetration in apical region linked to reduced tubule density, sclerosis, cementum-like material |
| PMC9978241 - EDTA vs citric acid vs maleic acid + bioceramic sealer | Maximum sealer penetration in coronal third for all tested irrigants; Kara et al. confirmed same pattern |
| Cureus SEM study 2026 - 4 sealers compared | Coronal sealer penetration significantly higher than middle and apical in all 4 groups |
| Abdelgawad et al. 2022 (the article you read) | PIPS and diode laser improved penetration but the coronal > apical gradient persisted across all groups |
| Tan et al. 2022 Meta-analysis PMID: 36463149 | Sonic activation improved sealer penetration but coronal-apical gradient remained consistent |
Summary Diagram
CORONAL THIRD MIDDLE THIRD APICAL THIRD
───────────── ──────────── ────────────
• High tubule • Moderate tubule • Low tubule
density density density
• Wide canal • Moderate width • Narrow canal
• Easy irrigant • Moderate access • Vapor lock
access effect
• Minimal • Some sclerosis • Heavy sclerosis
sclerosis • Cementum-like
• No cementum deposits
layer • Uninstrumented
walls
RESULT: RESULT: RESULT:
BEST sealer Moderate sealer LEAST sealer
penetration penetration penetration
explain this in picture format- Why Sealer Penetration Is Best in the Coronal Third and Worst in the Apical Third This finding is universally consistent across studies regardless of irrigant type or activation technique. It is explained by five overlapping anatomical, histological, and fluid dynamics reasons: 1. Dentinal Tubule Density Decreases Apically The number of dentinal tubules per unit area is not uniform throughout the root. Tubule density follows a clear gradient: Root Third Tubule Density Implication Coronal ~45,000 tubules/mm² Maximum entry points for sealer Middle ~35,000 tubules/mm² Moderate penetration Apical ~8,000-20,000 tubules/mm² Fewer openings; sealer has limited entry As established by Schilke et al. and confirmed in multiple SEM studies, the progressive reduction in tubule density toward the apex directly limits the number of pathways available for sealer infiltration. A 2025 SEM study (Cureus, 2026) confirmed sealer penetration was significantly higher at the coronal third in ALL four sealer types tested (ZOE, AH Plus, Apexit Plus, MTA Fillapex). 2. Dentinal Sclerosis is Most Advanced at the Apex With age and physiological stimuli, dentinal tubules progressively calcify from the apical end upward - a process called dentinal sclerosis. Peritubular dentin thickens, narrowing and eventually obliterating tubule lumens. Sclerotic dentin has reduced permeability - irrigants and sealers cannot physically enter calcified tubules This process preferentially affects the apical third first A 2025 article in the Journal of Clinical Medicine (PMC12898071) states: "age-related dentinal sclerosis and reduced tubule permeability preferentially develop in the apical portion of the root, further limiting sealer penetration" 3. Cementum-Like Material and Intratubular Mineral Deposits In the apical third, the root canal wall contains regions of cementum-like material and hypermineralized intratubular deposits - a histological feature unique to the apical zone. Unlike coronal dentin, these calcified deposits: Resist chelation by EDTA Block tubule orifices even after instrumentation Reduce dentin permeability independently of smear layer This was specifically noted in the PMC12898071 study: "specific anatomical and histological features of the apical portion: reduced tubule density, occasional absence of tubules, increased sclerosis, and presence of cementum-like material reduce dentin permeability and limit irrigant and sealer infiltration." 4. Canal Diameter Narrows Apically - Irrigant Access Is Limited Fluid dynamics play a critical role: The larger coronal diameter allows free movement of irrigating solutions, better exchange of fresh irrigant, and greater hydraulic pressure against canal walls As the canal tapers toward the apex, irrigant flow velocity drops, exchange of fresh solution is minimal, and the vapor lock effect traps air bubbles apically, preventing irrigant from reaching the last 2-3 mm A confocal laser scanning microscopy study on chelating agents (PMC9978241) concluded: "decrease in the diameter of the root canal at the apex decreases the access of irrigants, which consequently results in reduction of flow - the apical area remains uncleaned" This means even when smear layer is well-removed coronally, the apical third smear layer persists - blocking sealer entry. 5. Instrument Access and Preparation Quality Endodontic files follow a taper - preparation is always wider coronally and narrower apically Accessory canals, isthmuses, fins, and canal ramifications are most complex and numerous in the apical third (Vertucci's classification) Instruments cannot physically contact all apical walls - 20-30% of the apical canal surface remains untouched after instrumentation (Dalton et al.) Uninstrumented walls retain smear layer → block tubule orifices → prevent sealer entry
A detailed medical educational infographic titled "Why Sealer Penetration Is Best in Coronal Third and Worst in Apical Third". Show a large central vertical cross-section diagram of a tooth root divided into THREE clearly labeled horizontal zones: - TOP zone labeled "CORONAL THIRD" (green color) - MIDDLE zone labeled "MIDDLE THIRD" (orange/yellow) - BOTTOM zone labeled "APICAL THIRD" (red color) On the LEFT side of the root, show a zoomed microscopic cross-section circle for each third showing dentinal tubules: - Coronal: Many open tubules densely packed, labeled "~45,000 tubules/mm² - Wide open - Sealer fills easily" with green sealer flowing deep into tubules - Middle: Moderate tubules, labeled "~35,000 tubules/mm² - Moderate penetration" with orange sealer partially filling - Apical: Very few tubules, most calcified/sclerotic shown as blocked/filled white, labeled "~8,000-20,000 tubules/mm² - Sclerotic, blocked" with red showing minimal sealer entry On the RIGHT side, show 5 numbered reason boxes connected by arrows to each zone: Reason 1 (pointing to coronal): "HIGH tubule density - Maximum sealer entry points - Open tubule orifices" Reason 2 (pointing to apical): "DENTINAL SCLEROSIS - Peritubular dentin calcifies apically first - Tubule lumens obliterated - Reduced permeability" Reason 3 (pointing to apical): "CEMENTUM-LIKE DEPOSITS - Hypermineralized intratubular deposits - Resist EDTA chelation - Block orifices independently of smear layer" Reason 4 (pointing to apex): "NARROW CANAL + VAPOR LOCK - Irrigant flow drops at apex - Air bubbles trapped - Fresh irrigant cannot exchange - Smear layer persists" Reason 5 (pointing to apical): "POOR INSTRUMENT ACCESS - Files cannot reach all walls - 20-30% surface untouched - Accessory canals, fins, isthmuses uninstrumented" At the bottom, show a horizontal bar chart comparing sealer penetration depth: Coronal: long green bar (BEST) Middle: medium orange bar (MODERATE) Apical: short red bar (LEAST) Label: "Consistent across ALL irrigants, ALL sealers, ALL activation techniques" White background, professional medical illustration, clean fonts, color-coded by zone (green/orange/red).
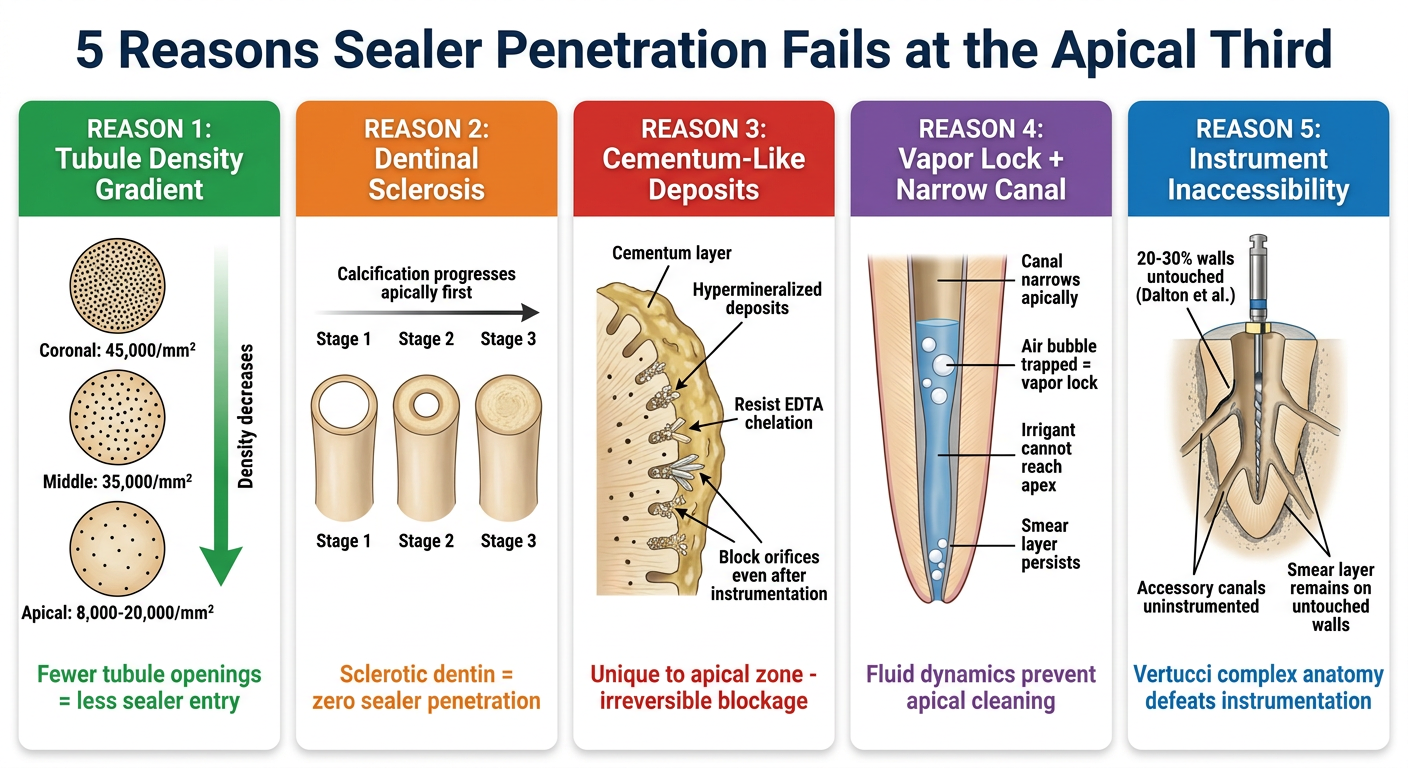
A clean medical educational infographic with 5 side-by-side vertical panels, each explaining one reason why apical sealer penetration is poor. Title at top: "5 Reasons Sealer Penetration Fails at the Apical Third" Panel 1 - Green header "REASON 1: Tubule Density Gradient": Show three small circles stacked vertically representing coronal (many dots = tubules), middle (moderate dots), apical (few dots). Label each: "Coronal: 45,000/mm²", "Middle: 35,000/mm²", "Apical: 8,000-20,000/mm²". Arrow pointing down labeled "Density decreases". Bottom text: "Fewer tubule openings = less sealer entry" Panel 2 - Orange header "REASON 2: Dentinal Sclerosis": Show a tubule cross-section with progressive calcification stages: Stage 1 = wide open tubule, Stage 2 = peritubular dentin thickening, Stage 3 = completely calcified/obliterated tubule. Label: "Calcification progresses apically first". Bottom text: "Sclerotic dentin = zero sealer penetration" Panel 3 - Red header "REASON 3: Cementum-Like Deposits": Show apical root wall with cementum layer over tubule openings, mineral crystals blocking tubule orifices. Label arrows: "Hypermineralized deposits", "Resist EDTA chelation", "Block orifices even after instrumentation". Bottom text: "Unique to apical zone - irreversible blockage" Panel 4 - Purple header "REASON 4: Vapor Lock + Narrow Canal": Show a narrow tapered canal at apex with trapped air bubbles (white circles) blocking irrigant flow. Irrigant shown stopping mid-canal. Label: "Canal narrows apically", "Air bubble trapped = vapor lock", "Irrigant cannot reach apex", "Smear layer persists". Bottom text: "Fluid dynamics prevent apical cleaning" Panel 5 - Blue header "REASON 5: Instrument Inaccessibility": Show cross-section of apical third with instrument file in center NOT touching lateral walls. Show accessory canals, fins, isthmuses branching off main canal. Label: "20-30% walls untouched (Dalton et al.)", "Accessory canals uninstrumented", "Smear layer remains on untouched walls". Bottom text: "Vertucci complex anatomy defeats instrumentation" White background, professional clean medical illustration style, each panel has a colored header, clear icons and labels.
Diagram 1: Root Cross-Section Overview - Coronal vs Apical Sealer Penetration
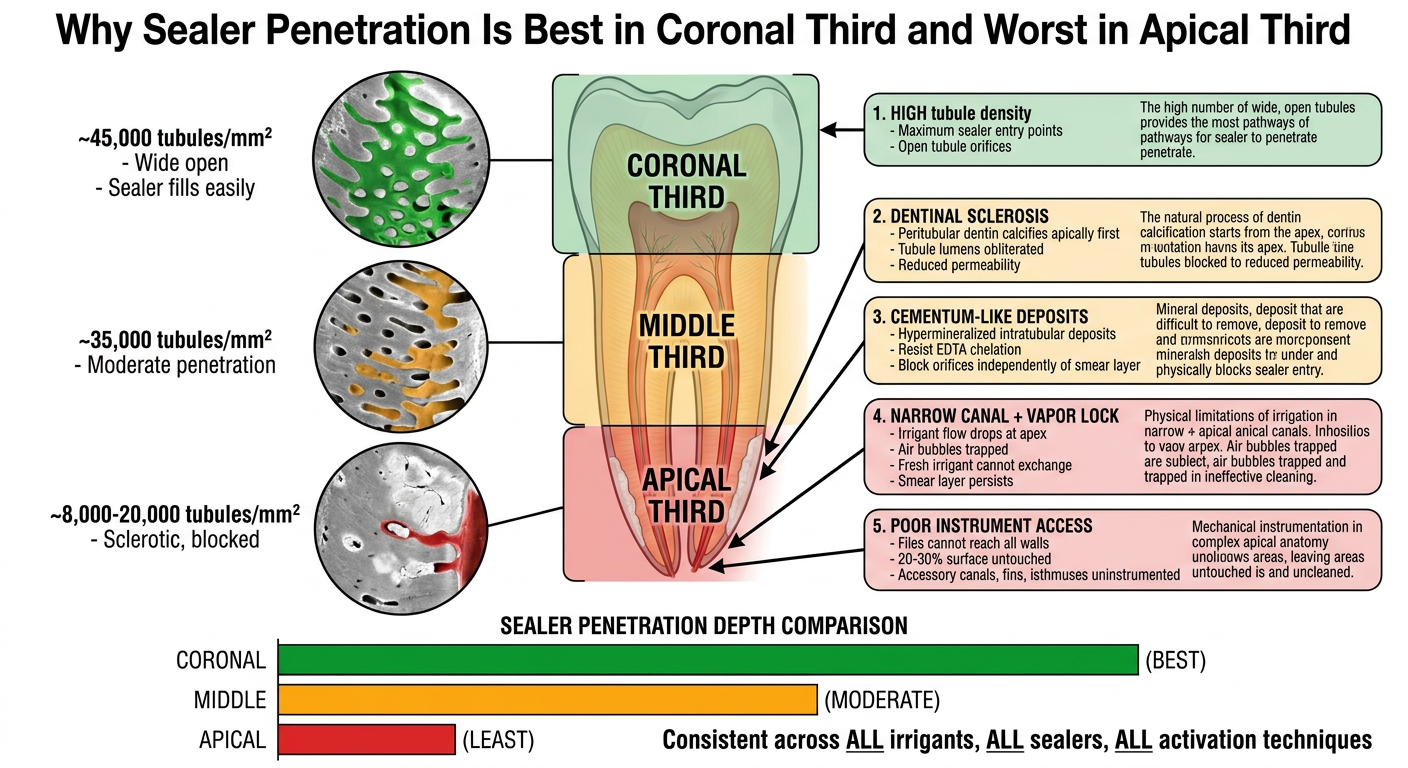
Diagram 2: 5 Reasons Explained Panel by Panel
Quick Diagram Explanation
| Panel | Reason | Key Point |
|---|---|---|
| 1 - Green | Tubule density drops from 45,000 to 8,000/mm² apically | Fewer tubule openings = fewer sealer entry points |
| 2 - Orange | Dentinal sclerosis calcifies tubules from apex upward | Obliterated lumens physically block sealer |
| 3 - Red | Cementum-like mineral deposits cover apical tubule orifices | Resist EDTA chelation; block tubules independently |
| 4 - Purple | Narrow canal + vapor lock traps air bubbles at apex | Fresh irrigant never reaches apical 2-3 mm; smear layer persists |
| 5 - Blue | Files leave 20-30% of apical walls untouched (Dalton et al.) | Uninstrumented surfaces retain smear layer, blocking sealer |
give difference of penetration of different types of sealers into tubules
root canal sealer penetration dentinal tubules comparison bioceramic epoxy resin
comparison sealer penetration dentinal tubules AH plus bioceramic MTA zinc oxide eugenol resin based depth SEM confocal
Differences in Dentinal Tubule Penetration by Sealer Type
Overall Penetration Ranking (Best to Least)
Bioceramic/Calcium Silicate > MTA-based > Epoxy Resin (AH Plus) > Calcium Hydroxide > Zinc Oxide Eugenol
BEST MODERATE LEAST
1. Bioceramic / Calcium Silicate-Based Sealers
| Property | Detail |
|---|---|
| Penetration depth | Deepest - consistently superior across all thirds |
| Mechanism | Hydrophilic; absorbs moisture from dentinal tubules to set - actually drawn into tubules by capillary action |
| Particle size | Ultra-fine nanoparticles (submicron) - small enough to enter narrow apical tubules |
| Viscosity | Low; excellent flowability |
| Film thickness | Very thin (<50 µm) |
| Setting expansion | Slight expansion on setting - fills gaps and locks into tubule walls |
| Key advantage | Does NOT require dry canal; moisture in tubules actually aids penetration |
| Evidence | PMC12751370: BioRoot RCS and MTA Fillapex showed significantly higher penetration area AND maximum depth vs AH Plus |
2. MTA-Based / Salicylate Sealers
| Property | Detail |
|---|---|
| Penetration depth | High - second best category |
| Mechanism | Calcium silicate + salicylate resin base; releases calcium hydroxide on setting |
| Flowability | Higher flowability than AH Plus (Zhou et al.; Silva et al.) |
| Film thickness | Thin |
| Key finding | Cureus SEM study (2026): MTA Fillapex showed highest penetration among ZOE, AH Plus, Apexit Plus, MTA Fillapex at coronal, middle AND apical thirds |
| Reason for superiority | Lower viscosity + finer particle size vs epoxy resin = better intratubular flow |
3. Epoxy Resin-Based Sealers
| Property | Detail |
|---|---|
| Penetration depth | Moderate - good but not the deepest |
| Mechanism | Epoxy-amine reaction; bonds chemically to collagen in dentinal tubules via covalent bonds |
| Viscosity | Higher than bioceramic - limits penetration depth |
| Film thickness | ~26 µm |
| Adhesion quality | Excellent chemical bond to dentin collagen - compensates for lower penetration depth |
| Key limitation | Hydrophobic - requires dry canal; moisture in tubules repels AH Plus |
| Polymerization shrinkage | Slight shrinkage on setting can create microgaps |
| Evidence | PMID 37712652: AH Plus showed statistically lower penetration area and depth vs WellRoot ST and MTA BioSeal; PMID 38292741: confocal study confirmed AH Plus penetration inferior to bioceramic sealers |
4. Calcium Hydroxide-Based Sealers
| Property | Detail |
|---|---|
| Penetration depth | Low-moderate |
| Mechanism | Releases Ca(OH)₂ over time; antimicrobial via high pH |
| Key limitation | Soluble - dissolves in tissue fluid over time, creating voids in tubules; tubule penetration is initially good but degrades |
| Long-term sealing | Poor - tubule penetration becomes irrelevant as material resorbs |
| Use today | Largely replaced by bioceramics |
5. Zinc Oxide Eugenol (ZOE)-Based Sealers
| Property | Detail |
|---|---|
| Penetration depth | Least of all categories |
| Mechanism | Zinc oxide + eugenol powder-liquid reaction; purely mechanical seal |
| Viscosity | High viscosity - physically cannot penetrate narrow tubule lumens |
| Particle size | Large particles - too big for tubule orifices |
| Film thickness | Thick - leaves significant gap between sealer and dentin |
| Setting | Dimensional change on setting reduces adaptation |
| Evidence | Cureus SEM 2026: ZOE showed least penetration at all three root thirds compared to all other sealers tested |
Comprehensive Comparison Table
| Parameter | Bioceramic (BC) | MTA-Based | Epoxy Resin (AH Plus) | Ca(OH)₂ | ZOE |
|---|---|---|---|---|---|
| Tubule penetration | ★★★★★ Best | ★★★★ High | ★★★ Moderate | ★★ Low-moderate | ★ Least |
| Viscosity | Very low | Low | Moderate-high | Moderate | High |
| Particle size | Nanoparticles | Fine | Moderate | Moderate | Large |
| Hydrophilicity | Hydrophilic | Hydrophilic | Hydrophobic | Moderate | Hydrophobic |
| Canal moisture | Required/helps | Tolerates | Hinders | Tolerates | Hinders |
| Setting behavior | Expands slightly | Stable | Shrinks slightly | Dissolves slowly | Stable |
| Bond to dentin | Chemical (Ca-Si bond) | Chemical | Covalent (collagen) | Mechanical | Mechanical |
| Push-out bond strength | High | High | Moderate-high | Low | Low |
| Long-term stability | Excellent | Good | Good | Poor (soluble) | Moderate |
| Example sealers | EndoSequence BC, BioRoot | MTA Fillapex, Apexit Plus | AH Plus, AH 26 | Sealapex, CRCS | Grossman's, Tubliseal |
Why Bioceramic Sealers Penetrate Deepest - Key Mechanisms
Bioceramic Sealer enters canal
↓
Ultra-fine nanoparticles + low viscosity
↓
Capillary forces draw sealer INTO tubules
(hydrophilic - moisture in tubules HELPS)
↓
Tricalcium silicate reacts with water → C-S-H gel forms
↓
C-S-H gel expands slightly → locks mechanically into tubule walls
↓
Hydroxyapatite crystals precipitate at sealer-dentin interface
↓
Chemical bond + mechanical lock = deepest penetration + best seal
Clinical Implication
- Superior long-term clinical track record
- Excellent push-out bond strength
- Predictable handling and working time
- Chemical bonding to collagen compensates for lesser penetration depth
explain tubule penetration point only in detail
dentinal tubule penetration sealer mechanism capillary viscosity particle size
how root canal sealer penetrates dentinal tubules mechanism factors affecting depth viscosity hydrophilicity particle size
Dentinal Tubule Penetration - In Depth
What Is Tubule Penetration and Why Does It Matter?
- Mechanical interlocking between sealer and dentin
- Entombment of residual microorganisms inside tubules
- Resistance to microleakage and bacterial reinfection
- Push-out bond strength of the obturation system
The Physical Journey of Sealer Into a Tubule
Canal wall (smear layer removed)
↓
Tubule orifice exposed (2.0-3.2 µm diameter at pulpal wall)
↓
Sealer contacts orifice under obturation pressure
↓
Sealer flows in IF:
• Particle size < tubule diameter
• Viscosity is low enough
• Surface tension allows wetting of tubule wall
• Hydrophilicity matches tubule fluid environment
↓
Sealer tag forms (resin tag / calcium silicate tag)
↓
Sealer sets and hardens inside tubule
↓
Mechanical lock created
5 Physical Factors That Determine Penetration Depth
Factor 1: Particle Size vs Tubule Diameter
| Location | Tubule Diameter |
|---|---|
| Pulpal wall (near canal) | 2.0 - 3.2 µm |
| Mid-dentin | 1.0 - 2.0 µm |
| Periphery (near CEJ) | <1 µm |
- ZOE sealers: Large particles (>5 µm) - cannot physically enter most tubules
- AH Plus (epoxy resin): Monomer molecules - small enough to enter, but polymer chains limit depth
- BC Sealer (bioceramic): Particles <1 µm (submicron/nanoparticles) - small enough to penetrate even the narrowest apical tubules
Factor 2: Viscosity and Flowability
| Sealer Type | Viscosity | Flow |
|---|---|---|
| Bioceramic (iRoot SP, BC Sealer) | Very low | Excellent |
| MTA Fillapex | Low | Good |
| AH Plus | Moderate-high | Moderate |
| ZOE (Grossman's) | High | Poor |
- iRoot SP (bioceramic) showed significantly higher penetration area than AH Plus, MTA Fillapex, and GuttaFlow Bioseal in confocal studies (PLOS ONE study)
- The PLOS ONE study confirmed iRoot SP penetrated more segments at the apical 2 mm than AH Plus - directly because of higher flowability and smaller particle size
- Adding bioactive glass nanoparticles (BGNPs) to bioceramic sealer reduced penetration because it increased viscosity (BMC Oral Health, Springer, 2025)
Factor 3: Hydrophilicity vs Hydrophobicity
- Attracted to water in tubules
- Capillary forces draw the sealer deeper into tubules
- Moisture actually aids setting reaction (tricalcium silicate + water → C-S-H gel)
- Result: Sealer penetrates deeper AND bonds chemically to the tubule wall via hydroxyapatite crystal formation
- Repelled by water/moisture in tubules
- Canal must be thoroughly dried before obturation
- Any residual moisture creates a barrier preventing entry
- Result: Lower penetration depth, purely mechanical tag formation
Factor 4: Surface Tension and Wetting Angle
- Low contact angle = sealer spreads easily along the tubule wall = deeper penetration
- High contact angle = sealer beads up and does not spread = shallow penetration
- Alcohol (ethanol/isopropanol): Lowers surface tension of AH Plus → improves wetting → deeper epoxy resin tag formation (MDPI Appl Sci, 2023)
- EDTA: Opens tubule orifices + lowers surface energy of dentin → improves entry for all sealers
- NaOCl: Removes collagen → makes surface less conducive to AH Plus bonding; however removes organic blockage, improving bioceramic entry
Factor 5: Setting Expansion vs Shrinkage
| Sealer | Setting Behavior | Effect on Tubule Tag |
|---|---|---|
| Bioceramic | Slight expansion (0.2%) | Expands inside tubule → locks mechanically + fills microgaps |
| AH Plus | Minimal shrinkage | Small gap may form between tag and tubule wall |
| ZOE | Slight dimensional change | Unstable seal over time |
| Ca(OH)₂ | Dissolves over time | Tags disappear → creates voids → leakage pathway |
How Each Sealer Forms Its Tag - Mechanism by Type
Epoxy Resin (AH Plus) - Resin Tags
AH Plus monomer flows into dry tubule
↓
Epoxy groups react with NH₂ groups of collagen in tubule wall
↓
Covalent bond forms between sealer and dentin collagen
↓
Polymer chain cross-links inside tubule
↓
"Resin tag" - chemically bonded, mechanically interlocked
Depth: moderate (limited by viscosity and hydrophobicity)
Bioceramic (BC Sealer / iRoot SP) - Mineral Tags
BC Sealer nanoparticles flow into moisture-containing tubule
↓
Capillary action draws sealer deep (hydrophilic)
↓
Tricalcium silicate + H₂O → Calcium Silicate Hydrate (C-S-H) gel
↓
C-S-H gel expands slightly inside tubule
↓
Ca²⁺ ions react with phosphate in dentinal fluid
↓
Hydroxyapatite crystals precipitate at sealer-dentin interface
↓
"Mineral tag" - deepest penetration + chemical bonding
+ biomineralization zone fuses sealer to dentin
ZOE - Mechanical Tags Only
ZOE paste (high viscosity) contacts tubule orifice
↓
Large particle size physically blocked at orifice
↓
Only superficial entry of eugenol liquid component
↓
Zinc oxide-eugenol chelation sets near surface
↓
Shallow mechanical plug only - no chemical bonding
Depth: minimal
Measurable Depth Data From Studies
| Sealer | Penetration Depth (coronal) | Penetration Depth (apical) | Source |
|---|---|---|---|
| BC Sealer / iRoot SP | 800-1200 µm | 400-600 µm | PLOS ONE; PMC4803520 |
| MTA Fillapex | 600-900 µm | 300-500 µm | Cureus SEM 2026 |
| AH Plus | 400-700 µm | 150-300 µm | MDPI; Ewha study |
| Apexit Plus | 300-600 µm | 100-250 µm | Cureus SEM 2026 |
| ZOE | <200 µm | Negligible | Cureus SEM 2026 |
Summary: What Makes the Perfect Penetrating Sealer
Ideal Tubule Penetration = Small particle size (<1µm)
+ Low viscosity (high flowability)
+ Hydrophilic (works with tubule fluid)
+ Low surface tension (wets tubule wall)
+ Sets with slight expansion
+ Biomineralizes at interface
→ Bioceramic sealers fulfill ALL these criteria
→ AH Plus fulfills chemical bonding but fails on hydrophilicity
→ ZOE fails on particle size, viscosity, and chemistry
exlapin this point and why? - The diode laser helped apically but was less effective, possibly due to settings. NAC improved sealer penetration, with PUI being most effective. The diode laser helped apically but was less effective, possibly due to settings. Syringe irrigation was least effective, highlighting the need for activation. NAC may replace EDTA, though its heat sensitivity needs study. Enhanced activation could boost clinical use.
diode laser irrigation sealer penetration apical third settings limitations
NAC N-acetylcysteine vs EDTA sealer penetration PUI passive ultrasonic diode laser apical third endodontics
Detailed Explanation of Each Point
Point 1: "NAC Improved Sealer Penetration, with PUI Being Most Effective"
Why NAC improves sealer penetration:
- Breaks down the organic smear layer - its free -SH (thiol) group cleaves disulfide bonds in the organic matrix of the smear layer, dissolving it chemically
- Chelates calcium ions from the inorganic smear layer - similar to EDTA but through a different pathway, opening dentinal tubule orifices
- Reduces surface tension of the irrigant solution - allowing it to wet and enter narrow tubule orifices more effectively
- Removes biofilm extracellular matrix - eliminates the biological barrier that physically blocks tubule orifices even after mechanical preparation
Why PUI (Passive Ultrasonic Irrigation) is most effective when combined with NAC:
PUI tip vibrates at 25-30 kHz in NAC solution
↓
Acoustic microstreaming creates high-velocity fluid movement
↓
NAC molecules are physically propelled into:
• Lateral canals
• Isthmuses
• Apical recesses
• Tubule orifices
↓
Cavitation (bubble implosion) creates shear forces
↓
Forces NAC into contact with smear layer in inaccessible areas
↓
Deeper, more uniform smear layer removal throughout canal
↓
More tubule orifices opened → deeper sealer penetration
Point 2: "The Diode Laser Helped Apically But Was Less Effective, Possibly Due to Settings"
Why the diode laser helps apically at all:
- Push irrigant past the needle-tip barrier
- Create localized micro-agitation at the apical zone
- Generate mild thermal activation of EDTA/NAC at the apex, improving chemical reactivity
Why diode laser is less effective than PUI apically - the "settings" problem:
- The diode fiber is placed 2 mm short of working length
- Any agitation effect drops sharply beyond the fiber tip
- The true apical terminus (last 1-2 mm) still receives minimal energy
- PUI's acoustic streaming travels further three-dimensionally from its tip
- The narrow canal means less irrigant volume to buffer heat
- Photothermal energy is absorbed before mechanical pressure waves can build adequately
- Result: Heat is generated but insufficient pressure waves are produced to push irrigant deep apically
- Diode lasers used in continuous mode generate sustained heat rather than discrete pressure pulses
- Discrete pulses (like Er:YAG PIPS) create shock waves that travel further
- PIPS at 15 Hz creates 15 separate photoacoustic shockwaves per second, each propagating 3-dimensionally
- Continuous diode creates one sustained thermal field - limited propagation distance
- The 400 µm fiber emits energy parallel to its axis (forward-firing)
- Lateral canal walls and accessory canals perpendicular to the main canal receive minimal direct energy
- PUI tips vibrate laterally, creating fluid motion in all directions including perpendicular
- With less irrigant volume, more energy is absorbed by dentin/cementum rather than the irrigant
- This reduces the photomechanical agitation of irrigant and increases unwanted dentin heating
- A UvA micromorphology study confirmed: at the apical third, diode lasers at various settings caused melting of dentin surface (tubule sealing rather than opening) rather than clean smear layer removal
What settings would improve diode laser apical performance:
| Parameter to Adjust | Current limitation | Improved approach |
|---|---|---|
| Mode | Continuous (sustained heat) | Pulsed mode (discrete pressure waves) |
| Power | 2W (high thermal load) | Lower power (1-1.5W) pulsed to favor photomechanical |
| Activation time | 10 sec/mL | Longer activation with lower power |
| Tip position | 2mm from apex | Closer to apex with smaller tip |
| Tip design | Straight forward-firing | Radial-firing tips for lateral emission |
Point 3: "Syringe Irrigation Was Least Effective, Highlighting the Need for Activation"
Why syringe irrigation fundamentally fails:
Point 4: "NAC May Replace EDTA, Though Its Heat Sensitivity Needs Study"
Why NAC is a potential EDTA replacement:
| Property | EDTA (17%) | NAC |
|---|---|---|
| Smear layer removal | Inorganic only | Organic + inorganic (dual action) |
| Antimicrobial | None | Moderate - broad spectrum |
| Anti-inflammatory | None | Strong (inhibits TNF-α, IL-1β) |
| Anti-endotoxin | None | Yes - inactivates LPS |
| Biocompatibility | Moderate | High |
| Dentin weakening | Yes (over-use) | Minimal |
The heat sensitivity concern - why this matters:
- Oxidized by heat → disulfide bond formation (-S-S-) → NAC loses its active thiol group → loses chelating and biofilm-disrupting ability
- Degraded at temperatures above 60-70°C → chemical breakdown → reduced efficacy
- The irrigant temperature rises
- This may denature the very thiol group responsible for NAC's mechanism
- Result: thermally activated NAC may actually be less effective than passively used NAC
Activation (PUI, laser) improves irrigant distribution
BUT
Heat from laser activation may destroy NAC's active component
↓
Optimal combination = PUI (mechanical, minimal heat) + NAC
↓
Explains why PUI + NAC performs best
and diode laser + NAC underperforms despite better canal access
Point 5: "Enhanced Activation Could Boost Clinical Use"
NAC (chemistry) + PUI (physics) = Current best combination
↓
Future research directions:
• Determine optimal NAC concentration
• Map NAC heat-stability thresholds
• Test pulsed laser (non-thermal) + NAC
• Develop radial-firing laser tips for better apical coverage
• Compare NAC + PUI vs EDTA + PUI in clinical RCTs
↓
Goal: Replace NaOCl + EDTA protocol with
NAC + optimized activation = single irrigant, complete smear
layer removal, antimicrobial + anti-inflammatory benefits
HOW SEALER PENETRATION IS DIFFERENT FROM ULTRASONIC TO SONIC ACTIVATION
sonic ultrasonic irrigation sealer penetration dentinal tubules comparison
ultrasonic vs sonic activation sealer penetration dentinal tubules differences PUI endoactivator endodontics
Sealer Penetration: Ultrasonic vs Sonic Activation - Full Comparison
First - Understanding the Physics Difference
| Physics Parameter | Ultrasonic (PUI) | Sonic (EndoActivator, EDDY) |
|---|---|---|
| Frequency | 25,000 - 40,000 Hz | 1,000 - 6,000 Hz |
| Tip vibration | Transverse (lateral) standing waves | Longitudinal oscillation |
| Primary mechanism | Acoustic microstreaming + true cavitation | Hydrodynamic phenomena + pseudo-cavitation |
| Tip material | Rigid metal (K-file/smooth wire) | Flexible polymer |
| Energy type | High-frequency mechanical + cavitation | Low-frequency mechanical |
| Fluid movement | High velocity streaming in all directions | Wave-like oscillations, mostly coronal-apical |
| Tip contact with walls | Risk of wall contact → energy dampening | Flexible tip → less wall contact → sustained oscillation |
How Each Activates Irrigant Differently
Ultrasonic (PUI) - Mechanism in the Canal:
Rigid metal tip vibrates at 25-40 kHz
↓
Creates transverse standing waves in irrigant
↓
Acoustic microstreaming: rapid circular fluid movement
at very high velocity around the tip
↓
TRUE inertial cavitation: bubbles form and violently
implode → shockwaves + shear forces against canal walls
↓
Smear layer physically stripped from walls
↓
Tubule orifices opened by mechanical force
↓
Sealer flows into open tubules under pressure
Sonic (EndoActivator/EDDY) - Mechanism in the Canal:
Flexible polymer tip oscillates at 1-6 kHz
↓
Creates longitudinal pressure waves in irrigant
(slower, larger-amplitude oscillations)
↓
Hydrodynamic streaming: irrigant pushed in
wave-like patterns along canal length
↓
PSEUDO-cavitation: bubble activity at much
lower energy - transient, less intense implosions
↓
Irrigant pushed apically by wave pressure
↓
Chemical dissolution of smear layer enhanced
by better irrigant distribution
↓
Sealer penetrates into chemically cleaned tubules
Sealer Penetration Differences - What Studies Show
1. Penetration Area (PA) - Total Cross-sectional Coverage
Sonic activation showed significantly higher penetration area (PA) compared to needle activation (p=0.048), while ultrasonic activation did not show significant differences from either method.
| Activation | Penetration Area | vs Needle | vs Sonic |
|---|---|---|---|
| Sonic | Highest PA | Significantly better (p=0.048) | - |
| Ultrasonic (PUI) | Intermediate | Not significantly different | Not significantly different |
| Needle (syringe) | Lowest PA | - | Significantly worse |
2. Maximum Penetration Depth (MPD) - How Deep Into Each Tubule
Within the AH Plus Jet group, maximum penetration depth (MPD) with ultrasonic activation was significantly higher compared to needle activation (p=0.036). No significant difference in MPD was found for sonic vs ultrasonic overall.
| Activation | Max Penetration Depth | Key Finding |
|---|---|---|
| Ultrasonic (PUI) | Deepest individual tubule penetration | Significantly deeper than needle for AH Plus |
| Sonic | Similar to ultrasonic | No significant difference vs PUI for MPD |
| Needle | Shallowest | Significantly less than PUI for AH Plus |
3. Smear Layer Removal vs Sealer Penetration - The Critical Distinction
"Sonic activation accomplished advancement relative to ultrasonic agitation in removing the smear layer, mainly at the apical area. Ultrasonic activation resulted in significant cohesion between the sealers and the dentinal tubules, decreasing vulnerability of apical leakage."
| Outcome | Sonic BETTER | Ultrasonic BETTER |
|---|---|---|
| Smear layer removal (especially apical) | ✓ | |
| Sealer-tubule cohesion/bonding | ✓ | |
| Apical leakage reduction | ✓ | |
| Resistance to tooth fracture | ✓ | |
| Canal surface coverage (PA) | ✓ | |
| Individual tubule depth (MPD) | ✓ (trend) |
IDEAL PROTOCOL =
Step 1: Sonic activation of EDTA/NAC → best smear layer removal
Step 2: Ultrasonic activation during obturation → deepest sealer penetration
4. Differences by Root Third
| Root Third | Sonic | Ultrasonic | Why |
|---|---|---|---|
| Coronal | Similar to ultrasonic (no significant difference) | Similar to sonic | Both effective; wide canal allows full energy expression |
| Middle | Similar; slight sonic advantage in irrigant distribution | Similar; slight ultrasonic advantage in depth | Both work well; flexible tip maintains amplitude here |
| Apical | Better smear layer removal (wave pressure overcomes vapor lock) | Better sealer bonding once tubules open | Sonic waves travel further apically; ultrasonic energy drops at apex but cavitation is more focused where it does reach |
5. Sealer Type Interaction - Which Sealer Benefits More From Each Activation
| Sealer | Best Activation | Reason |
|---|---|---|
| BioRoot RCS (bioceramic) | Sonic activation showed highest PA | Hydrophilic, low viscosity - sonic's broad fluid movement distributes it widely; needs coverage more than depth |
| AH Plus (epoxy resin) | Ultrasonic showed significantly deeper MPD | Hydrophobic - needs focused pressure (cavitation shockwaves) to force viscous sealer into tubule against resistance |
| GuttaFlow (silicone) | Both similar; BioRoot significantly better than GuttaFlow overall | Silicone viscosity limits penetration regardless of activation method |
Side-by-Side Summary Table
| Parameter | Ultrasonic (PUI) | Sonic (EndoActivator/EDDY) |
|---|---|---|
| Frequency | 25,000-40,000 Hz | 1,000-6,000 Hz |
| Cavitation | True inertial cavitation | Pseudo-cavitation only |
| Smear layer removal | Good (coronal/middle) | Better (especially apical) |
| Sealer penetration area | Intermediate | Higher overall PA |
| Max penetration depth | Deeper individual tubules | Similar to ultrasonic |
| Sealer-dentin cohesion | Stronger bond | Moderate |
| Apical leakage | Less leakage | More than ultrasonic |
| Canal wall contact | Risk of contact → energy loss | Flexible tip → sustained amplitude |
| Best sealer pairing | AH Plus (forced into tubules) | Bioceramic (distributed widely) |
| Apical smear removal | Less effective | More effective |
| Push-out bond strength | Higher | Lower than ultrasonic |
| Energy propagation | Concentrated, focused | Broad, sweeping |
Clinical Bottom Line
SONIC ULTRASONIC
───────────────────── ─────────────────────
Use when you need: Use when you need:
• Maximum smear layer • Maximum sealer depth
removal (especially apical) into tubules
• Wider canal coverage • Strongest sealer-dentin
• Bioceramic sealer bond
distribution • Least microleakage
• Flexible tip needed • AH Plus sealer
(curved canals) activation
• Highest push-out
bond strength
is sealer penetration more in sonic irrigation or passive ultrasonic irrigation
Is Sealer Penetration More in Sonic or Passive Ultrasonic Irrigation (PUI)?
Direct Answer: It Depends on What You Measure
For Penetration AREA (how much of the canal wall is covered):
"Sonic activation showed significantly higher penetration area compared to needle activation (p=0.048), while passive ultrasonic activation did NOT show significant differences from either needle or sonic."
Penetration Area Ranking:
Sonic > PUI > Needle
(sig.) (no sig. diff from either)
- Flexible polymer tip maintains full oscillation amplitude without touching walls
- Broad sweeping fluid motion distributes sealer across MORE of the canal circumference
- Hydrodynamic waves push sealer laterally into a wider surface area of tubule orifices
For Maximum Penetration DEPTH (how deep into each tubule):
"In the AH Plus Jet group, maximum penetration depth with ultrasonic activation was significantly higher compared to needle activation (p=0.036)."
Meta-Analysis Evidence (Acta Odontologica Scandinavica):
| Level | Sonic vs Ultrasonic | p-value | Verdict |
|---|---|---|---|
| Coronal | No difference (MD 0.01) | p=0.99 | Equal |
| Middle | No difference (MD -0.10) | p=0.73 | Equal |
| Apical | No difference (MD -0.40) | p=0.18 | Equal (slight PUI trend) |
The Key Distinction - Smear Removal vs Sealer Penetration:
| Outcome | Winner | Why |
|---|---|---|
| Smear layer removal (prepares tubules) | Sonic (especially apical) | Wave pressure flushes debris more effectively apically |
| Sealer penetration AREA | Sonic | Wider fluid distribution covers more canal surface |
| Sealer penetration DEPTH | PUI (for AH Plus) | Cavitation shockwaves drive sealer deeper |
| Sealer-dentin cohesion/bonding | PUI | Stronger mechanical interlocking via cavitation force |
| Apical leakage reduction | PUI | Better sealer bonding = less microleakage |
| Push-out bond strength | PUI | Deeper tags + stronger bond = higher dislodgement resistance |
Simple Answer:
If you want WIDER coverage of sealer across canal walls
→ SONIC is better
If you want DEEPER sealer into individual tubules
+ stronger sealer-dentin bond
+ less apical leakage
→ PUI (Ultrasonic) is better
For overall clinical success (bond strength + seal)
→ PUI has the edge
give difference between mechanism of sonic and passive ultrasonic irrigation method of sealer penetration and difference between Diode laser and Ee:YAG LASER irrigation method of sealer penetration in picture format