Spinal cord and reflex arc detail information about spinal cord and reflex arc
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive, authoritative information and excellent diagrams from multiple medical textbooks. Let me compile the complete answer.
Spinal Cord and Reflex Arc - Detailed Information
Sources: Gray's Anatomy for Students, Costanzo Physiology 7th Ed., Ganong's Review of Medical Physiology 26th Ed., Neuroanatomy through Clinical Cases 3rd Ed., Medical Physiology
PART 1: THE SPINAL CORD
1. Overview and Location
The spinal cord is the most caudal portion of the CNS. It extends from the foramen magnum down to approximately the disc between vertebrae L1 and L2 in adults (it can end as high as T12 or as low as L2-L3). In neonates, it extends to approximately L3 (sometimes reaching L4). The distal cone-shaped end is called the conus medullaris, from which a fine connective tissue filament called the filum terminale (pial part) continues inferiorly.
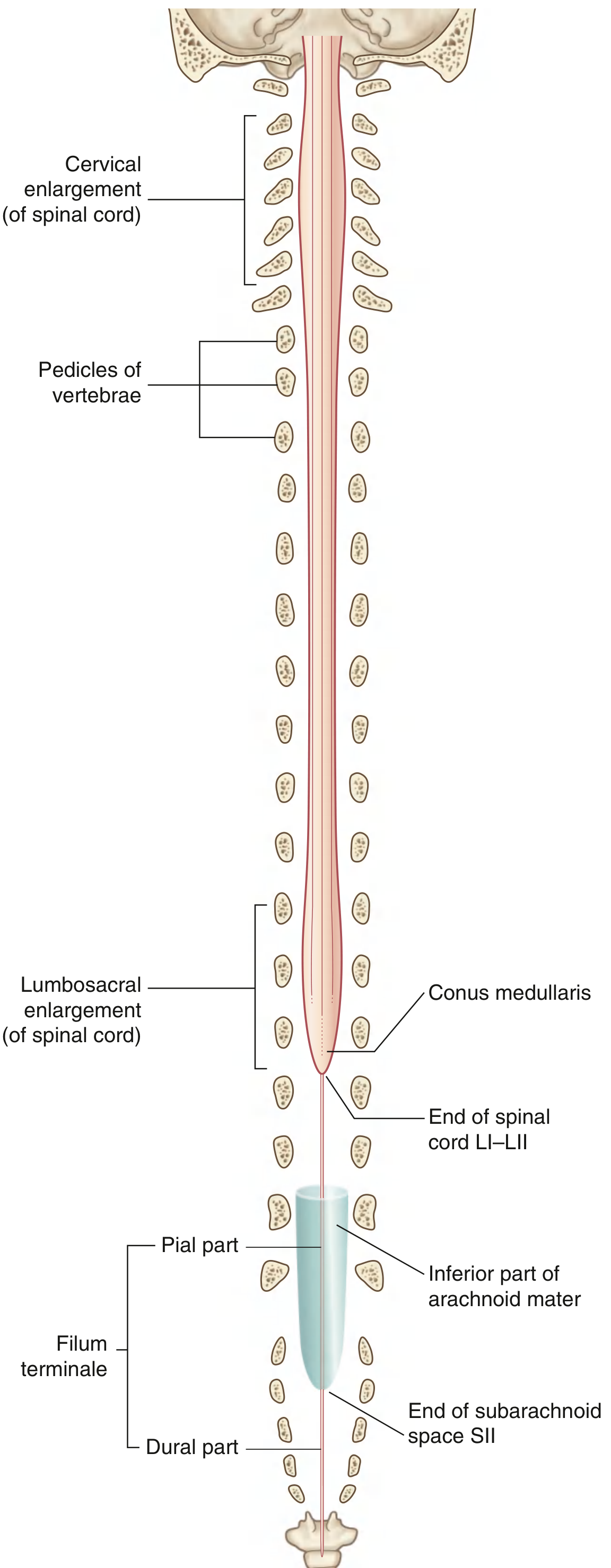
The spinal cord has 31 pairs of spinal nerves (8 cervical, 12 thoracic, 5 lumbar, 5 sacral, 1 coccygeal) containing both sensory (afferent) and motor (efferent) nerves.
2. Enlargements
The cord is not uniform in diameter:
| Enlargement | Segments | Innervates |
|---|---|---|
| Cervical enlargement | C5 to T1 | Upper limbs |
| Lumbosacral enlargement | L1 to S3 | Lower limbs |
The white matter is thickest in the cervical region (where most ascending fibers have entered and descending fibers have not yet terminated). The sacral cord is mostly gray matter.
3. External Surface Features
The external surface carries several longitudinal grooves:
- Anterior median fissure - extends the full length of the anterior surface
- Posterior median sulcus - along the posterior surface
- Posterolateral sulcus (each side) - where posterior rootlets of spinal nerves enter
4. Internal Structure - Gray and White Matter
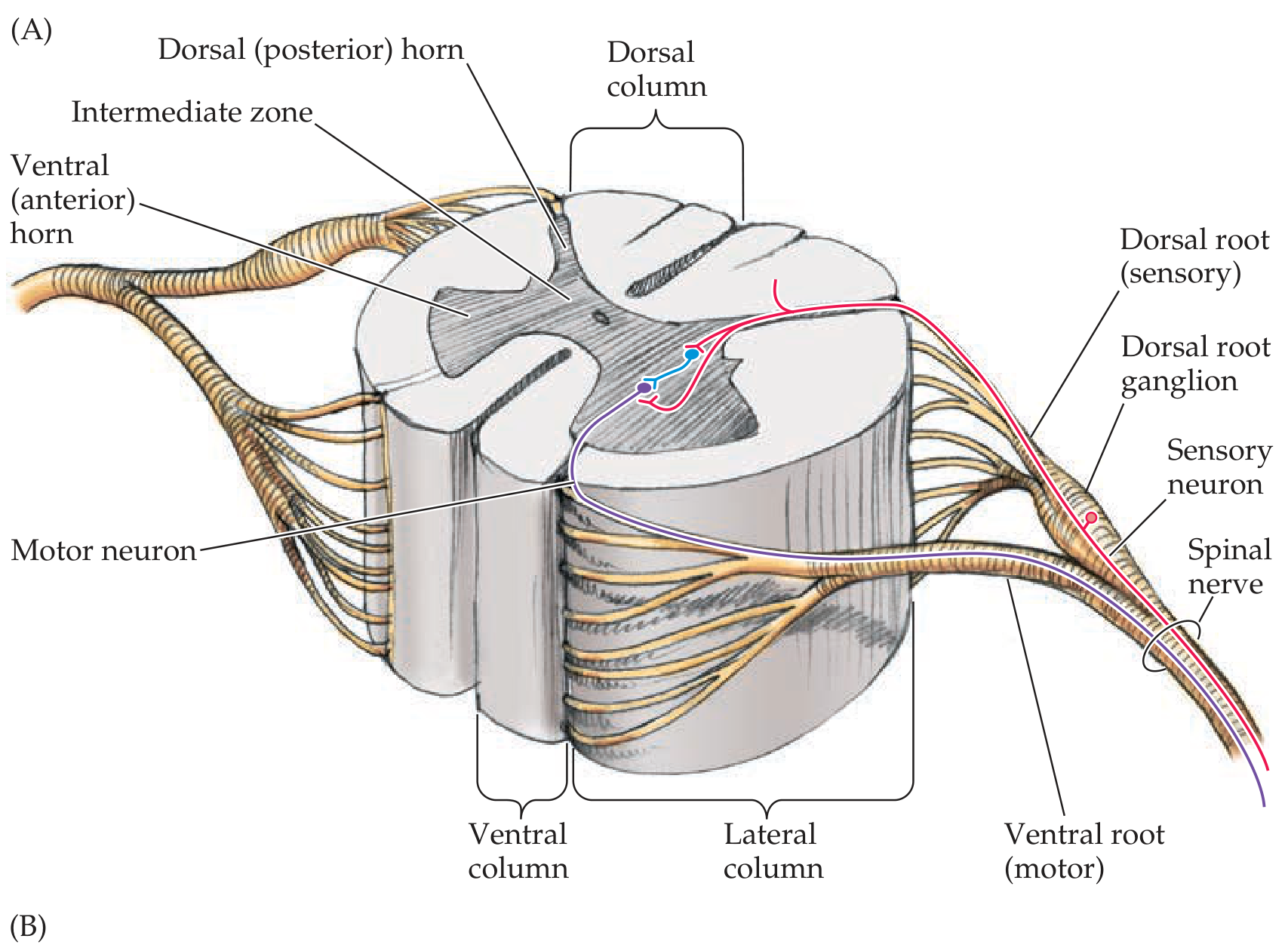
Gray Matter (H-shaped, butterfly appearance)
Rich in nerve cell bodies, forming longitudinal columns. In cross-section it shows:
- Dorsal (posterior) horn - mainly involved in processing sensory input
- Ventral (anterior) horn - contains lower motor neurons (alpha and gamma motoneurons) that innervate skeletal muscle
- Intermediate zone - contains Clarke's nucleus (spinocerebellar relay) and intermediolateral nucleus (autonomic preganglionic neurons)
Rexed's Laminae - The gray matter is organized into 10 functional layers (Rexed's laminae):
| Region | Nucleus | Laminae |
|---|---|---|
| Dorsal horn | Marginal zone | I |
| Dorsal horn | Substantia gelatinosa | II |
| Dorsal horn | Nucleus proprius | III, IV |
| Dorsal horn | Neck of dorsal horn | V |
| Dorsal horn | Base of dorsal horn | VI |
| Intermediate zone | Clarke's nucleus, intermediolateral nucleus | VII |
| Ventral horn | Commissural nucleus | VIII |
| Ventral horn | Motor nuclei | IX |
| Around central canal | Commissural cells | X |
White Matter
Surrounds the gray matter and is rich in myelinated nerve fiber tracts. Organized into three columns on each side:
- Dorsal (posterior) columns
- Lateral columns
- Ventral (anterior) columns
5. Spinal Nerve Roots
Every spinal nerve is formed by the joining of:
- Dorsal root (sensory/afferent) - carries information FROM the periphery (skin, joints, muscles, viscera) INTO the cord; cell bodies located in the dorsal root ganglion (DRG)
- Ventral root (motor/efferent) - carries motor information FROM the cord TO the periphery; includes somatic motor nerves (to skeletal muscle) and autonomic motor nerves
6. Ascending and Descending Tracts
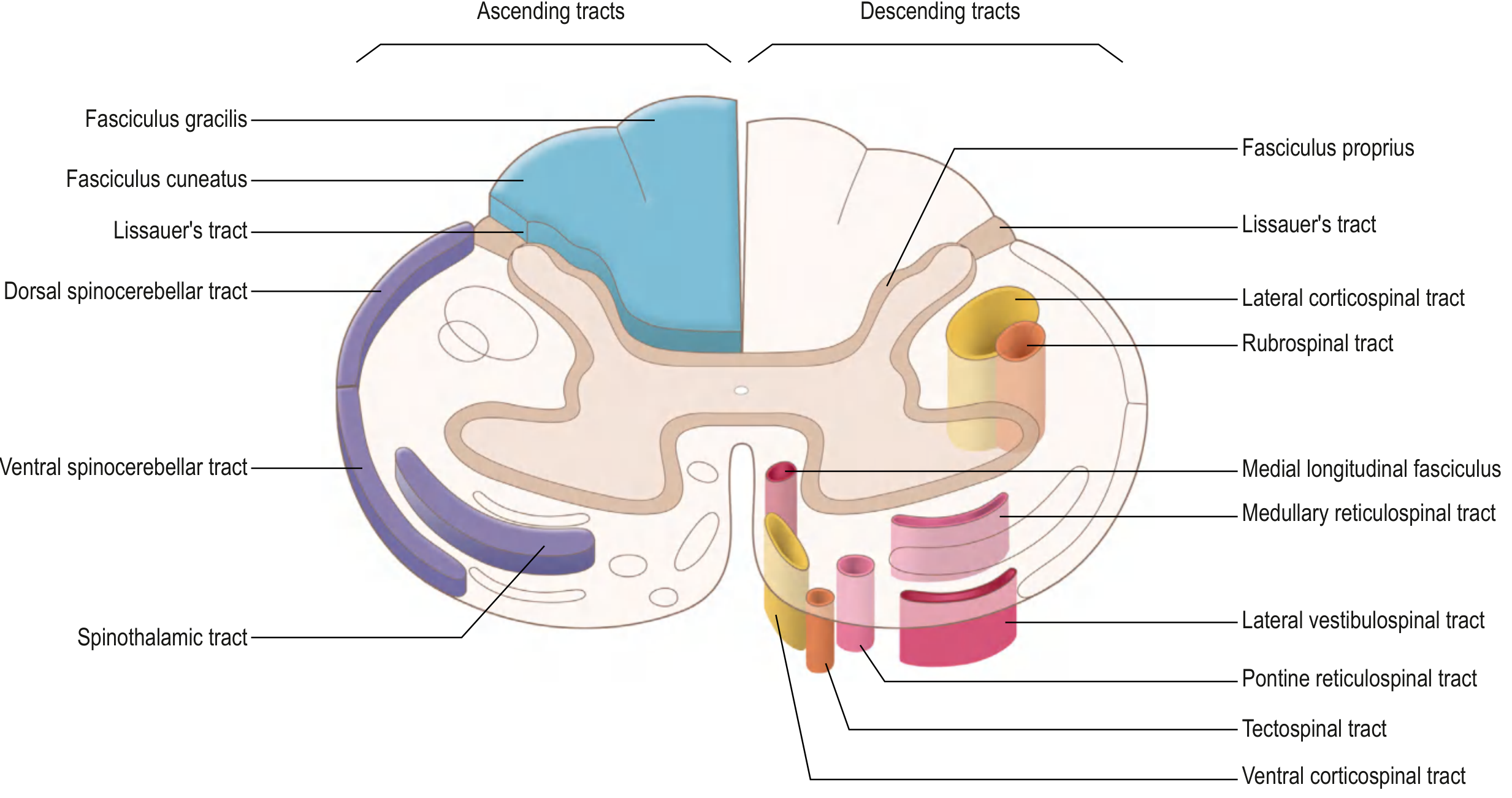
Major Ascending Tracts (carry sensory information to the brain)
| Tract | Location | Carries | Destination |
|---|---|---|---|
| Fasciculus gracilis + cuneatus (posterior columns) | Dorsal column | Fine touch, proprioception, vibration | Thalamus via medial lemniscus |
| Spinothalamic tract | Lateral column | Pain, temperature, crude touch | Thalamus |
| Dorsal spinocerebellar | Lateral column | Proprioception (ipsilateral) | Cerebellum |
| Ventral spinocerebellar | Lateral column | Proprioception (bilateral) | Cerebellum |
Major Descending Tracts (carry motor commands from the brain)
| Tract | Location | Function |
|---|---|---|
| Lateral corticospinal | Lateral column | Voluntary movement of limbs (contralateral) |
| Anterior corticospinal | Ventral column | Axial muscle control (ipsilateral) |
| Rubrospinal | Lateral column | Limb motor control |
| Lateral vestibulospinal | Ventral column | Balance, extensor tone |
| Reticulospinal (pontine + medullary) | Ventral column | Posture, tone, reflexes |
| Tectospinal | Ventral column | Head-eye reflex movements |
The lateral corticospinal tract is clinically the most important - upper motor neuron axons decussate at the caudal medulla (pyramidal decussation), descend in the lateral column, and synapse on lower motor neurons in the anterior horn.
7. Blood Supply
The spinal cord receives arterial supply from two sources:
- Anterior spinal artery (single) - supplies the anterior 2/3 of the cord
- Posterior spinal arteries (paired) - supply the posterior 1/3
These are supplemented by radicular arteries at multiple levels, with the artery of Adamkiewicz (great anterior radicular artery, usually arising from T9-T12) being the dominant supply to the thoracolumbar cord.
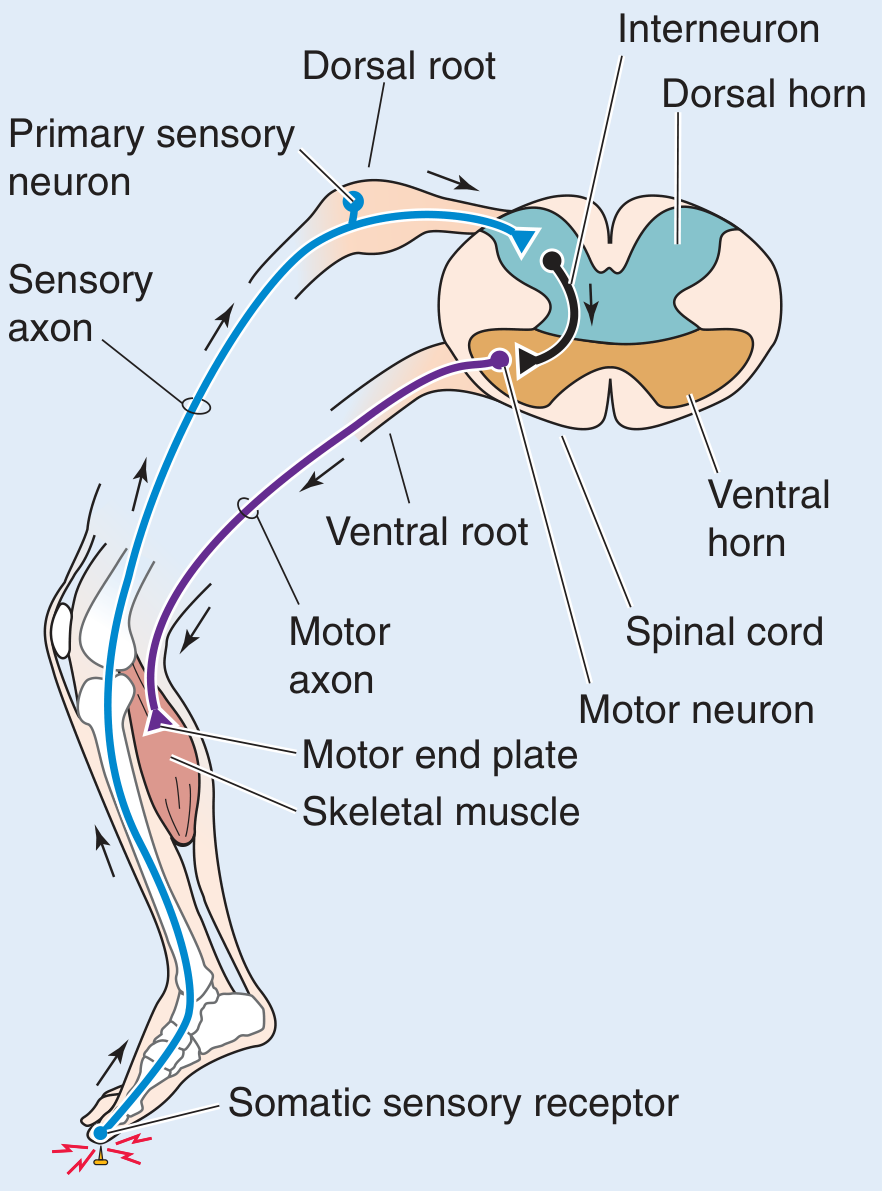
PART 2: THE REFLEX ARC
1. Definition
A reflex is a stereotyped, specific motor response to a particular stimulus. The neuronal circuit that directs this response is the reflex arc.
2. Components of the Reflex Arc
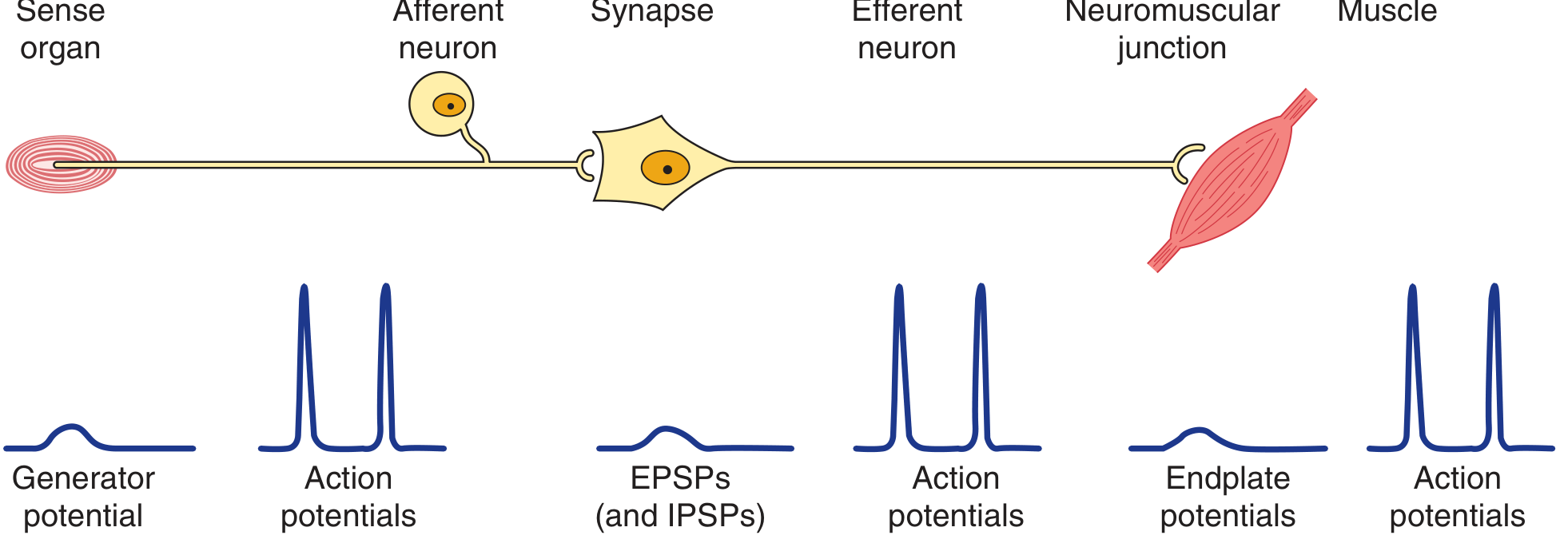
The basic unit consists of 5 components:
- Sensory receptor - detects the stimulus; generates a graded receptor potential proportional to stimulus strength
- Afferent (sensory) neuron - carries the signal to the CNS via dorsal root; cell bodies in the dorsal root ganglion; generates all-or-none action potentials
- Integrating center (CNS interneurons) - in the spinal gray matter; generates graded EPSPs and IPSPs
- Efferent (motor) neuron - lower motor neuron; carries the command from the ventral horn out via the ventral root
- Effector (muscle/gland) - produces the response; generates graded endplate potentials
The alpha motoneurons supplying extrafusal skeletal muscle fibers are the "final common pathway" - all neural influences on muscular contraction converge here.
3. Types of Spinal Cord Reflexes
| Type of Reflex | Example | Synapses | Stimulus | Afferent Fiber | Response |
|---|---|---|---|---|---|
| Stretch (myotatic) reflex | Knee jerk | 1 (monosynaptic) | Stretch (lengthening) of muscle | Group Ia | Contraction of same muscle |
| Golgi tendon reflex | Clasp-knife | 2 (dysynaptic) | Contraction (shortening) of muscle | Group Ib | Relaxation of same muscle |
| Flexor-withdrawal reflex | Touching a hot stove | Many (polysynaptic) | Pain / noxious stimulus | Groups II, III, IV | Ipsilateral flexion + contralateral extension |
4. Stretch Reflex (Monosynaptic)
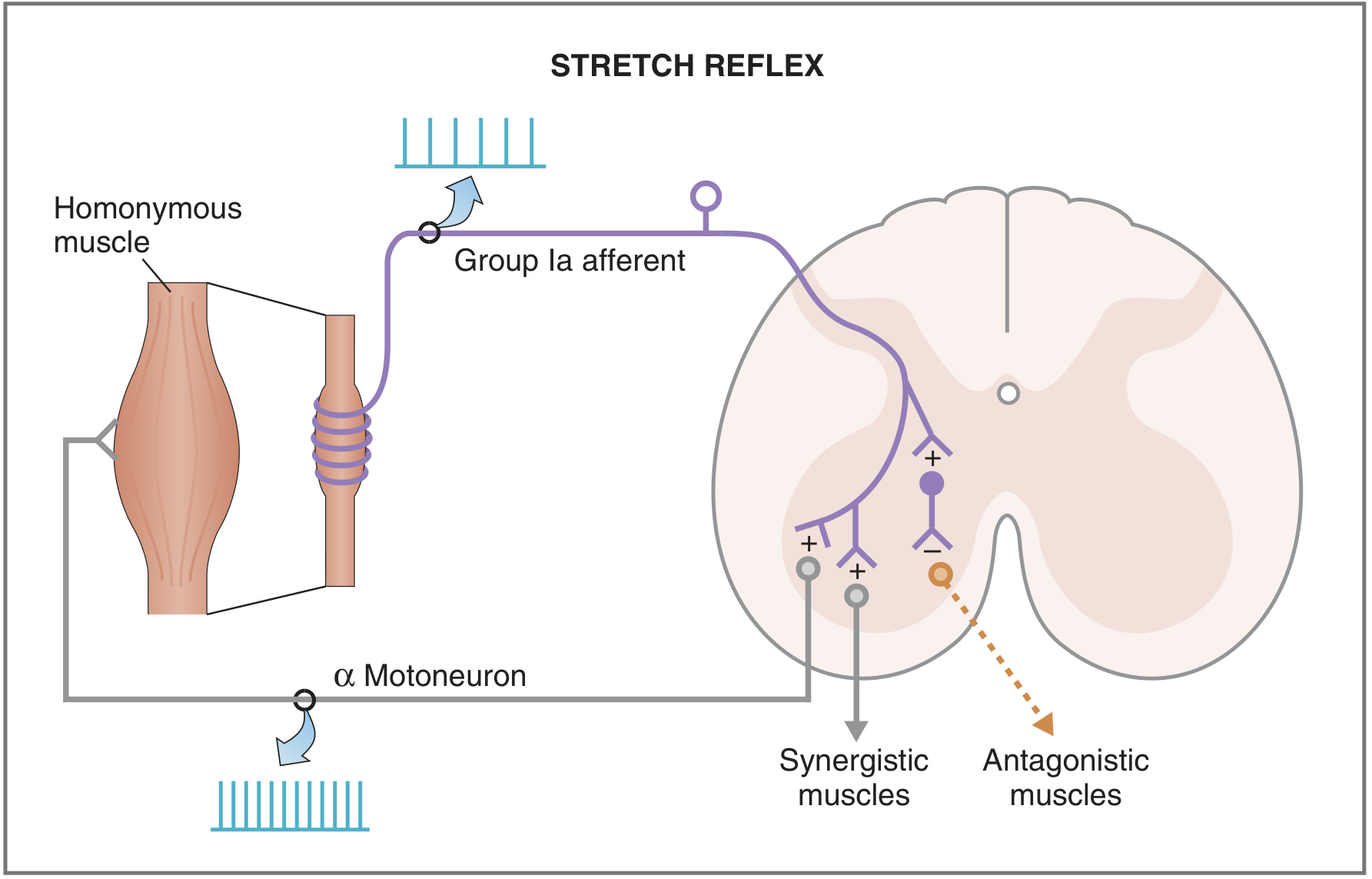
Steps:
- Muscle is stretched → muscle spindles (intrafusal fibers) are stretched
- Group Ia afferent fibers (detecting velocity of stretch) and Group II fibers (detecting length) increase firing rate
- Group Ia afferents enter spinal cord via dorsal root and synapse directly on alpha motoneurons (the single synapse)
- Alpha motoneurons activate extrafusal fibers of the homonymous (same) muscle → muscle contracts, opposing the stretch
- Simultaneously, synergistic muscles contract and antagonistic muscles relax (reciprocal inhibition via Ia inhibitory interneurons)
- Gamma motoneurons are co-activated to maintain spindle sensitivity during contraction
Neurotransmitter at central synapse: Glutamate
Clinical example - Knee jerk (patellar reflex):
- Tap patellar tendon → stretches quadriceps → Group Ia afferents fire → alpha motoneurons fire → quadriceps contracts → leg extends
- Spinal level: L3-L4
- Grading: 0 (absent) to 5+ (sustained clonus)
DTR spinal levels for clinical testing:
| Reflex | Spinal Level |
|---|---|
| Biceps | C5, C6 |
| Triceps | C7 |
| Patellar (knee jerk) | L4 |
| Achilles (ankle jerk) | S1 |
5. Golgi Tendon Reflex (Dysynaptic - Inverse Myotatic)
The Golgi tendon organ is located in tendons, arranged in series with extrafusal fibers (unlike muscle spindles, which are in parallel).
Steps:
- Muscle contracts → extrafusal fibers shorten → Golgi tendon organs activated
- Group Ib afferent fibers activated → synapse on inhibitory interneurons in spinal cord
- Inhibitory interneurons inhibit alpha motoneurons → muscle relaxes
- Synergistic muscles also relax; antagonistic muscles contract
This reflex acts as a protective mechanism against excessive muscle tension.
The clasp-knife reflex is an abnormal exaggeration seen in spasticity: initial resistance to passive stretch suddenly gives way as the Golgi tendon reflex is triggered.
6. Flexor-Withdrawal Reflex (Polysynaptic)
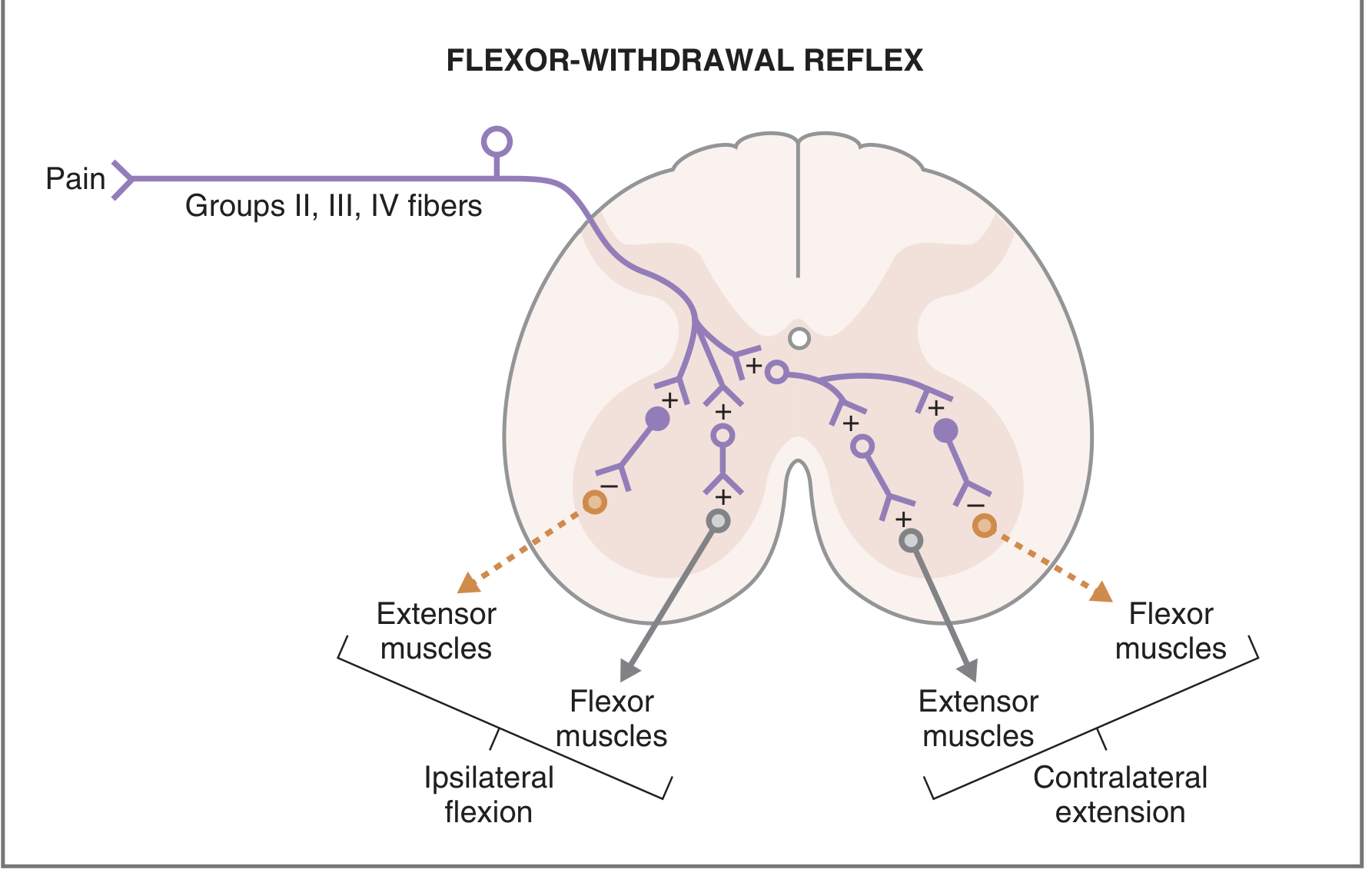
Steps:
- Painful/noxious stimulus activates flexor reflex afferent fibers (Groups II, III, IV) entering via dorsal root
- These synapse on multiple interneurons in the spinal cord (hence polysynaptic)
- Ipsilateral side: Flexors contract, extensors relax → withdrawal of the limb
- Contralateral side: Extensors contract, flexors relax → crossed-extension reflex to maintain balance
- Afterdischarge - persistent neural firing in polysynaptic circuits keeps the contracted muscles contracted even after the stimulus is removed
7. Modulation of Reflexes
Reflex activity is not fixed. It is continuously modulated by:
- Descending pathways from the cerebral cortex and brainstem
- Convergence of multiple inputs onto alpha motoneurons - on average ~10,000 synaptic knobs converge on a single motor neuron
- Higher center damage (e.g., upper motor neuron lesion) hyperactivates stretch reflexes (hyperreflexia, clonus) because inhibitory descending input is lost
- Lower motor neuron or peripheral nerve damage abolishes the reflex (areflexia)
Summary Table: UMN vs LMN Lesion Effects on Reflexes
| Feature | Upper Motor Neuron (UMN) Lesion | Lower Motor Neuron (LMN) Lesion |
|---|---|---|
| Deep tendon reflexes | Hyperreflexia | Hyporeflexia / absent |
| Tone | Spasticity | Flaccidity |
| Babinski sign | Present | Absent |
| Muscle atrophy | Disuse (mild) | Denervation (severe) |
| Fasciculations | Absent | Present |
Sources: Gray's Anatomy for Students, p. 119-120 | Costanzo Physiology 7th Ed., pp. 76, 111-113 | Ganong's Review of Medical Physiology 26th Ed., pp. 235-236 | Neuroanatomy through Clinical Cases 3rd Ed., pp. 62-63, 250 | Medical Physiology (Boron & Boulpaep), p. 419
This is a shared conversation. Sign in to Orris to start your own chat.