Pulmonary embolism lastest guidelines
Reading File
Checking Date & Time
Finding Sources
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND "guideline"[pt]
Searching the Web
pulmonary embolism guidelines 2024 2025 ESC AHA latest recommendations
Reading Article
PMID: 41712677
Reading Article
PMID: 40587333
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer.
Pulmonary Embolism: Latest Guidelines (2026)
Most current guidance: The 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults was published in Circulation (March 2026) and JACC (April 2026). This is a de novo guideline — the most comprehensive and current available. PMID 41712677 | PMID 41712898
A key feature of this 2026 guideline is the introduction of the AHA/ACC Acute Pulmonary Embolism Clinical Categories, replacing the older "massive/submassive" terminology to enhance severity classification and treatment decisions.
1. Risk Stratification
PE severity is determined by hemodynamic status and right ventricular (RV) dysfunction — not clot size.
| Category | Criteria | Mortality |
|---|---|---|
| Low-Risk | Hemodynamically stable; no RV dysfunction | <1–3% |
| Intermediate-Risk | Hemodynamically stable + RV dysfunction on echo or positive troponin | 3–15% |
| High-Risk ("massive") | SBP <90 mmHg sustained ≥15 min (not from arrhythmia); or SBP drop >40 mmHg; or vasopressor-dependent; or bradycardia <40 bpm | 15–50% |
Intermediate-risk is further subdivided:
- Intermediate-low: PESI class ≥III or sPESI ≥1, plus RV dysfunction OR elevated troponin (not both)
- Intermediate-high: both RV dysfunction on imaging AND elevated troponin
— Rosen's Emergency Medicine, p. 1208
2. Diagnosis
Pre-test Probability (PTP)
Wells Score (most widely used):
- Score ≤4 = low/moderate PTP → D-dimer testing
- Score >4 = high PTP → proceed directly to CT pulmonary angiography (CTPA)
Revised Geneva Score: Uses only objective elements; score 0–3 = low, 4–10 = intermediate, >10 = high probability. Performs similarly to Wells in clinical practice.
PERC Rule
When clinician gestalt for PE is low, if ALL 8 criteria are met, testing is not required:
- Age <50
- Pulse <100
- SaO₂ >94%
- No unilateral leg swelling
- No hemoptysis
- No recent trauma or surgery
- No prior PE/DVT
- No hormone use
D-Dimer
- 95–98% sensitive, 40–55% specific
- Excludes PE in non-high PTP when negative (NPV 99–100%)
- Age-adjusted threshold: D-dimer < (age × 10 µg/L) in patients >50 years — shown to safely increase specificity and reduce unnecessary imaging without increasing missed PE rates
- YEARS algorithm: Can use higher D-dimer threshold (1000 ng/mL) when no YEARS criteria present
Imaging
- CTPA: Gold standard — first-line imaging for suspected PE
- V/Q scan: Alternative when CTPA contraindicated (renal failure, contrast allergy, pregnancy)
- Echocardiography: Confirms RV dysfunction; useful in high-risk unstable patients when CTPA is not immediately available
- Lower extremity US: Can support diagnosis by showing DVT
— Rosen's Emergency Medicine, pp. 1205–1207
3. Treatment by Risk Category
Low-Risk PE
- Initiate anticoagulation — DOACs preferred (apixaban or rivaroxaban as first-line; dabigatran and edoxaban are alternatives after initial parenteral therapy)
- Early discharge / outpatient management — validated using either:
- PESI / sPESI score, or
- Hestia criteria (negative = safe for home)
- Avoid systemic thrombolysis
Intermediate-Risk PE (Submassive)
- Anticoagulate immediately (DOAC or LMWH → VKA)
- Close monitoring in monitored setting; ICU or step-down unit for intermediate-high
- Systemic thrombolysis not routine — reserve for clinical deterioration
- Catheter-directed therapy (CDT): Reasonable option for intermediate-high risk patients at centres with expertise; 2025 ESVM guidelines confirm CDT (catheter-directed thrombolysis or mechanical thrombectomy) is gaining ground here [PMID 40587333]
- PERT (PE Response Team): Multi-disciplinary team approach recommended for intermediate-high and high-risk PE
High-Risk PE (Massive)
- Systemic thrombolysis is the treatment of choice in the absence of contraindications
- Alteplase 100 mg IV over 2 hours (standard dose)
- 0.6 mg/kg (max 50 mg) over 15 min if cardiac arrest imminent
- Absolute contraindications to thrombolysis: Prior intracranial hemorrhage, known structural intracranial lesion, ischemic stroke within 3 months, active bleeding
- If thrombolysis contraindicated or fails: surgical embolectomy or catheter-based mechanical thrombectomy
- Anticoagulation: Unfractionated heparin (UFH) weight-based bolus + infusion preferred acutely (easily reversible)
- Vasopressor support (norepinephrine preferred for hemodynamic instability)
- Avoid aggressive fluid resuscitation (can worsen RV dilation)
— Rosen's Emergency Medicine, pp. 1208–1210
4. Anticoagulation Summary
| Agent | Regimen | Notes |
|---|---|---|
| Apixaban | 10 mg BID × 7 days → 5 mg BID | No parenteral bridging needed; preferred DOAC |
| Rivaroxaban | 15 mg BID × 21 days → 20 mg OD | No parenteral bridging needed |
| Dabigatran | After 5–10 days LMWH → 150 mg BID | Requires parenteral lead-in |
| Edoxaban | After 5–10 days LMWH → 60 mg OD | Requires parenteral lead-in |
| LMWH → Warfarin | INR 2–3 | Still appropriate in pregnancy, cancer |
| UFH | Weight-based IV infusion | Preferred in high-risk/unstable PE |
Cancer-associated PE: LMWH (e.g., dalteparin) remains preferred, though DOACs (apixaban, rivaroxaban) are now acceptable alternatives per recent evidence.
Pregnancy: LMWH throughout pregnancy and for ≥6 weeks postpartum. DOACs and warfarin are contraindicated.
5. Duration of Anticoagulation
| Trigger | Duration |
|---|---|
| Provoked by major transient risk factor (surgery, trauma, immobility) | 3 months |
| Provoked by minor transient risk factor (oestrogen use, travel) | 3–6 months |
| First unprovoked PE | At least 3 months; consider extended if low bleeding risk |
| Second unprovoked VTE | Indefinite anticoagulation recommended |
| Active cancer | Indefinite (until cancer resolved) |
6. Special Populations
- Pregnancy: V/Q scan preferred over CTPA (less maternal breast radiation); LMWH is the anticoagulant of choice; peripartum management requires haematology/obstetrics co-management
- Renal impairment: UFH or VKA preferred when CrCl <15–30 mL/min; DOAC dose adjustments required
- Elderly: Age-adjusted D-dimer threshold; higher bleeding risk with anticoagulation must be weighed
7. Chronic Thromboembolic Pulmonary Hypertension (CTEPH)
- Screen all symptomatic PE patients at follow-up (3–6 months) with echocardiography
- Confirmed by right heart catheterization + V/Q scan
- Treatment:
- Pulmonary endarterectomy (PEA): Curative in operable patients — gold standard
- Balloon pulmonary angioplasty (BPA): For inoperable/persistent CTEPH; growing evidence base (2026 BPA-CTEPH Alliance statement [PMID 42055655])
- Riociguat (soluble guanylate cyclase stimulator): Approved pharmacotherapy for CTEPH
Key 2026 Guideline Highlights vs. Prior Guidance
| Update | Prior | 2026 AHA/ACC |
|---|---|---|
| Risk classification terminology | "Massive / Submassive / Low-risk" | New AHA/ACC Acute PE Clinical Categories (more precise) |
| CTPA for diagnosis | Standard | Still first-line; clearer role for echo in unstable patients |
| CDT for intermediate-high | Emerging option | More formally supported, PERT teams recommended |
| DOAC use in cancer | LMWH preferred | DOACs as acceptable alternative in selected patients |
| Outpatient treatment | Selected low-risk | Broader criteria, PESI/Hestia validated |
Key References:
- 2026 AHA/ACC PE Guideline — Circulation (PMID 41712677) — the definitive current guideline
- 2025 ESVM Interventional VTE Guidelines (PMID 40587333) — catheter-based therapies
- 2026 BPA-CTEPH Alliance Statement (PMID 42055655) — balloon pulmonary angioplasty
- Rosen's Emergency Medicine, 9th ed. — Chapter 74
Risk stratification
Checking Date & Time
Finding Sources
Finding Sources
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND "risk stratification"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive breakdown of PE risk stratification, integrating the 2026 AHA/ACC guideline framework with detailed scoring tools.
PE Risk Stratification
Risk stratification in acute PE has two goals: (1) identify patients who need immediate aggressive intervention, and (2) identify those safe for early discharge. The 2026 AHA/ACC guideline formalises this into distinct clinical categories based on hemodynamic status, RV function, and biomarkers — not clot size or location.
Step 1 — Hemodynamic Screen (First Branch Point)
The primary question: Is the patient in shock or persistent hypotension?
High-Risk PE is defined by ANY of:
- SBP <90 mmHg sustained for ≥15 minutes (not due to arrhythmia or hypovolemia)
- SBP drop >40 mmHg from baseline
- Vasopressor requirement
- Cardiac arrest (pulseless electrical activity is the most common rhythm in PE arrest)
- Severe bradycardia <40 bpm with shock features
If YES → High-Risk PE → emergency reperfusion (systemic thrombolysis or embolectomy) without delay If NO → proceed to Step 2
Step 2 — Clinical Severity Score (PESI / sPESI)
For hemodynamically stable patients, calculate PESI or sPESI to separate intermediate from low risk.
Full PESI Score
| Variable | Points |
|---|---|
| Age | Age in years |
| Male sex | +10 |
| History of cancer | +30 |
| History of heart failure | +10 |
| History of chronic lung disease | +10 |
| Heart rate ≥110 bpm | +20 |
| SBP <100 mmHg | +30 |
| Respiratory rate ≥30/min | +20 |
| Temperature <36°C | +20 |
| Altered mental status | +60 |
| SpO₂ <90% | +20 |
PESI Classes:
| Class | Score | 30-day Mortality |
|---|---|---|
| I (Very Low) | ≤65 | 0–1.6% |
| II (Low) | 66–85 | 2.0–3.5% |
| III (Moderate) | 86–105 | 6.5–7.7% |
| IV (High) | 106–125 | 10.4–12.2% |
| V (Very High) | ≥126 | 17.9–24.5% |
Classes I–II = Low risk; Classes III–V = Elevated risk
Simplified PESI (sPESI)
| Variable | Points |
|---|---|
| Age >80 years | +1 |
| History of cancer | +1 |
| Heart failure or chronic lung disease | +1 |
| Heart rate ≥110 bpm | +1 |
| SBP <100 mmHg | +1 |
| SpO₂ <90% | +1 |
- sPESI = 0 → Low risk (30-day mortality ~1%)
- sPESI ≥1 → Elevated/Intermediate risk
sPESI ≥1 or PESI Class ≥III = Intermediate-risk → proceed to Step 3 for sub-classification
— Braunwald's Heart Disease, p. 978; Murray & Nadel's Respiratory Medicine, p. 1880
Step 3 — Intermediate-Risk Sub-Classification
For normotensive patients with sPESI ≥1 or PESI ≥III, assess RV dysfunction (imaging) and myocardial injury (biomarkers):
| Sub-category | RV Dysfunction | Biomarker Elevation | 30-day Mortality |
|---|---|---|---|
| Intermediate-High | ✅ Present | ✅ Elevated | ~5–15% |
| Intermediate-Low | ✅ Present OR ✅ Elevated | (only one, not both) | ~3–5% |
RV dysfunction on imaging (any one):
- Echo: RV dilation, hypokinesis, or interventricular septal bowing toward LV
- CT (CTPA): RV:LV ratio ≥0.9–1.0 (88% sensitive but only 39% specific; confirm with echo)
Biomarkers:
- Troponin (I or T): Elevation reflects RV myocyte injury/ischemia; high negative predictive value for adverse outcomes when normal. High-sensitivity assays improve prognostic accuracy.
- BNP / NT-proBNP: Reflects RV pressure overload and wall stretch. BNP <50 pg/mL has 97% NPV for adverse outcomes.
Troponin T Survival Data (30 days):
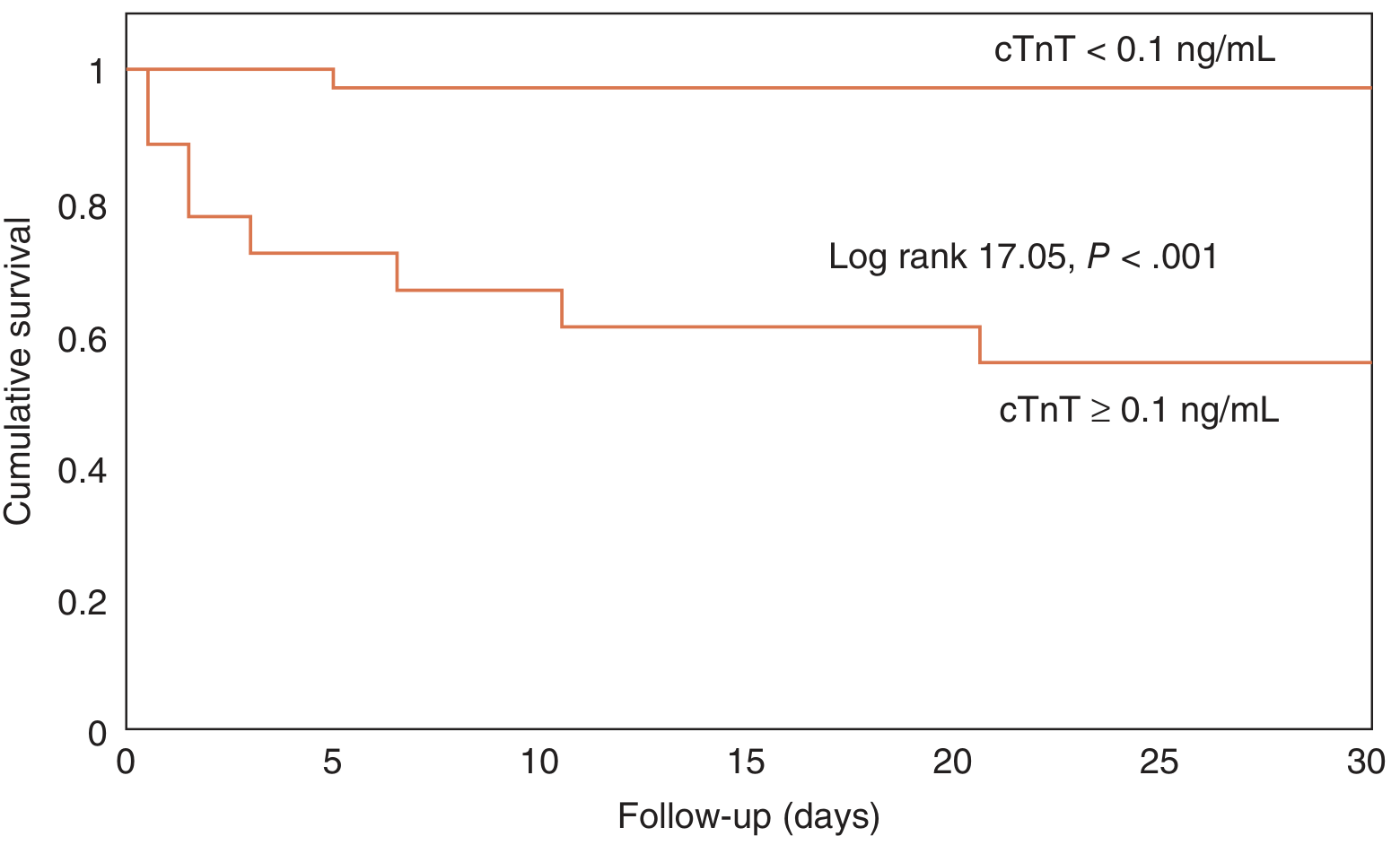
30-day survival is markedly worse in PE patients with cTnT ≥0.1 ng/mL (log-rank P<0.001). — Fuster & Hurst's The Heart, 15th ed., p. 1778
Important: Despite its utility, neither troponin nor echo alone should drive reperfusion decisions. Both the positive predictive value for death is low — most biomarker-elevated patients survive with anticoagulation alone. The risk of aggressive therapy must be weighed against the potential benefit.
— Murray & Nadel's Respiratory Medicine, p. 1848; Fuster & Hurst's The Heart, pp. 1777–1778
Step 4 — Low-Risk Identification & Outpatient Eligibility
Patients with:
- sPESI = 0 (or PESI Class I–II), AND
- No RV dysfunction on echo/CT, AND
- Normal troponin
→ Low-Risk PE (<1–3% mortality)
Outpatient Treatment — Hestia Criteria
If ALL Hestia criteria are absent, the patient is safe for home management:
| Hestia Criterion | Exclusion if Present |
|---|---|
| Hemodynamic instability | ✅ |
| Thrombolysis or embolectomy needed | ✅ |
| Active bleeding or high risk | ✅ |
| Requires >24h IV heparin | ✅ |
| SpO₂ <90% on room air | ✅ |
| PE diagnosed on anticoagulation | ✅ |
| Severe pain requiring IV analgesia >24h | ✅ |
| Medical/social reason for admission | ✅ |
| Creatinine clearance <30 mL/min | ✅ |
| Severe liver impairment | ✅ |
| Pregnancy | ✅ |
| Documented HIT | ✅ |
Summary: Full Risk Matrix
CONFIRMED ACUTE PE
│
├─► Shock / Hypotension? ──YES──► HIGH-RISK (≥15–50% mortality)
│ → Systemic thrombolysis / embolectomy
│
└─► Stable → PESI / sPESI
│
├─► PESI I-II / sPESI 0 → LOW-RISK (<1–3%)
│ → DOAC; consider outpatient
│
└─► PESI ≥III / sPESI ≥1 → INTERMEDIATE RISK
│
├─► RV dysfunction AND ↑troponin
│ → INTERMEDIATE-HIGH (5–15%)
│ → ICU; PERT; consider CDT
│
└─► RV dysfunction OR ↑troponin (not both)
→ INTERMEDIATE-LOW (~3–5%)
→ Monitored bed; anticoagulate
Additional Scoring: Bova Score
For intermediate-risk PE, the Bova score uses 4 variables to predict PE-related complications at 30 days:
| Variable | Points |
|---|---|
| Elevated cardiac troponin | +2 |
| Heart rate ≥110 bpm | +1 |
| RV dysfunction on echo or CT | +2 |
| SBP 90–100 mmHg | +2 |
- Stage I (0–2): 1.7% PE-related mortality
- Stage II (3–4): 5.0%
- Stage III (≥5): 15.5%
Useful for further risk-grading within the intermediate-risk group to guide intensity of monitoring and escalation threshold.
ECG Findings Correlating with Higher Risk
ECG patterns associated with increased risk of circulatory collapse and death:
- S1Q3T3 pattern (classic RV strain)
- Right bundle branch block (complete > incomplete, progressive RBBB is ominous)
- Inverted T waves in V1–V4, inferior leads, or right-sided leads
- ST elevation in aVR
- Prolonged QT interval
- Sinus tachycardia or new atrial fibrillation
- Widespread T-wave inversions
— Murray & Nadel's Respiratory Medicine, p. 1848
Sources: Braunwald's Heart Disease, p. 978 | Murray & Nadel's Respiratory Medicine, pp. 1848, 1865–1880 | Fuster & Hurst's The Heart 15th ed., pp. 1777–1778 | Rosen's Emergency Medicine, pp. 1208–1210 | 2026 AHA/ACC PE Guideline (PMID 41712677)
This is a shared conversation. Sign in to Orris to start your own chat.