Purulent Anthritis of Knee joint
Reading File
search_medical_text
purulent septic arthritis knee joint etiology diagnosis management
search_medical_image
purulent septic arthritis knee joint
GradeResponse
GradeResponse
Purulent Arthritis of the Knee Joint (Septic Arthritis)
Purulent (septic) arthritis of the knee is an acute, destructive joint infection characterized by the presence of purulent (pus-containing) fluid within the joint space. The knee is the most commonly affected joint, accounting for ~50% of all cases.
Etiology & Pathogenesis
| Route | Description |
|---|---|
| Hematogenous (most common) | Bacteremia seeds the highly vascular synovium |
| Direct inoculation | Trauma, surgery, intra-articular injection |
| Contiguous spread | Adjacent osteomyelitis or soft tissue infection |
Common Causative Organisms
| Population | Organisms |
|---|---|
| Adults (non-STI) | Staphylococcus aureus (most common overall), Streptococcus spp., Gram-negatives |
| Sexually active adults | Neisseria gonorrhoeae (most common in young adults) |
| Elderly / immunocompromised | S. aureus, Gram-negatives (E. coli, Pseudomonas) |
| Children (< 5 yrs) | Kingella kingae, S. aureus, Group B Strep |
| IV drug users | Pseudomonas aeruginosa, S. aureus |
| Prosthetic joint | S. epidermidis, S. aureus, Cutibacterium acnes |
Clinical Presentation
- Acute monoarthritis — pain, swelling, warmth, erythema of the knee
- Restricted range of motion — patient holds knee in slight flexion (position of comfort)
- Fever, rigors, systemic toxicity
- Massive joint effusion — circumferential knee swelling (see image below)
- In gonococcal arthritis: may have preceding migratory polyarthralgia, skin pustules, tenosynovitis (the triad)
Diagnostic Imaging & Clinical Findings
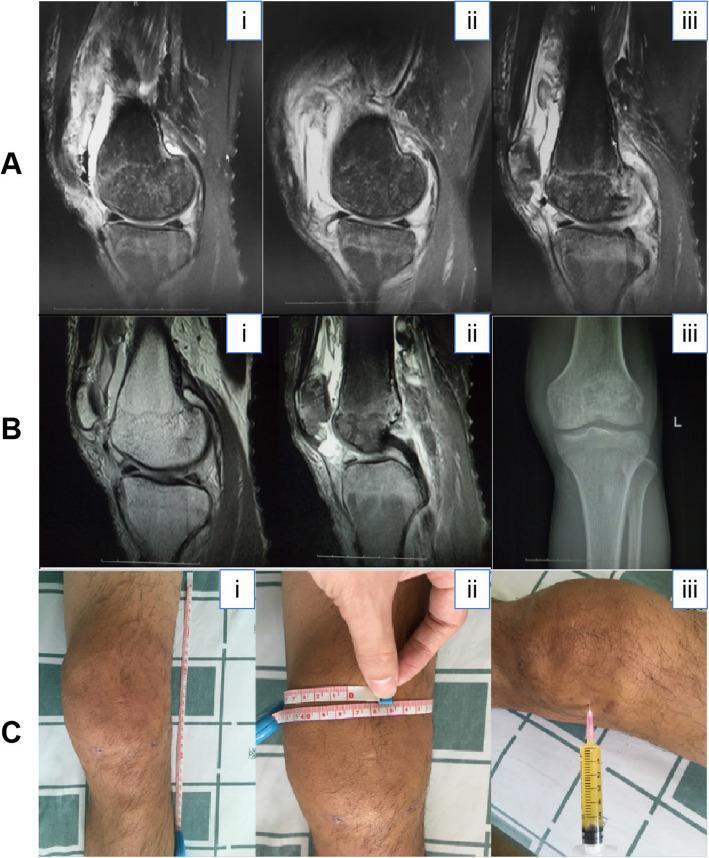
This composite figure illustrates diagnostic findings in a confirmed case of purulent knee arthritis. Row A (sagittal MRI): significant joint effusion, bone marrow edema in distal femur and proximal tibia, posterior horn meniscal tears. Row B (post-operative MRI + AP radiograph): reduced joint swelling, improved marrow signal, soft tissue swelling, and periarticular osteopenia. Row C (clinical photographs): severe knee swelling with 29 cm longitudinal and 47.4 cm circumferential measurements, and bedside arthrocentesis yielding ~6 mL of yellow, purulent synovial fluid.
Investigations
Laboratory
| Test | Finding in Septic Arthritis |
|---|---|
| WBC | Elevated (non-specific) |
| ESR / CRP | Elevated (non-specific) |
| Blood cultures | Positive in ~50% — collect during febrile episodes |
| Procalcitonin | May support bacterial infection |
Synovial Fluid Analysis (Arthrocentesis — KEY diagnostic step)
| Parameter | Normal | Septic Arthritis |
|---|---|---|
| Appearance | Clear, straw-colored | Turbid, yellow-green, purulent |
| Viscosity | High | Low |
| WBC (cells/mm³) | < 200 | > 50,000 (often > 100,000); predominantly PMNs > 75% |
| Glucose | Equal to serum | Reduced |
| Protein | Low | Elevated |
| Gram stain | Negative | Positive in 50–70% |
| Culture | Negative | Positive in 70–90% (send in blood culture bottles) |
Per the Guide to Utilization of the Microbiology Laboratory (p. 82): "Traditionally, a synovial fluid leukocyte count more than 50,000 cells/mm³ was considered to suggest septic arthritis; however, lower counts do not exclude the diagnosis." If Gram stain and culture are negative, multiplex PCR or 16S rRNA gene PCR/sequencing should be considered. K. kingae and N. gonorrhoeae are included in recently FDA-cleared multiplex PCR panels for synovial fluid.
Imaging
| Modality | Findings |
|---|---|
| X-ray | Early: soft tissue swelling, joint space widening; Late: osteopenia, joint space narrowing, bony destruction |
| Ultrasound | Joint effusion (guides aspiration), synovial thickening |
| MRI (most sensitive) | Effusion, synovial enhancement, bone marrow edema, cartilage destruction, adjacent soft tissue involvement |
Differential Diagnosis
- Crystal arthropathies (gout, pseudogout) — synovial fluid microscopy distinguishes
- Reactive arthritis (Reiter's syndrome)
- Rheumatoid arthritis flare
- Hemarthrosis (trauma, coagulopathy)
- Transient synovitis (children)
- Lyme arthritis (Borrelia burgdorferi)
- Osteoarthritis exacerbation
Management
1. Drainage (Surgical or Needle)
Prompt and complete drainage is mandatory to prevent cartilage destruction.
| Method | Indication |
|---|---|
| Serial needle arthrocentesis | Early, accessible effusions; initial management |
| Arthroscopic lavage & debridement | Preferred when feasible; allows direct visualization |
| Open surgical drainage | Failed arthroscopy, loculated collections, adjacent osteomyelitis, prosthetic joint infection |
2. Empiric Antibiotic Therapy
Started immediately after cultures are obtained (do not wait for results).
| Clinical Scenario | Empiric Regimen |
|---|---|
| Healthy adult (non-STI) | Flucloxacillin or Nafcillin (anti-staphylococcal) IV |
| MRSA risk or penicillin allergy | Vancomycin IV |
| Gram-negative concern (elderly, immunocompromised, IVDU) | Add 3rd-gen cephalosporin or Piperacillin-tazobactam |
| Gonococcal arthritis | Ceftriaxone 1g IV/IM daily |
| Children | Flucloxacillin ± cefotaxime (cover K. kingae) |
3. Duration of Therapy
- Native joint: typically 2–4 weeks IV, followed by oral step-down (total 4–6 weeks)
- Gonococcal: 7–14 days (1 week IV then oral)
- Guided by clinical response, inflammatory markers, and organism sensitivities
4. Supportive Care
- Joint immobilization initially, then early mobilization and physiotherapy once infection controlled
- Analgesia (NSAIDs used cautiously — may mask fever)
- Treat underlying source (e.g., skin infection, endocarditis screening if bacteremia)
Complications
| Complication | Details |
|---|---|
| Cartilage destruction | From proteolytic enzymes; begins within hours–days |
| Osteomyelitis | Contiguous spread to bone |
| Avascular necrosis | Especially femoral head if hip involved |
| Joint fibrosis / ankylosis | Chronic stiffness, loss of function |
| Chronic osteomyelitis | In inadequately treated cases |
| Septicemia / sepsis | Life-threatening systemic spread |
| Growth disturbance | In children (epiphyseal involvement) |
Prognosis
- Excellent if treated within 24–48 hours of onset
- Delayed treatment (> 5–7 days) leads to significant cartilage and bone destruction
- Poor prognostic factors: extremes of age, S. aureus infection, pre-existing joint disease (RA), immunosuppression, prosthetic joint, delayed diagnosis
Key Clinical Pearl: The combination of acute monoarthritis + fever + purulent joint fluid must be treated as septic arthritis until proven otherwise. Do not delay arthrocentesis and empiric antibiotics waiting for imaging or confirmatory cultures.
This is a shared conversation. Sign in to Orris to start your own chat.