Explain ecg in easy to remember way and how to become expert in reading ecg
Reading File
Finding Sources
Searching the Web
how to read ECG systematically easy mnemonic approach for beginners
Finding Sources
Searching Images
ECG waveform PQRST diagram labeled
Reading File
Finding Sources
Loading Image
Finding Sources
Searching Images
12 lead ECG placement electrode leads diagram
Finding Sources
Searching Images
normal sinus rhythm ECG interpretation steps
Reading File
Reading File
Reading File
I now have comprehensive information from the textbooks. Let me compile the complete, easy-to-remember ECG guide.
ECG: The Complete Easy-to-Remember Guide
What is an ECG?
An ECG (electrocardiogram) records the electrical activity of your heart as tiny voltage differences detected by electrodes on the body surface. Because different parts of the heart depolarize and repolarize in a specific sequence — atria first, then ventricles — these differences create a characteristic waveform you can read.
Part 1: The Waveform — "Please Q RS Tonight"
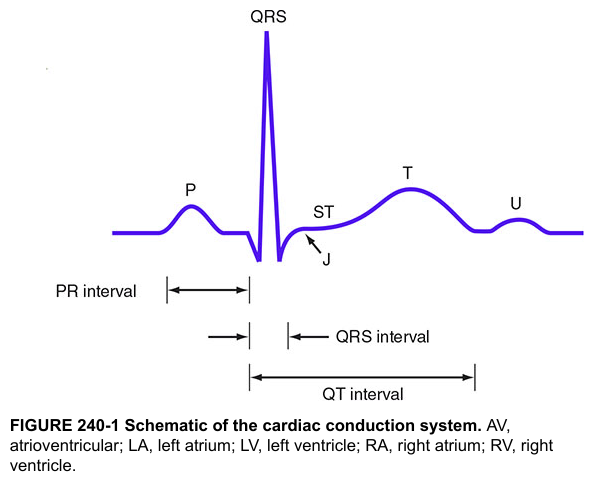
Every heartbeat on an ECG produces the same sequence of waves. Remember them with the mnemonic "Please Q-R-S Tonight U-know":
| Wave/Segment | What it represents | Normal duration/value |
|---|---|---|
| P wave | Atrial depolarization (atria contract) | < 0.12 sec (3 small boxes) |
| PR interval | Conduction from atria → AV node → ventricles | 0.09–0.20 sec (90–200 ms) |
| QRS complex | Ventricular depolarization (ventricles contract) | 0.075–0.11 sec (< 3 small boxes) |
| ST segment | Early ventricular repolarization (flat = normal) | At isoelectric line |
| T wave | Ventricular repolarization | Upright in most leads |
| U wave | After-potential of Purkinje fibers | Small, sometimes invisible |
| QT interval | Full ventricular depolarization + repolarization | Males ≤0.45 sec, Females ≤0.46 sec |
Memory trick for waves: Think of the heart as saying "P-QRS-T" — P is the polite knock (atria), QRS is the big slam (ventricles firing), T is the recovery.
Part 2: The 12 Leads — "Looking at the heart from 12 windows"
The 12 leads are 12 different "camera angles" of the heart's electricity:
Limb Leads (look at the heart in the frontal plane)
- I, II, III — Einthoven's triangle (RA, LA, LL)
- aVR, aVL, aVF — Augmented views (R = right arm, L = left arm, F = foot)
Normal: P waves and QRS upright in I, II, III, aVF. Inverted in aVR (always — because it looks "away" from the heart).
Precordial Leads (look at the heart front-to-back)
- V1–V2 → Right side of heart (septum)
- V3–V4 → Anterior wall (LAD territory)
- V5–V6 → Lateral wall (LCx territory)
Normal progression: Small r, deep S in V1 → tall R, small s in V6 (R wave "grows" across the chest — called R-wave progression)
Which territory → which leads:
| Territory | Leads | Artery |
|---|---|---|
| Inferior | II, III, aVF | RCA |
| Anterior | V1–V4 | LAD |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | V7–V9 / reciprocal in V1–V2 | RCA/LCx |
Part 3: Systematic Reading — "RRIPPER"
Never just glance at an ECG. Use this 7-step system every single time:
| Step | Letter | What to check |
|---|---|---|
| 1 | Rate | Count boxes. 300 ÷ large boxes between R–R = rate. Or: 6-second strip × 10 |
| 2 | Rhythm | Regular or irregular? Is every P followed by QRS? |
| 3 | Intervals | PR (0.09–0.2s), QRS (<0.12s), QT (corrected) |
| 4 | P wave | Present? Upright in II? One P per QRS? |
| 5 | Progression | R-wave grows V1→V6? Transition zone at V3–V4? |
| 6 | Elevation/Depression | ST segment above or below the line? |
| 7 | Repolarization | T wave morphology — inverted, peaked, biphasic? |
Part 4: Key Normal Values at a Glance
| Parameter | Normal |
|---|---|
| Heart rate | 50–100 bpm |
| PR interval | 90–200 ms (one big box = 200 ms) |
| QRS duration | 75–110 ms |
| QTc (corrected) | ≤450 ms (male), ≤460 ms (female) |
| QRS axis | −30° to +90° |
Rate estimation trick: Count large boxes between two R waves → divide 300 by that number.
- 1 box = 300 bpm | 2 = 150 | 3 = 100 | 4 = 75 | 5 = 60 | 6 = 50
Part 5: Pattern Recognition — The "Big 5" to spot first
Once you know normals, these five abnormalities cover the vast majority of clinical ECGs:
1. STEMI (ST Elevation MI)
- ST elevation ≥ 1mm in ≥2 contiguous leads
- Look for: ST elevation with reciprocal depression in the opposite territory
- "Tombstone" or convex (dome-shaped) ST elevation = classic MI pattern
2. Atrial Fibrillation
- No P waves (replaced by chaotic f-waves)
- Irregularly irregular RR intervals
- Remember: "No P, totally irregular = A-Fib"
3. Heart Block (AV Blocks)
- 1st degree: PR > 200 ms, every P conducts → "Just prolonged, nothing dropped"
- 2nd degree Mobitz I (Wenckebach): PR gets longer and longer until a QRS drops → "Longer, longer, longer… DROP"
- 2nd degree Mobitz II: Fixed PR, sudden dropped QRS → dangerous, often needs pacemaker
- 3rd degree (complete): P and QRS have no relationship, rate ~20–40 bpm → emergency
4. Bundle Branch Block
- Wide QRS > 120 ms (3 small boxes)
- RBBB: "RSR' pattern in V1 like rabbit ears" + wide S in I and V6
- LBBB: Broad notched R in V5–V6, no septal q waves → remember WiLLiaM MaRRoW (LBBB: W in V1, M in V6; RBBB: M in V1, W in V6)
5. LVH (Left Ventricular Hypertrophy)
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥ 35 mm
- Plus: ST depression and T-wave inversion in lateral leads (strain pattern)
Part 6: How to Become an Expert — The Roadmap
Stage 1 — Foundation (Weeks 1–4)
- Master the normal ECG cold: know every wave, interval, and normal value by heart
- Draw the PQRST complex from memory daily
- Learn the 12-lead anatomy and which leads represent which wall
- Resource: Costanzo Physiology for cardiac electrophysiology; Goldman-Cecil Medicine Ch. 42 for ECG basics
Stage 2 — Pattern Drills (Months 1–3)
- Read at least 5–10 ECGs per day — this is non-negotiable for expertise
- Use free platforms: ECGpedia, Litfl ECG library, 123sonography ECG course
- For each ECG, use RRIPPER systematically before looking at the interpretation
- Start with obvious rhythms (NSR, A-fib, SVT, VT), then progress to blocks, then ischemia
Stage 3 — Clinical Correlation (Months 3–6)
- Never read an ECG in isolation — always correlate with clinical context
- Practice: "What does this patient's story + ECG tell me together?"
- Learn the common mimics (hyperkalemia → wide QRS; hypothermia → Osborn waves; PE → S1Q3T3)
- Focus on: axis deviation, bundle branch blocks, hypertrophy patterns
Stage 4 — Expert Level (6+ months)
- Read Braunwald's Heart Disease ECG chapters for advanced interpretation
- Study Holter monitoring, stress testing ECGs, and device-based ECGs (pacemakers)
- Aim to read 1,000+ ECGs — studies show ~1,000 interpreted ECGs correlates with clinical competence
- Join ECG case discussions; teach others (teaching solidifies expertise faster than anything)
The single most important rule:
Use the same systematic approach every single time. Experts don't skip steps — they just do them faster. Speed comes from repetition, not shortcuts.
Quick Reference Card
WAVEFORM: P → PR → QRS → ST → T → (U)
Atria AV Vent Repol
RATE: 300 ÷ large boxes (between R-R)
INTERVALS: PR 90-200ms | QRS <120ms | QTc <450ms (M) <460ms (F)
LEADS: Inferior=II,III,aVF | Anterior=V1-V4 | Lateral=I,aVL,V5-V6
SYSTEM: R-R-I-P-P-E-R (Rate, Rhythm, Intervals, P wave, Progression,
Elevation, Repolarization)
Sources: Goldman-Cecil Medicine, 26th ed. (Ch. 42); Costanzo Physiology, 7th ed. (Ch. 4); Braunwald's Heart Disease, 12th ed.; Tintinalli's Emergency Medicine, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.