Diagnostic form of Giardiasis
Reading File
Finding Sources
Finding Sources
Searching PubMed
Giardia diagnosis stool antigen PCR
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is the complete answer:
Diagnostic Forms of Giardiasis
Giardia duodenalis (syn. G. lamblia, G. intestinalis) exists in two diagnostic forms found in fecal specimens and other clinical samples:
1. Trophozoite (Active / Vegetative Form)
The trophozoite is the motile, feeding form that lives in the duodenum and jejunum.
Morphology:
- Pear-shaped (pyriform), 9-12 µm long, 5-15 µm wide
- 2 nuclei, each with a large central karyosome - gives the classic "old man face" / "face looking back at you" appearance
- Large ventral sucking disk (concave, used to attach to intestinal villi)
- 4 pairs of flagella (8 total) for motility
- 2 oblong parabasal (median) bodies below the nuclei - pathognomonic feature
- Bilateral symmetry
Found in: Diarrheal (loose/watery) stools, duodenal aspirates, jejunal biopsy specimens
2. Cyst (Infective / Resistant Form)
The cyst is the environmentally resistant, infective form passed in formed stool.
Morphology:
- Oval/ellipsoidal, 8-12 µm long, 7-10 µm wide (slightly smaller than trophozoite)
- 4 nuclei (mature cyst) - nuclei and parabasal bodies are visible
- Thick protective wall
- Internal structures (axonemes, median bodies) visible on staining
- Minimum infective dose: 10-25 cysts
Found in: Formed stool; resistant to chlorine at standard water-treatment concentrations (1-2 ppm)
Life Cycle - Diagnostic Summary
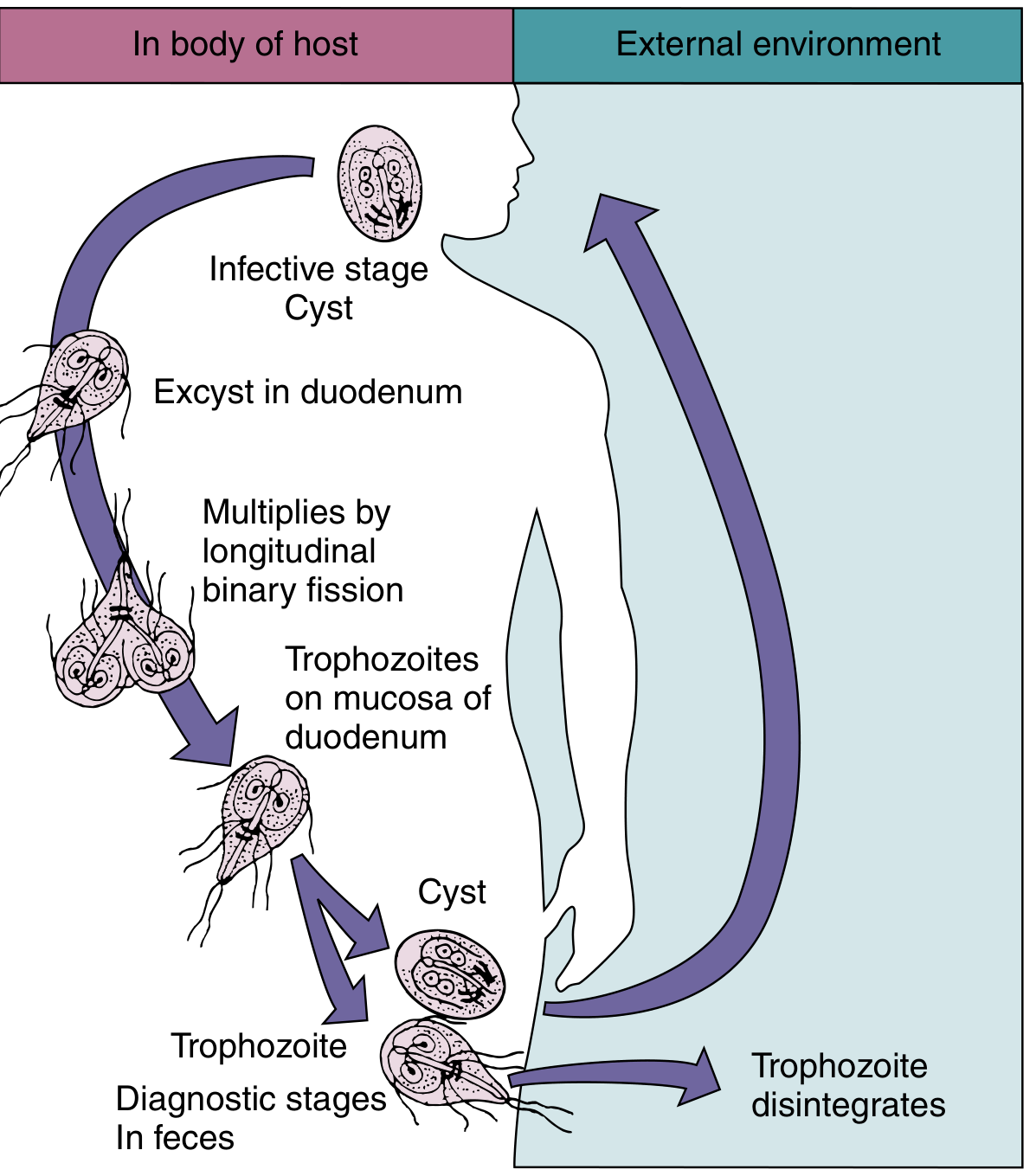
Life cycle of G. duodenalis - note both trophozoite and cyst are diagnostic stages in feces, while the trophozoite disintegrates rapidly in the external environment.
Microscopic Appearance (Stained Preparations)
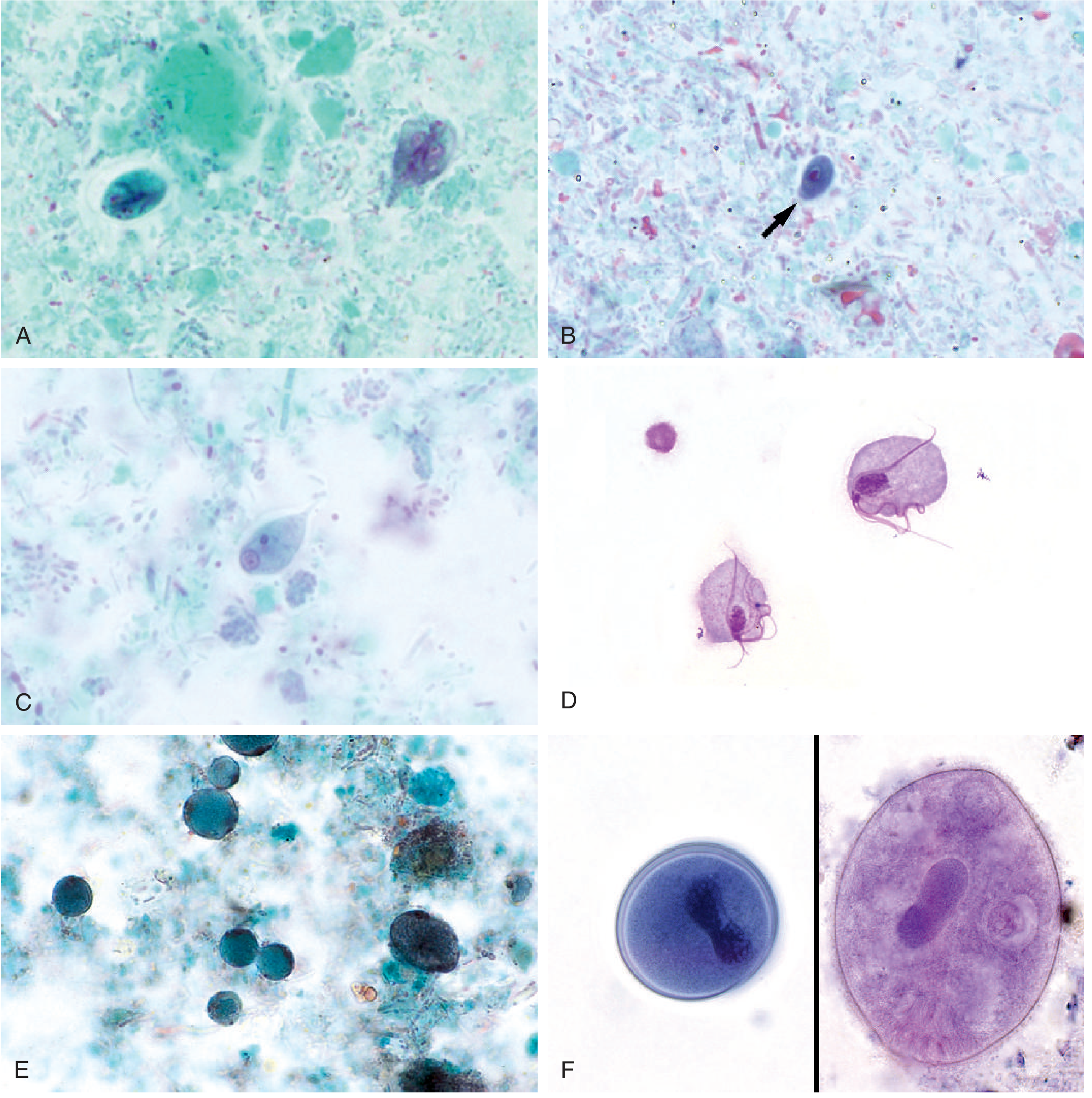
Panel A (top-left): G. duodenalis cyst (left) and trophozoite (right), Wheatley's trichrome stain, 1000x. (Tietz Textbook of Laboratory Medicine, 7th Ed.)
Diagnostic Methods
| Method | Details | Sensitivity |
|---|---|---|
| Stool microscopy (O&P) | Cyst in formed stool; trophozoite in diarrheal stool. Concentration + trichrome/iodine stain. Examine 3 specimens (1/day x 3 days) | 50-70% (single); ~90% (3 specimens) |
| Enzyme Immunoassay (EIA) | Detects Giardia antigen in stool; several commercial kits available | >90% sensitivity; comparable to microscopy |
| Immunofluorescence (IFA) | Detects cysts in stool using fluorescent antibodies | High sensitivity |
| Immunochromatographic assay (LFICA) | Rapid antigen detection; point-of-care format | ~88-98% |
| Multiplex NAAT/PCR | FDA-approved multiplex panels; also genotypes infecting strains (assemblages A/B = human; C-H = animal) | 98-100% sensitivity, ~99% specificity |
| Duodenal aspirate / String test (Enterotest) | Swallowed capsule retrieves duodenal fluid; examined for motile trophozoites | Used when stool repeatedly negative |
| Jejunal biopsy | Rarely needed; shows trophozoites attached to villi; no tissue necrosis | Last resort |
| Culture | Organism can be grown but not adaptable to routine diagnostics | Not clinically used |
Key Practical Points
- Organism excretion occurs in "showers" - intermittent shedding means a single negative stool does NOT exclude infection. At least 3 specimens over 3 days should be examined
- In chronic cases, stool may need to be collected weekly for 4-5 weeks for parasitologic confirmation
- Trophozoites disintegrate rapidly outside the host - only cysts survive in the environment and are the infective stage
- Immunoassay methods are generally superior to routine microscopy in sensitivity
- NAAT panels offer the highest sensitivity and can distinguish Giardia genotypes (assemblages), which is relevant for epidemiologic tracking
Source notes: Sherris & Ryan's Medical Microbiology, 8th Ed.; Medical Microbiology, 9th Ed.; Tietz Textbook of Laboratory Medicine, 7th Ed.; Symptom to Diagnosis, 4th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.