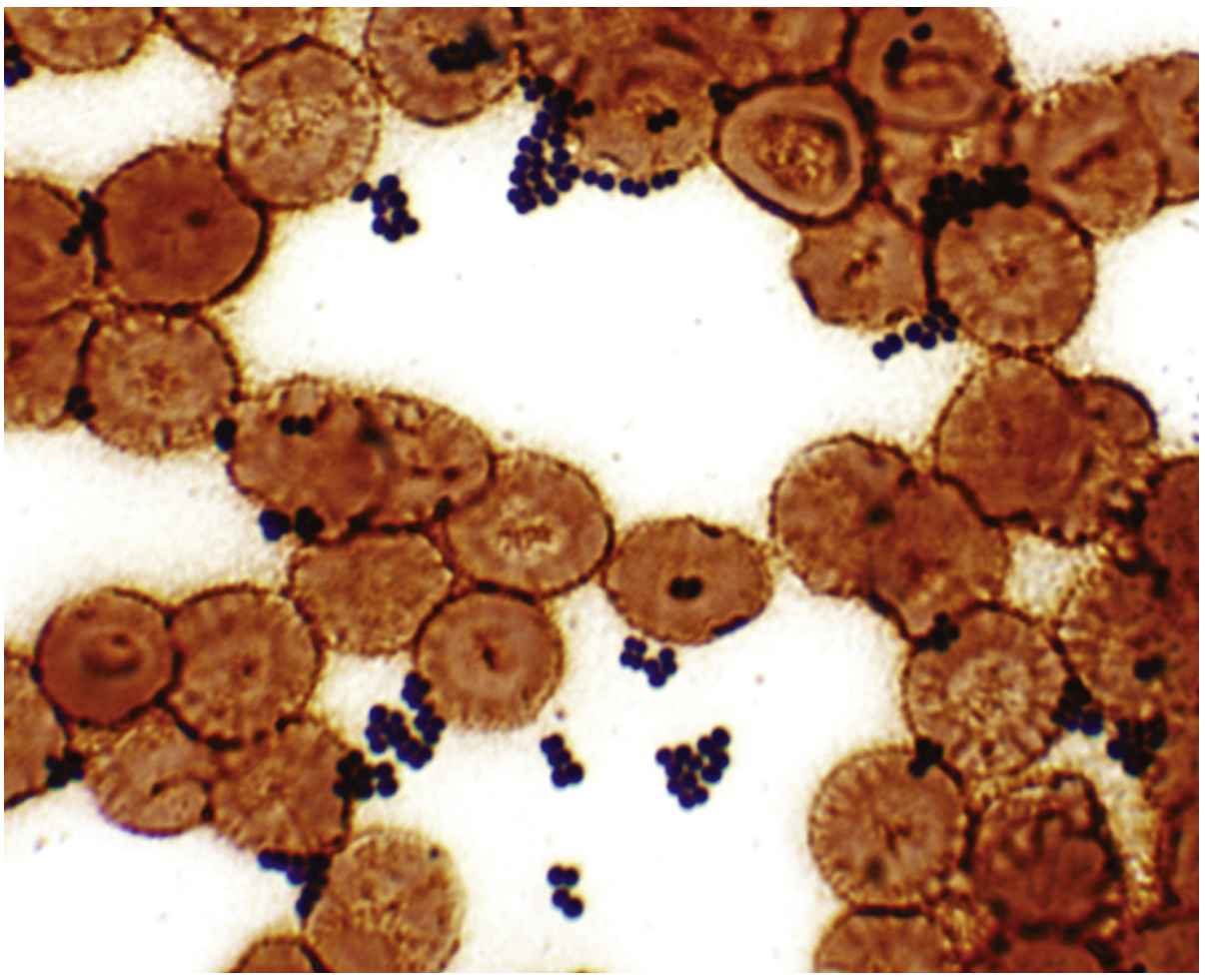
Staphylococcus aureus
"Staphylococcus aureus"[MeSH Terms] AND infections
Staphylococcus aureus
Microbiology
-
Catalase-positive (distinguishes from Streptococcus/Enterococcus)
-
Coagulase-positive (the defining feature separating it from coagulase-negative staphylococci)
-
Protein A expression on the cell surface
-
Colonies may appear yellow/gold due to carotenoid pigments (hence "aureus" = golden)
-
Grows across a wide range of conditions: aerobic and anaerobic, 18-40°C, up to 10% NaCl
-
Medical Microbiology 9e
Epidemiology
- Atopic dermatitis, eczema, chronic skin ulcers
- Insulin-dependent diabetes
- Patients on dialysis
- HIV infection
- Injection drug users
- Patients with intravascular catheters, prosthetic devices, or surgical wounds
- Goldman-Cecil Medicine, p. 3018-3020
Virulence Factors
| Category | Key Factor | Effect |
|---|---|---|
| Structural | Capsule | Inhibits phagocytosis |
| Protein A | Binds IgG Fc region; B-cell superantigen; evades antibody-mediated immunity | |
| Coagulase | Converts fibrinogen to fibrin; aids in abscess formation | |
| Toxins | α-Toxin (alpha-hemolysin) | Pore-forming; lyses host cells; provokes inflammation |
| Panton-Valentine Leukocidin (PVL) | Pore-forming; destroys leukocytes; associated with community-MRSA, necrotizing pneumonia, skin abscesses | |
| Exfoliative toxins A & B | Serine proteases; cleave desmoglein-1; cause Staphylococcal Scalded Skin Syndrome (SSSS) | |
| Toxic Shock Syndrome Toxin-1 (TSST-1) | Superantigen; massive cytokine release; multisystem shock | |
| Enterotoxins (A-E, G-I) | Heat-stable superantigens; cause food poisoning | |
| Enzymes | Staphylokinase | Fibrinolysis; aids invasion |
| Hyaluronidase | Breaks down connective tissue | |
| Lipases, nucleases | Tissue destruction | |
| Phenol-soluble modulins | PSMs | Cell lysis; inflammation - especially important in CA-MRSA |
- Medical Microbiology 9e; Goldman-Cecil Medicine
Clinical Diseases
Toxin-Mediated Diseases
| Disease | Toxin | Features |
|---|---|---|
| Staphylococcal food poisoning | Enterotoxins (heat-stable) | Rapid onset (1-6 h), severe vomiting, diarrhea, abdominal cramping; resolves within 24 h; no fever typical |
| Staphylococcal Scalded Skin Syndrome (SSSS / Ritter disease) | Exfoliative toxins A & B | Infants; perioral erythema progresses to bullae, widespread desquamation; no organisms in blisters |
| Toxic Shock Syndrome (TSS) | TSST-1, enterotoxins | Fever, hypotension, diffuse macular erythematous rash, multi-organ dysfunction; menstrual (tampon use) and non-menstrual forms |
Pyogenic (Suppurative) Infections
-
Skin & Soft Tissue: Impetigo, folliculitis, furuncles (boils), carbuncles, wound infections, cellulitis, necrotizing fasciitis, pyomyositis
-
Bacteremia: Primary source is often an intravascular catheter or skin infection; high mortality
-
Endocarditis: Both native valve (especially tricuspid in IV drug users) and prosthetic valve; aggressive, destructive course
-
Pneumonia: Consolidation, abscess formation; seen in very young, elderly, post-influenza patients; necrotizing pneumonia with septic shock (often PVL-positive MRSA) carries very high mortality
-
Osteomyelitis: Hematogenous spread; primarily affects metaphysis of long bones in children
-
Septic arthritis: Purulent joint effusion with pain and erythema
-
Meningitis: Typically device-associated (shunts)
-
Empyema
-
Medical Microbiology 9e; Goldman-Cecil Medicine
Diagnosis
| Method | Use |
|---|---|
| Gram stain | Useful for pyogenic infections (wound, joint, CSF); not sensitive for bacteremia |
| Culture | Grows rapidly on nonselective media; selective media (mannitol-salt agar, chromogenic agar) for contaminated specimens |
| Biochemical | Coagulase test (tube/slide) is definitive |
| MALDI-TOF mass spectrometry | Rapid species identification |
| Molecular/PCR | NAAT for MSSA and MRSA screening and confirmation; mecA gene detection for MRSA |
| Blood cultures | Mandatory when bacteremia or endocarditis suspected |
- Medical Microbiology 9e; Tietz Textbook of Laboratory Medicine
Antibiotic Resistance: MRSA
| Feature | Hospital-acquired MRSA (HA-MRSA) | Community-acquired MRSA (CA-MRSA) |
|---|---|---|
| SCCmec type | I, II, III (large) | IV, V (small) |
| PVL | Rare | Frequent |
| Multi-drug resistance | Common | Less common |
| Typical infection | Bacteremia, VAP, SSI | Skin abscesses, necrotizing pneumonia |
Treatment
MSSA (Methicillin-Susceptible S. aureus)
- Drug of choice: Antistaphylococcal penicillins (nafcillin, oxacillin) or cefazolin (equivalent efficacy, easier dosing - supported by recent 2025 meta-analysis [PMID 40349971])
- For penicillin allergy: cefazolin (unless anaphylaxis history), vancomycin
MRSA
| Setting | Options |
|---|---|
| Oral (mild-moderate) | TMP-SMX, doxycycline/minocycline, clindamycin, linezolid |
| IV (serious/invasive) | Vancomycin (drug of choice) - AUC/MIC-guided dosing preferred |
| Alternative IV | Daptomycin (especially bacteremia/endocarditis; some authorities prefer higher doses 8-10 mg/kg; NOTE: do not use for pneumonia - inactivated by surfactant) |
| Alternative IV | Linezolid, tigecycline, ceftaroline |
-
For food poisoning: symptomatic treatment only (toxin pre-formed in food; antibiotics not indicated)
-
Localized infections (abscesses): Incision and drainage is the primary intervention; antibiotics for systemic disease
-
A 2025 meta-analysis found oral antibiotic therapy is non-inferior to IV therapy for stable S. aureus bacteremia in select patients [PMID 39290168]
-
Medical Microbiology 9e; Goldman-Cecil Medicine; Harrison's Principles 22E
Prevention & Control
- Thorough hand hygiene (the cornerstone of hospital infection control)
- Contact precautions for MRSA-colonized/infected patients
- Proper wound care and disinfection
- Decolonization with intranasal mupirocin ± chlorhexidine bathing in high-risk patients (pre-surgical, dialysis, recurrent infections)
- Screening and isolation protocols in healthcare settings
- No approved S. aureus vaccine is currently in widespread clinical use
Recent Evidence Updates (2024-2025)
- Cefazolin vs. antistaphylococcal penicillins for MSSA bacteremia: A 2025 systematic review/meta-analysis (PMID 40349971) supports cefazolin as at least equivalent to oxacillin/nafcillin for MSSA bacteremia, with a potentially better safety profile.
- Oral step-down therapy for bacteremia: A 2025 meta-analysis (PMID 39290168) found oral antibiotics non-inferior to IV therapy for S. aureus bacteremia/endocarditis in stable patients meeting criteria for de-escalation, suggesting oral step-down is a viable strategy.
- MRSA comparative treatments: A 2024 network meta-analysis (PMID 38789000) compared six antibiotics for MRSA infections.
Clinical importance of staphylococcus aureus
Clinical importance of staphylococcus aureus In ENT
"Staphylococcus aureus"[MeSH Terms] AND "ear nose throat"[All Fields]
Clinical Importance of Staphylococcus aureus in ENT
1. The Ear
Acute Otitis Externa (AOE)
- Presents with rapid onset otalgia (worsened with pinna manipulation), pruritus, canal erythema, edema, and seropurulent discharge
- Progresses from pruritus with scant clear discharge to severe pain, canal occlusion, and conductive hearing loss
- Risk factors: swimming ("swimmer's ear"), narrow canals, eczema, seborrhea, ear plugs, hearing aid trauma, cerumen removal attempts
- Cummings Otolaryngology Head and Neck Surgery
Chronic Otitis Externa (COE)
- Cummings Otolaryngology
Necrotizing (Malignant) Otitis Externa
-
Seen in diabetics, immunocompromised patients, and the elderly
-
Infection spreads from the EAC into the surrounding soft tissues, cartilage, and bone, leading to osteomyelitis of the temporal bone and skull base
-
Complications include cranial nerve palsies (CN VII most common), intracranial spread, meningitis, and death
-
CT scanning demonstrates bony erosion
-
Treatment: systemic antibiotics active against causative organism (ciprofloxacin for Pseudomonas; vancomycin for MRSA); surgical debridement in refractory cases
-
Rosen's Emergency Medicine; Tintinalli's Emergency Medicine
Chronic Suppurative Otitis Media (CSOM)
Mastoiditis
- Rosen's Emergency Medicine
2. The Nose and Paranasal Sinuses
Nasal Colonization - The Reservoir
- Carriers have several-fold higher risk of developing S. aureus infection
- The nares serve as the source for autogenous infection (skin/soft tissue, surgical sites)
- Nasal carriage of S. aureus is associated with atopic dermatitis, eczema, and chronic skin conditions
Nasal Vestibulitis
Chronic Rhinosinusitis (CRS)
| Mechanism | Clinical Relevance |
|---|---|
| Biofilm formation | S. aureus and P. aeruginosa biofilms in the sinuses are associated with unfavorable post-surgical outcomes and treatment failure after FESS |
| Superantigen activity | S. aureus enterotoxins act as superantigens on mucosal T cells, driving massive polyclonal T-cell activation and eosinophilic inflammation |
| IgE to S. aureus enterotoxins | Serum IgE directed against S. aureus enterotoxins is elevated in patients with CRS and nasal polyps - linking bacterial colonization to type 2 eosinophilic disease |
| Loss of microbiome diversity | Chronically inflamed sinuses show decreased bacterial diversity with overgrowth of pathologic species including S. aureus |
- Goldman-Cecil Medicine; Murray & Nadel's Textbook of Respiratory Medicine; Cummings Otolaryngology
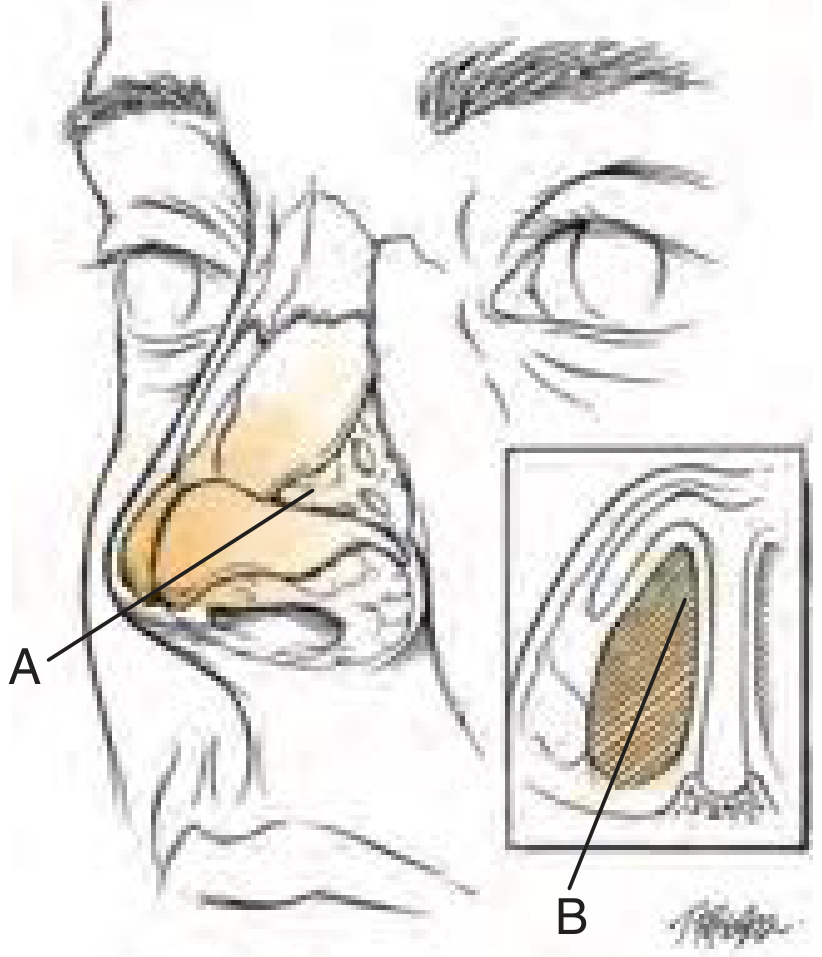
Nasal Septal Abscess
3. The Throat, Tonsils, and Pharynx
Peritonsillar Abscess (PTA)
-
Begins as acute exudative tonsillitis progressing to cellulitis and abscess
-
Presents with severe throat pain, trismus, "hot-potato" voice, uvular deviation
-
Treatment: needle aspiration or I&D + antibiotics covering streptococci, S. aureus, and anaerobes; tonsillectomy if recurrent
-
Pfenninger and Fowler's Procedures for Primary Care
Deep Neck Space Infections
4. Post-Surgical ENT Infections
- Patients with known nasal MRSA carriage (identified on pre-op screening)
- Healthcare workers and their contacts
- Revision surgeries
5. MRSA - Special ENT Considerations
| Feature | Detail |
|---|---|
| Community-associated MRSA (CA-MRSA) | Increasingly seen in skin and soft tissue infections of the head and neck (furunculosis, parotid abscess) |
| Biofilm | MRSA forms robust biofilms on ENT implants (osseointegrated implants, cochlear implants, tympanostomy tubes) |
| Screening | Nasal swab PCR/culture is the standard screening method for MRSA carriage |
| Decolonization | Mupirocin 2% nasal ointment BID x 5 days ± chlorhexidine body wash reduces carriage rates |
Summary Table: S. aureus in ENT
| Site | Condition | Role of S. aureus |
|---|---|---|
| Ear canal | Acute otitis externa | 2nd/3rd most common pathogen |
| Ear canal | Chronic otitis externa | Frequent isolate alongside Pseudomonas |
| Skull base | Necrotizing otitis externa | Important co-pathogen/alternative to Pseudomonas |
| Middle ear/mastoid | CSOM, mastoiditis | Recognized pathogen; MRSA emerging |
| Nasal vestibule | Vestibulitis, furuncle | Primary causative organism |
| Paranasal sinuses | Chronic rhinosinusitis + CRSwNP | Biofilm, superantigen, IgE mechanisms |
| Nasal septum | Septal abscess | Most common causative organism |
| Tonsils/pharynx | Peritonsillar abscess | Key aerobic pathogen (with GAS) |
| Deep neck | Parapharyngeal/retropharyngeal abscess | Polymicrobial contributor |
| Surgical wounds | Post-ENT SSI | Leading pathogen; MRSA concern |
Clinical importance of staphylococcus aureus In ENT
Clinical Importance of Staphylococcus aureus in ENT
THE EAR
Acute Otitis Externa (AOE) - "Swimmer's Ear"
- S. aureus is the 2nd/3rd most common bacterial isolate (after Pseudomonas aeruginosa); bacterial infections cause >90% of AOE cases
- Presents with rapid-onset otalgia worsened by pinna manipulation, canal erythema, edema, seropurulent discharge, and conductive hearing loss
- Risk factors: water exposure, narrow canals, eczema, hearing aids, cotton swab trauma
- Treatment: Topical fluoroquinolone drops (first-line); oral antibiotics are NOT effective for uncomplicated OE; aminoglycoside drops are contraindicated if TM is perforated
Chronic Otitis Externa (COE)
- Staphylococcal species (alongside Pseudomonas) are frequently cultured
- Contributes to granulation tissue, canal lichenification, and stenosis
- COE is bilateral in >50% of patients and affects 3-5% of the population
Necrotizing (Malignant) Otitis Externa
- Pseudomonas aeruginosa is the primary pathogen, but S. aureus (including MRSA) is an important alternative/co-pathogen
- Aggressive, life-threatening skull base osteomyelitis
- Seen almost exclusively in diabetics, immunocompromised, and elderly patients
- Complications: CN VII palsy (most common), meningitis, intracranial spread, death
- Diagnosis: CT showing bony erosion of temporal bone/skull base
- Treatment: Systemic antibiotics (vancomycin for MRSA); surgical debridement in refractory cases; co-management with ENT
Chronic Suppurative Otitis Media (CSOM)
- S. aureus is a recognized pathogen in persistent otorrhea through a perforated TM, alongside Pseudomonas and anaerobes
- MRSA is an emerging concern in treatment-resistant CSOM
- Often associated with cholesteatoma and middle ear destruction
Mastoiditis
- S. aureus is one of the key organisms in acute mastoiditis - the most common suppurative complication of otitis media
- Presents with postauricular erythema, tenderness, auricle protrusion, abnormal TM
- Treatment: Vancomycin IV empirically (covers MRSA); add anti-Pseudomonal coverage if previously antibiotic-treated; CT if intracranial involvement suspected; ENT consultation mandatory
THE NOSE AND PARANASAL SINUSES
Nasal Colonization - The ENT Reservoir
- The anterior nares are the primary ecological niche of S. aureus in humans
- ~20-30% of the general population are persistent nasal carriers
- ENT relevance:
- Carriers have several-fold higher risk of developing invasive S. aureus infection
- Nares serve as the autogenous source for surgical site infections
- Higher carriage rates in atopic dermatitis, eczema, and chronic sinusitis patients
Nasal Vestibulitis
- S. aureus is the primary causative organism
- Presents as erythema, crusting, and painful furuncles at the nasal entrance
- Risk factors: nose picking, nasal hair removal, nasal cannula use
- Treatment: Topical mupirocin 2%; systemic antibiotics for spreading cellulitis or recurrent disease
Nasal Septal Abscess
- S. aureus is the most common pathogen
- Complication of nasal trauma or untreated septal hematoma
- If untreated: septal cartilage necrosis → saddle-nose deformity
- Risk of intracranial spread (cavernous sinus thrombosis, meningitis)
- Treatment: Urgent surgical drainage + antibiotics
Chronic Rhinosinusitis (CRS) - A Multifaceted Role
| Mechanism | Clinical Impact |
|---|---|
| Biofilm formation | S. aureus biofilms in sinuses → treatment failure after FESS, poor surgical outcomes |
| Superantigen activity | Enterotoxins act as superantigens on mucosal T cells → polyclonal T-cell activation, massive eosinophilic inflammation → nasal polyp formation |
| IgE to S. aureus enterotoxins | Elevated serum IgE to enterotoxins in CRS with nasal polyps (CRSwNP) - links bacterial colonization to type 2 eosinophilic disease and severe asthma |
| Microbiome disruption | Chronically inflamed sinuses show loss of bacterial diversity with S. aureus overgrowth |
| Post-surgical recurrence | S. aureus carriage predicts polyp recurrence after endoscopic sinus surgery |
The S. aureus enterotoxin-superantigen mechanism is now recognized as a key driver in the pathogenesis of severe CRSwNP and comorbid asthma, making it a therapeutic target (e.g., anti-IgE therapy with omalizumab).
THE THROAT, TONSILS, AND PHARYNX
Peritonsillar Abscess (PTA)
- PTA is polymicrobial; S. aureus is one of the most common aerobic organisms alongside Streptococcus pyogenes (GAS); anaerobes include Bacteroides and Fusobacterium
- Progresses from acute tonsillitis → peritonsillar cellulitis → abscess
- Presents with severe odynophagia, trismus, "hot-potato" voice, uvular deviation to contralateral side
- Treatment: Needle aspiration or I&D (definitive) + antibiotics covering GAS, S. aureus, and anaerobes (amoxicillin-clavulanate or clindamycin; vancomycin if MRSA suspected)
Acute Epiglottitis
- While H. influenzae type b was historically the dominant pathogen, S. aureus (including MRSA) is now one of the important causes of adult epiglottitis in the post-Hib vaccine era
- Presents with dysphagia, drooling, muffled voice, and respiratory distress - a potential airway emergency
- Empirical antibiotics must cover S. aureus
Tonsillitis and Pharyngitis
- S. aureus contributes to recurrent and chronic tonsillitis, particularly in adults
- Found as part of the polymicrobial flora in tonsillar crypts
DEEP NECK SPACE INFECTIONS
| Space | Infection | Key Risk |
|---|---|---|
| Peritonsillar space | Peritonsillar abscess | Airway obstruction |
| Parapharyngeal space | Parapharyngeal abscess | Carotid artery erosion, IJV thrombosis |
| Retropharyngeal space | Retropharyngeal abscess | Airway compromise, mediastinitis |
| Submandibular space | Ludwig's angina (mixed flora) | Rapid airway loss |
POST-SURGICAL ENT INFECTIONS
| Procedure | Risk |
|---|---|
| Septoplasty / rhinoplasty | Nasal vestibulitis, septal abscess, implant infection |
| Functional endoscopic sinus surgery (FESS) | Biofilm-related recurrence, SSI |
| Tonsillectomy | Post-tonsillectomy wound infection (rare but serious) |
| Tympanostomy tube insertion | Otorrhea, CSOM |
| Cochlear implant / osseointegrated implants | Device infection, biofilm |
| Neck dissection / head and neck oncology | Wound breakdown, flap infection |
MRSA - Specific ENT Considerations
| Aspect | Detail |
|---|---|
| Community-MRSA (CA-MRSA) | Furunculosis, parotid abscess, skin/soft tissue infections of face and neck |
| Biofilm on implants | Cochlear implants, bone-anchored hearing aids, tympanostomy tubes |
| Nasal screening | Nasal swab PCR is gold standard for MRSA carriage detection |
| Decolonization | Mupirocin nasal ointment + chlorhexidine wash; repeat after 3 months if recolonization |
| Treatment of invasive MRSA | Vancomycin IV (AUC-guided dosing); daptomycin as alternative; oral step-down with TMP-SMX or doxycycline |
Summary: S. aureus Across ENT
| Region | Condition | Significance |
|---|---|---|
| External ear | AOE, COE | 2nd-3rd most common pathogen |
| Skull base | Necrotizing OE | Dangerous alternative to Pseudomonas; MRSA concern |
| Middle ear/mastoid | CSOM, mastoiditis | Persistent infection, MRSA emerging |
| Nasal vestibule | Vestibulitis, furuncle | Primary pathogen |
| Nasal septum | Septal abscess | Most common organism; cartilage-destructive |
| Paranasal sinuses | Chronic rhinosinusitis + CRSwNP | Biofilm + superantigen-IgE pathways |
| Tonsils/pharynx | PTA, epiglottitis | Key aerobic pathogen; MRSA causing adult epiglottitis |
| Deep neck | Parapharyngeal/retropharyngeal abscess | Life-threatening; surgical emergency |
| Postoperative | SSI after any ENT surgery | Leading pathogen; MRSA decolonization beneficial |
Total ossiculular reconstruction prosthesis - TORP and partial ossicular reconstruction prosthesis - PORP
"ossicular reconstruction"[MeSH Terms] AND prosthesis
"ossiculoplasty"[MeSH Terms] AND "TORP OR PORP"
ossiculoplasty TORP PORP hearing outcomes
Total Ossicular Reconstruction Prosthesis (TORP) and Partial Ossicular Reconstruction Prosthesis (PORP)
Definitions
| Prosthesis | Full Name | Indication |
|---|---|---|
| PORP | Partial Ossicular Replacement Prosthesis | Used when the stapes superstructure (head + crura) is intact; bridges from stapes head to tympanic membrane (or malleus) |
| TORP | Total Ossicular Replacement Prosthesis | Used when the stapes superstructure is absent; bridges from stapes footplate to tympanic membrane (or malleus) |
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Shambaugh Surgery of the Ear
Anatomy of the Normal Ossicular Chain (Why Reconstruction is Needed)
Ossicular Defect Classification (Austin/Kartush)
| Type | Malleus | Stapes Superstructure | Prosthesis Used |
|---|---|---|---|
| A | Present (M+) | Present (S+) | Sculpted incus, PORP, or incus interposition |
| B | Present (M+) | Absent (S-) | TORP |
| C | Absent (M-) | Present (S+) | PORP (TM directly to stapes head) |
| D | Absent (M-) | Absent (S-) | TORP (TM directly to footplate) |
The most commonly encountered ossicular defect is Type A (erosion of the long process of the incus with intact malleus and stapes), followed by types B, C, and D.
- Shambaugh Surgery of the Ear
How Each Prosthesis Works
PORP
- Sits with its base (cup/platform) on the stapes head (capitulum)
- Its shaft/head contacts the underside of the TM or the medial surface of the malleus manubrium
- Transmits vibrations: TM → PORP → stapes capitulum → stapes footplate → oval window → cochlea
- Effective length: typically ~2.0-2.5 mm
TORP
- Sits with its base directly on the stapes footplate
- Its shaft/head contacts the underside of the TM or malleus
- Used when the stapes crura are destroyed (e.g., by cholesteatoma, chronic OM, trauma)
- Effective length: typically ~3.5-4.5 mm (longer than PORP as it spans greater distance)
- Generally achieves slightly poorer hearing results than PORP due to the longer lever arm and absence of the stapes superstructure's natural amplification
Materials Used
1. Plastipore (High-Density Polyethylene Sponge - HDPS)
- First dedicated PORP and TORP (Sheehy, 1976)
- Porous structure encourages tissue ingrowth (fibrocytes, small round cells)
- Extrusion rates: 3-5% over 5-10 years (most within first year)
- Requires cartilage interposition to minimize extrusion
- Still used widely; preferred by ~16% of US otologists in surveys
- Shambaugh Surgery of the Ear
2. Hydroxylapatite (HA)
- Bioactive calcium phosphate material chemically similar to bone
- Promotes osseointegration - direct bone contact with the implant
- Excellent biocompatibility; minimal reactive fibrosis; can tolerate direct TM contact
- However, extrusion with thin TM reported in ~16% if no cartilage interposition
- Can fracture during trimming due to brittleness; use a diamond burr with copious irrigation
- Available in dense and porous forms; preferred by ~48% of US otologists
- Shambaugh Surgery of the Ear
3. Titanium
- Introduced by Stupp in 1993
- Lightweight, strong, excellent biocompatibility, tendency to osseointegrate
- Allows laser-cut precision designs (e.g., self-securing clips, complex cup designs)
- Can be MRI-compatible (non-ferromagnetic grades)
- Does extrude when in direct contact with TM - cartilage interposition is mandatory
- Now one of the two most commonly used materials (alongside HA)
- Shambaugh Surgery of the Ear
4. Other/Historical Materials
| Material | Notes |
|---|---|
| Homograft ossicles | Excellent biocompatibility; abandoned due to risk of viral/prion transmission |
| Wire prostheses (stainless steel, platinum, tantalum) | Better tolerated than early plastics; problems with displacement |
| Bioglass (ceramic) | Higher extrusion (~8%) and fragmentation; largely abandoned |
| Bone cement (hydroxylapatite/calcium phosphate) | Used for limited incus erosion; fills small gaps |
| Hybrid prostheses | HA head + Plastipore or Teflon shaft; combines TM tolerance with shaft flexibility |
Surgical Principles: The TRACS Mnemonic
| Letter | Principle | Detail |
|---|---|---|
| T | Tension | Prosthesis should be slightly longer than the gap, providing gentle tension; too lax = sound energy loss; too tight = dampening |
| R | Round window protection | Round window must be isolated; simultaneous equal waves to oval and round windows cancel out (hearing loss) |
| A | Angle | Prosthesis must contact TM at 45-90 degrees; more acute angle = hearing loss; PORP/TORP should be as vertical as possible |
| C | Centered | Contact point on TM should be as central as possible (maximum vibratory amplitude); placing near the annulus dampens transmission |
| S | Space | Middle ear airspace must be >0.3 mL (normal ~1 mL); reconstruction of this space prevents adhesions |
Cartilage Interposition - Why It Matters
-
Reduces extrusion risk - the most important complication of ossiculoplasty
-
Augments the prosthesis-tissue interface for better long-term hearing
-
Particularly essential with titanium and in thin/atrophic TMs
-
Can be partial or full thickness
-
Also indicated in: revision surgery, perforations >50%, drainage at surgery, bilateral perforations, post-cholesteatoma reconstruction
-
Cummings Otolaryngology
Hearing Outcomes
| Prosthesis | Expected Air-Bone Gap (ABG) closure to within 20 dB |
|---|---|
| PORP | ~60-70% of cases |
| TORP | ~40-55% of cases (generally less predictable) |
| Traumatic disruption (IS joint repair) | ABG closure within 10 dB in 78% (best outcomes) |
| Sculpted incus interposition (Type A) | ABG within 20 dB in 68% |
- The longer column is more susceptible to displacement
- Loss of the stapes superstructure removes natural lever amplification
- Footplate contact is technically more demanding
-
Eustachian tube dysfunction (atelectasis, negative middle ear pressure)
-
Active middle ear infection at the time of surgery
-
Absence of malleus (no support for prosthesis)
-
Thin/atrophic TM
-
Revision surgery
-
Cummings Otolaryngology; Shambaugh Surgery of the Ear
Complications
| Complication | Notes |
|---|---|
| Extrusion | Most common long-term complication; occurs in 3-16% depending on material and TM status; most within 1st year; prevented by cartilage cap |
| Displacement/migration | Can occur with poor tension or inadequate fixation; causes recurrent CHL |
| Residual/recurrent CHL | Failure to close ABG; most common functional outcome issue |
| Sensorineural hearing loss | Rare; may occur from excessive footplate pressure (TORP) or perilymph fistula |
| Tympanic membrane re-perforation | Due to extrusion or graft failure |
| Middle ear fibrosis/adhesions | Inadequate middle ear space, poor ET function |
| Infection / otitis media | Can lead to prosthesis contamination and failure |
Surgical Timing and Staging
- Stage 1: Disease removal (cholesteatoma, granulation tissue) + TM repair; a Silastic sheet or cartilage may be placed over the footplate to maintain middle ear space
- Stage 2 (6-12 months later): Ossiculoplasty with PORP/TORP once the middle ear is healed, dry, and well-aerated
Recent Developments (2024-2025)
- TORP-PORP hybrid technique (PMID 38361297, Otol Neurotol 2024): A novel technique for isolated stapes suprastructure defects where a TORP is modified to function as a PORP - addressing the Austin Type A defect when stapes superstructure is partially destroyed
- Bone vs titanium prostheses (PMID 38932647, Clin Otolaryngol 2024): A nationwide register-based study found similar hearing outcomes between autologous bone and titanium prostheses
- Long-term ossiculoplasty outcomes (PMID 40567078, Acta Otolaryngol 2025): Long-term data continues to support titanium as a durable option with good hearing gains
Quick Reference Summary
PORP: Stapes head → PORP → TM (stapes superstructure INTACT)
TORP: Stapes footplate → TORP → TM (stapes superstructure ABSENT)
Materials: Titanium (most common) | Hydroxylapatite | Plastipore
Key step: ALWAYS place cartilage between prosthesis head and TM
Goal: Air-bone gap < 20 dB postoperatively
TRACS: Tension | Round window | Angle | Centered | Space
Total ossiculular reconstruction prosthesis - TORP and partial ossicular reconstruction prosthesis - PORP
TORP and PORP - Ossicular Reconstruction Prostheses
Core Definitions
| Prosthesis | Stands For | Stapes Status | Bridges |
|---|---|---|---|
| PORP | Partial Ossicular Replacement Prosthesis | Stapes superstructure INTACT | Stapes head → TM (or malleus) |
| TORP | Total Ossicular Replacement Prosthesis | Stapes superstructure ABSENT | Stapes footplate → TM (or malleus) |
Background and History
- Normal ossicular chain (malleus - incus - stapes) provides ~27 dB of mechanical gain; disruption causes conductive hearing loss of 40-60 dB
- The long process of the incus is the most commonly eroded ossicle (poor blood supply; most vulnerable to chronic OM and cholesteatoma)
- Wullstein (1952) first classified tympanoplasty types I-V based on ossicular status
- Sheehy (1976) introduced the first dedicated PORP and TORP made from Plastipore (high-density polyethylene sponge)
- The terms TORP/PORP were popularized by Brackmann and Sheehy in their landmark 1979 paper (Laryngoscope)
Ossicular Defect Classification (Austin/Kartush)
| Type | Malleus Handle | Stapes Superstructure | Reconstruction |
|---|---|---|---|
| A (most common) | Present | Present | Sculpted incus, incus interposition, or PORP |
| B | Present | Absent | TORP |
| C | Absent | Present | PORP (TM to stapes head directly) |
| D | Absent | Absent | TORP (TM to footplate directly) |
Wullstein Tympanoplasty Classification (Relevant to Prosthesis Selection)
| Type | Description | Modern Application |
|---|---|---|
| I | Myringoplasty only; ossicular chain intact | No prosthesis needed |
| II | Manubrium eroded; TM draped onto incus long process | Rarely used today |
| III | TM/graft onto stapes capitulum | Minor columella = PORP; Major columella = TORP |
| IV | TM onto stapes footplate; round window protected | Direct footplate contact; no prosthesis |
| V | TM over lateral semicircular canal fenestration | Rarely performed |
Type III tympanoplasty with a PORP or TORP is the most commonly performed ossiculoplasty today.
PORP - Detailed
When to Use
- Stapes superstructure (head + crura) is intact
- Malleus may or may not be present
- Incus is absent or non-functional
Mechanism
Tympanic Membrane → PORP head → PORP shaft → cup on stapes capitulum → footplate → oval window → cochlea
Dimensions
- Typical length: ~2.0-2.5 mm
- The cup/platform base engages the stapes capitulum
- Head contacts TM (preferably with cartilage cap interposed)
Hearing Results
- Air-bone gap closure to within 20 dB in approximately 60-70% of cases
- Better results when malleus is preserved (prosthesis angulation is more favorable)
TORP - Detailed
When to Use
- Stapes superstructure is absent (destroyed by cholesteatoma, chronic OM, trauma, or surgery)
- Only the stapes footplate remains
- Malleus may or may not be present
Mechanism
Tympanic Membrane → TORP head → TORP shaft → base on stapes footplate → oval window → cochlea
Dimensions
- Typical length: ~3.5-4.5 mm (longer than PORP to reach footplate)
- Base must be stable and centered on the footplate (not on annular ligament)
Hearing Results
- Air-bone gap closure to within 20 dB in approximately 40-55% of cases
- Less predictable than PORP due to:
- Longer lever arm = more displacement risk
- Loss of natural stapes superstructure amplification
- Footplate contact technically more demanding
- Risk of perilymph fistula from excessive footplate pressure
Prosthesis Materials
1. Plastipore (HDPS - High-Density Polyethylene Sponge)
- First material used (Sheehy, 1976)
- Porous structure allows fibrous tissue ingrowth
- Biocompatible, non-reactive
- Extrusion rate: 3-5% at 5-10 years (most in year 1)
- Cartilage cap mandatory to reduce extrusion
- Still preferred by ~16% of US otologists
2. Hydroxylapatite (HA)
- Calcium phosphate composition similar to bone; bioactive
- Promotes osseointegration; minimal reactive fibrosis
- Most biocompatible material for TM contact
- Extrusion rate with thin TM if no cartilage: up to 16%
- Brittle - trim carefully with diamond burr + copious irrigation
- Preferred by ~48% of US otologists (most popular overall)
- Available in dense and porous forms
3. Titanium
- Introduced by Stupp, 1993
- Lightweight, strong, precise (laser-cut designs possible)
- Excellent biocompatibility; osseointegrates
- Self-securing clip designs improve intraoperative stability
- MRI-compatible (non-ferromagnetic)
- Extrudes without cartilage - cartilage interposition is mandatory
- Now one of the two most commonly used materials (alongside HA)
4. Other Materials (Historical/Adjunctive)
| Material | Status | Notes |
|---|---|---|
| Homograft ossicles | Largely abandoned | Risk of viral/prion transmission |
| Stainless steel / platinum wire | Historical | Displacement issues |
| Bioglass (ceramic) | Abandoned | 8% extrusion; fragmentation |
| Bone cement (HA/CaPO4) | Adjunctive | For small incus erosions; fills gaps |
| Hybrid (HA head + Teflon/Plastipore shaft) | Still used | Combines TM tolerance with shaft flexibility |
Cartilage Interposition - The Critical Step
- Reduces extrusion (the most important long-term complication)
- Provides structural support to thin or atrophic TM
- Improves long-term stability of prosthesis-TM interface
- Especially essential with titanium (mandatory) and in high-risk TMs
- Thin, atrophic, or retracted TMs
- Titanium prostheses (all cases)
- Revision surgery
- Perforation >50% of TM
- Discharge present at time of surgery
- Post-cholesteatoma reconstruction
- Bilateral perforations
The TRACS Principles (Surgical Biomechanics)
| Letter | Principle | Key Points |
|---|---|---|
| T | Tension | Prosthesis slightly longer than gap = gentle tension; too lax = energy loss; too tight = damping; test by gently displacing - should return to position |
| R | Round window | Must be isolated/protected; simultaneous equal sound pressure on both oval and round windows cancels out (destructive interference = hearing loss) |
| A | Angle | Contact angle with TM must be 45-90°; more acute = hearing loss; PORP and TORP should be positioned as vertical as possible |
| C | Centered | Contact point should be as central on TM as possible (maximum excursion zone); too peripheral dampens sound; preserve manubrium when possible |
| S | Space | Middle ear airspace must be >0.3 mL; reconstruct air pocket to prevent adhesions; consider tympanostomy tube if ET function remains poor |
Indications for Ossiculoplasty
- Chronic otitis media with ossicular erosion (most common)
- Cholesteatoma surgery (staged or single-stage)
- Traumatic ossicular disruption (incudostapedial joint dislocation, incus dislocation)
- Tympanosclerosis with ossicular fixation
- Congenital ossicular anomalies
- Failed previous ossiculoplasty
- Dry ear (no active infection) for at least 3 months (or staged approach)
- Adequate Eustachian tube function (or plan for tympanostomy tube)
- Conductive hearing loss >30 dB ABG
- Contralateral ear hearing adequate enough to make surgery meaningful
Surgical Staging
Single-stage ossiculoplasty
- Disease removal + ossicular reconstruction at one operation
- Appropriate when: limited disease, dry ear, good ET function, intact TM
Two-stage ossiculoplasty (preferred for cholesteatoma / complex disease)
- Stage 1: Remove disease, repair TM; place Silastic sheet or cartilage to maintain middle ear space; may place a "blind" PORP/TORP under the cartilage
- Stage 2 (6-12 months later): Second-look for residual cholesteatoma + formal ossiculoplasty in a healed, well-aerated middle ear
Hearing Outcome Benchmarks
| Scenario | ABG Closure Target | Expected Success Rate |
|---|---|---|
| PORP (any cause) | Within 20 dB | ~60-70% |
| TORP (any cause) | Within 20 dB | ~40-55% |
| Traumatic IS joint dislocation | Within 10 dB | ~78% |
| Sculpted incus interposition | Within 20 dB | ~68% |
| Chronic OM with cholesteatoma | Within 20 dB | ~50-60% |
- Active middle ear infection / wet ear
- Eustachian tube dysfunction / atelectasis
- Absent malleus (no support)
- Thin / atrophic TM
- Revision surgery
- Presence of cholesteatoma matrix
Complications
| Complication | Rate / Notes |
|---|---|
| Extrusion | 3-16%; most within year 1; material and cartilage-dependent |
| Displacement/migration | Recurrent CHL; poor tension or fixation |
| Residual CHL | Failure to close ABG; most common functional failure |
| SNHL | Rare; excessive footplate pressure (TORP) → perilymph fistula |
| TM re-perforation | Extrusion-related or graft failure |
| Middle ear fibrosis | Inadequate airspace, poor ET function |
| Infection | May lead to prosthesis failure; MRSA an emerging concern |
Quick Reference
PORP → Stapes superstructure INTACT → Head on stapes capitulum
TORP → Stapes superstructure ABSENT → Base on stapes footplate
Best material: Titanium or Hydroxylapatite
Always use: Cartilage cap between prosthesis and TM
Best results: Traumatic IS joint dislocation (78% within 10 dB)
PORP > TORP in hearing outcomes
Goal: ABG < 20 dB postoperatively
Mnemonic: TRACS (Tension, Round window, Angle, Centered, Space)
Virtual endoscopy in ENT
virtual endoscopy ENT otolaryngology sinuses larynx
"virtual endoscopy" paranasal sinuses OR larynx OR temporal bone
"virtual endoscopy" AND ("nasal cavity" OR "paranasal sinus" OR "larynx" OR "temporal bone" OR "ear")
PMID: 41264375
virtual endoscopy ENT applications paranasal sinuses larynx temporal bone cochlear implant 2024 2025
PMID: 40638414
Virtual Endoscopy in ENT
Definition and Concept
- Thin-section volumetric CT (or MRI) data is acquired
- DICOM data is processed using specialized software (e.g., OsiriX, 3D Slicer, Syngo.via, Voxar 3D)
- Surface rendering or volume rendering algorithms generate a photorealistic intraluminal view
- The virtual camera is navigated ("flown") through the airway or cavity
"Virtual endoscopy is a computer-generated simulation of endoscopic perspective. The virtual endoscopic images of the trachea, larynx, pharynx, nasal cavity, paranasal sinuses, and ear have demonstrated clinical utility."
- Cummings Otolaryngology Head and Neck Surgery
Technical Basis
Imaging Modalities Used
| Modality | Strengths for VE | Limitations |
|---|---|---|
| MDCT (Multi-detector CT) | Superior spatial resolution for bony detail; fast acquisition; thin slices (<1 mm); standard for VE | Radiation dose; limited soft tissue contrast |
| MRI | Excellent soft tissue contrast; no radiation; useful for soft tissue structures | Longer acquisition time; movement artifact; lower bony resolution |
| Cone-beam CT (CBCT) | Lower radiation; good for temporal bone/sinus VE | Limited soft tissue contrast |
Software Processing Steps
- Segmentation - identify the target hollow structure by thresholding (e.g., air density -1000 to -500 HU)
- Surface/volume rendering - generate a 3D model of the internal lumen surface
- Path planning - define a virtual camera flight path through the lumen
- Navigation - automated or manual fly-through with real-time rendering
- Correlation - simultaneous display of VE view with axial/coronal/sagittal 2D images
ENT Applications - By Region
1. Nasal Cavity and Paranasal Sinuses
- Pre-operative planning for Functional Endoscopic Sinus Surgery (FESS) - visualize sinus ostia, uncinate process, ethmoid labyrinth, and critical landmarks before actual endoscopy
- Evaluation of chronic rhinosinusitis and extent of sinonasal disease
- Assessment of nasal polyps and their extent into posterior sinuses
- Detection of sinonasal tumors - define extent, relationship to orbit, skull base, and cribriform plate
- Choanal atresia - evaluate patency and type (bony vs membranous) without instrumentation (especially useful in neonates)
- Assessment after prior surgery (anatomical distortion makes physical endoscopy harder to interpret)
- Can visualize areas inaccessible to conventional endoscopy (e.g., frontal recess, posterior ethmoids, sphenoid sinus)
- Overcomes patient discomfort/non-cooperation (especially pediatric patients)
- No risk of mucosal trauma or epistaxis
- Can be performed retrograde (from posterior to anterior)
- Cummings Otolaryngology
2. Larynx and Trachea (Virtual Laryngoscopy / Virtual Bronchoscopy)
- Laryngotracheal stenosis (LTS): CT with multiplanar reconstruction and VE is "highly accurate for detecting LTS" - can define the level (supraglottis, glottis, subglottis, trachea), length, and degree of stenosis for preoperative planning (Radiographics 2025, PMID 40638414)
- Laryngeal tumors: Assess subglottic extension, transglottic spread, and relationship to cartilage; plan partial laryngectomy vs total laryngectomy
- Post-intubation/post-tracheostomy stenosis: Quantify severity and plan dilation, resection, or stenting
- Foreign body (especially in children): Localise position before removal
- Vocal cord pathology: Adjunctive to conventional laryngoscopy; especially when airway is critically compromised and direct laryngoscopy is risky
- Congenital airway anomalies: Subglottic hemangioma, congenital subglottic stenosis, vascular rings
| Feature | Virtual Endoscopy | Direct Laryngoscopy |
|---|---|---|
| Invasiveness | Non-invasive | Invasive |
| Anaesthesia required | No | Often yes |
| Biopsy capability | No | Yes |
| Submucosal detail | Poor | Good |
| Bony/cartilaginous detail | Excellent | Poor |
| Area distal to stenosis | Visualized | Often not accessible |
| Dynamic assessment | No (static CT) | Yes |
| Risk to airway | None | Present in severe stenosis |
VE is particularly valuable for evaluating the airway distal to a stenosis - a region that may be completely inaccessible to direct endoscopy but is critical for surgical planning.
3. The Ear - Temporal Bone Virtual Endoscopy
- Assess stenosis (canal atresia, inflammatory stenosis)
- Evaluate extent of canal cholesteatoma
- Virtual otoscopy of the tympanic membrane
- Assess ossicular chain integrity (especially useful in congenital anomalies)
- Planning for cochlear implantation: A 2026 prospective study (PMID 41264375, Otol Neurotol) used CT-based VE to predict round window (RW) accessibility during cochlear implant surgery - achieving 96% accuracy with excellent inter-rater reliability (ICC 0.971). Virtual posterior tympanotomy and mastoidectomy were simulated using OsiriX software on DICOM data. This is now considered a valid, reliable, and reproducible preoperative tool.
- Assess anatomical variants relevant to surgery: high jugular bulb, aberrant ICA, dehiscent facial nerve canal
- Virtual endoscopy of the cochlea and semicircular canals (using ultra-thin CT or MRI)
- Planning electrode insertion for cochlear implants
- Visualize cochlear malformations (Mondini, incomplete partition, common cavity)
4. Skull Base and Deep Neck
- Map extent of skull base tumors (glomus jugulare, acoustic neuroma, chordoma)
- Evaluate relationship of tumor to ICA, jugular vein, facial nerve
- Plan endoscopic skull base surgery approaches (transsphenoidal, transnasal, transpterygoid corridors)
- Assess post-treatment anatomy and recurrence
5. Head and Neck Oncology
- Nasopharynx: Evaluate nasopharyngeal carcinoma extent; assess skull base invasion
- Oropharynx/hypopharynx: Assess tumor margins, pyriform fossa extension, cricopharyngeus
- Salivary duct VE (virtual sialendoscopy): CT or MRI-based visualization of parotid and submandibular ducts for sialolithiasis and stenosis - adjunct to actual sialendoscopy
Advantages of Virtual Endoscopy in ENT
| Advantage | Clinical Impact |
|---|---|
| Non-invasive | Safe in critically ill, uncooperative, or pediatric patients |
| No anaesthesia | Reduces procedural risk |
| Retrograde navigation | Can visualize distal to obstructions |
| Simultaneous 2D correlation | Click on VE view to see exact axial/coronal/sagittal slice |
| Reproducible and shareable | Can be reviewed, re-navigated, and shared with surgical team |
| Pre-surgical rehearsal | Surgeon can "practice" the endoscopic approach before actual surgery |
| Teaching tool | Excellent for anatomy teaching and trainee preparation |
| No radiation beyond diagnostic CT | Uses existing diagnostic imaging data |
| 3D spatial understanding | Particularly valuable for complex anatomy (skull base, petrous apex, frontal recess) |
Limitations of Virtual Endoscopy
| Limitation | Detail |
|---|---|
| No tissue sampling | Cannot perform biopsy - still requires actual endoscopy if tissue diagnosis needed |
| No mucosal color/texture | Cannot assess mucosal inflammation, vascular lesions, early dysplasia |
| Static imaging | Does not capture dynamic function (vocal cord movement, Eustachian tube opening, swallowing) |
| Radiation exposure | CT-based VE carries radiation dose (though within diagnostic range) |
| Spatial resolution limits | Very small structures (e.g., individual ossicular ligaments) may not be resolved |
| Software expertise required | Requires trained radiologist or surgeon to navigate and interpret |
| Artefacts | Dental amalgam, motion, beam hardening can degrade image quality |
| Cost | Post-processing software and workstation costs; not universally available |
| Cannot replace biopsy | Mucosal abnormalities detected on VE always require conventional endoscopy + biopsy to exclude malignancy |
Comparison: Virtual Endoscopy vs. Conventional Endoscopy
| Feature | Virtual Endoscopy (VE) | Conventional Endoscopy |
|---|---|---|
| Invasiveness | Non-invasive | Invasive |
| Patient tolerance | Excellent | Variable (discomfort, gag) |
| Biopsy | No | Yes |
| Mucosal colour assessment | No | Yes |
| Dynamic function | No | Yes |
| Inaccessible areas | Accessible | Often not accessible |
| 3D bony/anatomical detail | Excellent | Poor |
| Image-guided surgery integration | Yes | Partial |
| Real-time intraoperative use | No | Yes |
| Cost and availability | Higher/specialized | Lower/widely available |
Recent Advances (2024-2026)
| Development | Reference |
|---|---|
| CT-VE for cochlear implant round window prediction - 96% accuracy in prospective study of 40 patients; virtual mastoidectomy and posterior tympanotomy simulated preoperatively | PMID 41264375 (Otol Neurotol 2026) |
| CT multiplanar reconstruction + VE for laryngotracheal stenosis - now considered highly accurate for LTS detection and classification; essential for preoperative planning of airway reconstruction | PMID 40638414 (Radiographics 2025) |
| AI-assisted navigation - machine learning algorithms now being integrated into VE software for automated segmentation and path planning | |
| 3D printing from VE data - VE models used to generate physical 3D-printed anatomical models for surgical rehearsal |
Clinical Workflow Example: VE for Pre-FESS Planning
1. Obtain thin-section CT sinuses (coronal + axial, <1 mm slices, no contrast)
2. Load DICOM data into VE workstation (OsiriX, Syngo.via, etc.)
3. Segment air-filled nasal cavity and sinuses
4. Navigate virtual camera from nasal vestibule → choana:
- Assess inferior turbinate, middle meatus, uncinate process
- Identify and grade ostiomeatal complex obstruction
- Visualize frontal recess anatomy (agger nasi cells, frontal cells)
- Assess maxillary, ethmoid, sphenoid ostia
5. Correlate each VE view with corresponding 2D CT slice
6. Document anatomical variants (Onodi cell, Haller cell, paradoxical turbinate,
Keros classification of cribriform plate depth)
7. Use same CT dataset for intraoperative navigation (IGS) during FESS
Summary
- Pre-surgical planning for FESS, laryngotracheal reconstruction, and cochlear implantation
- Assessment of stenoses and obstructions inaccessible to conventional endoscopy
- Pediatric ENT where physical endoscopy is difficult
- Skull base surgery where 3D spatial orientation is critical
- Teaching and simulation
Ocular coherence tomography and its uses in ENT
optical coherence tomography otolaryngology ENT middle ear larynx
"optical coherence tomography" AND ("middle ear" OR "larynx" OR "tympanic membrane" OR "cochlea" OR "sinuses")
PMID: 38370517
PMID: 37253962
PMID: 39165857
"optical coherence tomography" AND ("laryngeal cancer" OR "vocal cord" OR "cholesteatoma" OR "eustachian tube" OR "cochlear implant")
PMID: 40178817
PMID: 36357503
Optical Coherence Tomography (OCT) and Its Uses in ENT
What is OCT?
"OCT is an analogue of ultrasound, using light instead of sound to produce a high (micrometre) resolution cross-sectional image, similar to a vertical histological section."
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Physical Principles
How OCT Works
| Step | Detail |
|---|---|
| Light source | Near-infrared broadband light (800-1300 nm); longer wavelengths penetrate deeper |
| Beam splitting | Light split into a sample beam (directed at tissue) and a reference beam (directed at a mirror of known path length) |
| Interferometry | Back-reflected light from tissue is combined with reference beam; interference pattern encodes the depth and intensity of reflections from each tissue layer |
| Why interferometry? | Speed of light is so fast that direct echo time measurement (as in ultrasound) is impossible; interferometry circumvents this by comparing path lengths |
| A-scan | A single depth profile at one point (analogous to a single ultrasound A-scan) |
| B-scan | Multiple A-scans combined = a 2D cross-sectional image |
| 3D OCT | Stack of B-scans = volumetric dataset |
OCT System Types
| Type | Mechanism | Advantages |
|---|---|---|
| Time-domain OCT (TD-OCT) | Reference mirror moves mechanically | Original technology; slower |
| Spectral-domain OCT (SD-OCT) | Fourier transform of spectral interference; no moving mirror | Faster, higher sensitivity; now standard |
| Swept-source OCT (SS-OCT) | Wavelength-swept laser source | Deeper penetration; faster; better for middle ear |
| OCT-Vibrometry | Detects sub-nanometer sound-induced vibrations in addition to imaging | Quantify ossicular and cochlear mechanics |
OCT Characteristics Relevant to ENT
| Parameter | Value |
|---|---|
| Axial resolution | 2-15 µm (near-histological) |
| Lateral resolution | 10-50 µm |
| Imaging depth | 1-3 mm in soft tissue (limited by optical scattering) |
| Acquisition speed | Real-time (thousands of A-scans/second) |
| Ionizing radiation | None |
| Contact required | No (non-contact for most systems) |
| Biopsy capability | No (optical biopsy only) |
ENT Applications
1. THE EAR - Most Clinically Developed ENT Application
A. Tympanic Membrane (TM) Imaging
- TM layers (epithelial, fibrous, mucosal layers)
- TM thickness measurement
- Myringosclerosis and tympanosclerosis plaques (depth and extent)
- Perforations and their margins
- Retraction pockets and their depth
- Cholesteatoma vs. serous effusion behind an intact TM
B. Middle Ear Effusion - Otitis Media
- Non-invasively visualize and characterize MEEs (serous vs. mucoid vs. purulent) based on optical backscattering
- Detect TM-adherent biofilms - a 2023 observational study (PMID 37253962) of 53 pediatric OM patients showed 89.6% had TM-adherent biofilm visible on OCT prior to tube surgery; this correlated with surgical findings
- Quantify MEE characteristics (viscosity, depth) that correlate with surgical outcome
- Distinguish otitis media with effusion (OME/"glue ear") from acute OM without tympanotomy
- Guide timing of tympanostomy tube insertion
C. OCT-Vibrometry - Middle and Inner Ear Mechanics
- Measure TM, ossicular chain, and round window vibration amplitudes and phases
- Map basilar membrane mechanics within the cochlea
- Quantify the functional impact of ossicular pathology (fixation, discontinuity)
- Assess stapes footplate motion in otosclerosis
- Evaluate cochlear partition mechanics in sensorineural hearing loss research
"OCT can be used as a vibrometry system capable of detecting sound-induced sub-nanometer vibrations of the middle and inner ear... the largest clinical impact of OCT for otology is to visualize various pathologies and quantify sound conduction and processing in the individual peripheral human ear."
- Seminars in Hearing 2024 (PMID 38370517)
D. Cholesteatoma Assessment
- Distinguish cholesteatoma keratin matrix from granulation tissue and effusion
- Assess depth of invasion into the mesotympanum
- A 2025 JAMA Otolaryngology study (PMID 40178817) fused middle ear OCT with CT images using rigid coregistration - finding that OCT revealed soft tissue features (e.g., cholesteatoma margins, traumatic middle ear injury detail) not apparent on CT, while CT provided superior bony overview; the two modalities were complementary
E. Cochlear Implant Surgery - A Major Emerging Application
- Pre-insertion planning: OCT-based atlas of the cochlear hook region (PMID 36615042) enables detailed visualization of scala tympani dimensions and cochlear anatomy
- Intraoperative real-time guidance: An optically-guided cochlear implant sheath integrating a fiber-optic OCT probe (PMID 36357503, Sci Rep 2022) provides real-time feedback during electrode insertion - the surgeon can detect cochlear walls (modiolar wall, osseous spiral lamina, basilar membrane) ahead of the advancing electrode and adjust trajectory in real time to prevent intracochlear trauma
- Post-insertion verification: Transtympanic OCT can confirm electrode positioning after insertion (PMID 35970156, Otol Neurotol 2022)
2. THE LARYNX - Optical Biopsy for Cancer

| Clinical Use | Detail |
|---|---|
| Benign vs. malignant discrimination | OCT images epithelial thickness, layered structure, basement membrane integrity, and vascular patterns; basement membrane transgression = invasion |
| Precancerous lesion grading | Dysplasia grade correlates with OCT features (irregular layering, loss of epithelial stratification) |
| Guiding biopsy site | OCT identifies the most suspicious area within a lesion to maximize diagnostic yield |
| Margin assessment | Intraoperative OCT can assess surgical margins during laryngeal microflap surgery |
| Optical biopsy | OCT combined with microlaryngoscopy significantly increases sensitivity for detecting malignancy and grading precancerous lesions compared to white-light microlaryngoscopy alone |
"In combination with microlaryngoscopy, OCT has been shown to significantly increase the sensitivity of determining benign versus malignant lesions and the grade of precancerous lesions when compared to microlaryngoscopy alone. Further studies are needed, however, to determine whether the optical biopsy derived from OCT can indeed replace an excisional tissue biopsy."
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
| Feature | Benign/Normal | Malignant |
|---|---|---|
| Epithelial thickness | Normal (<0.5 mm) | Thickened, irregular |
| Basement membrane | Sharp, continuous line | Disrupted, transgressed |
| Layered structure | Preserved (epithelium, lamina propria, muscle) | Disrupted; blurred layers |
| Rete ridges | Flat or mildly elongated | Deeply invading, angulated downward |
| Subepithelial scattering | Homogeneous | Heterogeneous, increased |
3. PARANASAL SINUSES AND NASAL CAVITY
- OCT can visualize mucociliary function - measure ciliary beat frequency and mucus transport in nasal epithelium (relevant to primary ciliary dyskinesia, cystic fibrosis, post-FESS assessment)
- Sinonasal tumors: OCT can potentially assess mucosal dysplasia depth
- Nasal polyp microstructure: Distinguish edematous stroma from invasive pathology
- Currently primarily a research tool for nasal/sinus applications; not yet standard clinical practice
4. UPPER AIRWAY / SLEEP MEDICINE
- OCT integrated into a catheter can image the pharyngeal airway cross-sectionally during sleep or sedation
- Quantify pharyngeal collapsibility in obstructive sleep apnea (OSA)
- Map the site and degree of upper airway collapse - critical for surgical planning (UPPP, tongue base surgery, hypoglossal nerve stimulation selection)
- Distinguish velopharyngeal from oropharyngeal/hypopharyngeal obstruction sites
- This is a growing research area with clinical translation potential
5. HEAD AND NECK TUMORS
- Oral cavity: OCT can detect submucosal extension of oral SCC, assess depth of invasion (a key prognostic factor)
- Oropharynx: Assess tonsillar and BOT lesion depth
- Thyroid: High-frequency OCT has been studied for thyroid nodule microstructure assessment
- Salivary glands: Experimental use for detecting salivary duct lesions and gland microstructure
Comparison: OCT vs. Other ENT Imaging Modalities
| Feature | OCT | Conventional Otoscopy | CT | MRI | Ultrasound |
|---|---|---|---|---|---|
| Resolution | µm scale | Surface only | 0.5-1 mm | 0.5-1 mm | 0.1-1 mm |
| Depth penetration | 1-3 mm | Surface | Unlimited | Unlimited | 2-10 cm |
| Real-time | Yes | Yes | No | No | Yes |
| Ionizing radiation | No | No | Yes | No | No |
| Soft tissue contrast | Excellent (micro) | Poor | Moderate | Excellent | Moderate |
| Bony detail | Limited | None | Excellent | Poor | Limited |
| Contact required | No | No | No | No | Yes |
| Portable/in-office | Yes | Yes | No | No | Yes |
| Functional/dynamic | Yes (vibrometry) | No | No | Limited | Doppler only |
| Cost | Moderate | Low | High | Very high | Moderate |
OCT vs. CT - Middle Ear (JAMA Otolaryngology 2025, PMID 40178817)
| Feature | Middle Ear OCT | CT (Temporal Bone) |
|---|---|---|
| Resolution | Higher (µm) | Lower (sub-mm) |
| Field of view | Limited - mesotympanum | Full temporal bone |
| Bony structures | Cannot image through thick bone | Excellent |
| Soft tissue detail | Superior | Limited |
| Radiation | None | Present |
| Real-time | Yes | No |
| In-office use | Yes | No |
| Role | Complementary - soft tissue pathology | Complementary - bony anatomy |
Advantages of OCT in ENT
| Advantage | Clinical Impact |
|---|---|
| Near-histological resolution | "Optical biopsy" - tissue characterization without cutting |
| Non-invasive / non-contact | Safe in all age groups; repeated use possible |
| Real-time acquisition | Intraoperative use; immediate feedback |
| No ionizing radiation | Safe for children, repeated examinations |
| Portable systems available | In-office, outpatient, bedside use |
| Functional vibrometry | Unique capability to measure ossicular mechanics in vivo |
| Visualizes behind opaque TM | Reveals hidden middle ear pathology |
| Biofilm detection | No other clinical tool can detect ME biofilms non-invasively |
Limitations of OCT in ENT
| Limitation | Detail |
|---|---|
| Limited penetration depth (1-3 mm) | Cannot image beyond superficial tissue layers; limited through thick bone |
| Cannot replace biopsy | Cannot provide definitive histopathological diagnosis |
| Limited field of view | Middle ear OCT largely confined to mesotympanum through intact TM |
| Shadowing artefacts | Bony walls and highly scattering tissues create shadows that obscure deeper structures |
| No tissue color information | Cannot assess mucosal vascular patterns as well as NBI |
| Operator expertise required | Interpretation of OCT images requires training |
| Cost and availability | Not yet widely available outside academic/research centers |
| Not yet in routine clinical guidelines | Most ENT applications remain at research/emerging clinical stage |
Current Status by ENT Region
| Application | Maturity Level |
|---|---|
| Ophthalmology (retina) | Standard of care |
| Middle ear / TM imaging | Emerging clinical - entering practice |
| OM with effusion / biofilm | Active clinical research; high promise |
| Cochlear implant guidance | Active research; prototype devices |
| Laryngeal cancer (optical biopsy) | Emerging clinical; increases diagnostic sensitivity |
| Upper airway / OSA | Research phase |
| Paranasal sinuses | Research phase |
| Head and neck tumors | Early research |
Recent Advances (2022-2025)
| Study | Finding | Reference |
|---|---|---|
| OCT-CT fusion for middle ear | OCT coregistered with CT reveals complementary soft tissue vs. bony detail in cholesteatoma and trauma; OCT superior for soft tissue, CT for bony overview | PMID 40178817 (JAMA Otolaryngol 2025) |
| Portable OCT otoscope in clinic | >100 patients imaged; TM/ME pathology revealed invisible to conventional otoscopy; fits clinical workflow | PMID 39165857 (J Biomed Opt 2024) |
| OCT vibrometry review | Demonstrates depth-resolved ossicular and cochlear vibration measurement; quantifies sound processing in individual human ears | PMID 38370517 (Semin Hear 2024) |
| OCT for OM biofilm detection | 89.6% of pediatric OM patients had TM-adherent biofilm on OCT; correlated with surgical findings | PMID 37253962 (JARO 2023) |
| OCT-guided cochlear implant sheath | Real-time fiber-optic OCT during electrode insertion detects cochlear walls; prevents intracochlear trauma; demonstrated in cadaveric cochleae | PMID 36357503 (Sci Rep 2022) |
Summary
OCT = Light-based, non-invasive, µm-resolution cross-sectional tissue imaging
Principle: Interferometry measures echo time delay of reflected near-infrared light
Top ENT applications:
1. EAR:
- TM: layers, thickness, perforation, retraction depth
- Middle ear: effusion type, biofilm, cholesteatoma soft tissue
- Cochlear implant: intraoperative real-time electrode guidance
- Vibrometry: ossicular/cochlear mechanics, sub-nm vibration measurement
2. LARYNX:
- Optical biopsy: benign vs. malignant (basement membrane integrity)
- Grades dysplasia; guides biopsy; assesses surgical margins
3. UPPER AIRWAY: pharyngeal collapse mapping in OSA (research)
4. SINUSES: ciliary function, mucosal dysplasia (research)
Key limitation: 1-3 mm depth only; cannot replace histological biopsy
Key strength: Real-time, radiation-free, near-histological, functional vibrometry
Alar collapse
alar collapse nasal valve obstruction treatment surgical
PMID: 39111772
PMID: 38992252
Alar Collapse
Definition
Relevant Anatomy
The Nasal Valves
| Valve | Location | Key Components | Normal Angle |
|---|---|---|---|
| Internal nasal valve | Junction of upper lateral cartilage (ULC) and septum | ULC, septum, anterior head of inferior turbinate | 10-15° (Caucasian); wider in non-Caucasians |
| External nasal valve | Nostril/vestibule level | LLC lateral crus, alar lobule, columella, piriform aperture, skin/soft tissue |
Pathophysiology
Bernoulli Effect and Nasal Valve Dynamics
- Negative pressure is generated in the nasal airway
- This exerts an inward force on the lateral nasal walls
- Normally, the structural rigidity of the LLC (lateral crus) resists this force
- When LLC support is insufficient, the ala is sucked inward with each breath → alar collapse
Classification
By Level of Collapse
| Type | Location | Structure Involved |
|---|---|---|
| Internal nasal valve collapse | ULC-septal junction | ULC weakness, septal deviation narrowing angle, scar adhesions |
| External nasal valve / alar collapse | Alar rim level | LLC lateral crus weakness, alar lobule laxity |
| Supra-alar collapse | Just superior to alar rim | Lateral wall insufficiency, LLC cephalic malposition |
Recent subclassification distinguishes the alar valve (LLC lateral crus region) from the rim valve (alar rim/lobule) to better guide surgical planning - Clin Exp Otorhinolaryngol 2024 (PMID 39111772)
By Mechanism (Dynamic vs. Static)
| Type | Mechanism | Example |
|---|---|---|
| Dynamic (inspiratory collapse) | Inadequate structural support against negative pressure | LLC weakness, post-rhinoplasty |
| Static obstruction | Fixed narrowing | Scar contracture, piriform aperture stenosis |
Causes
Primary (Congenital/Constitutional)
- Inherent LLC weakness - thin, floppy lateral crura that cannot resist inspiratory negative pressure
- Cephalic malposition of the LLC - an acute orientation of the LLC >35-45° off midline; the cartilage provides less lateral wall support
- Lax connective tissue (seen in aging or connective tissue disorders)
- Wide piriform aperture
Secondary (Acquired)
- Post-rhinoplasty (most common iatrogenic cause):
- Over-resection of the LLC during cephalic trim → loss of structural support
- Postoperative scar contracture at intercartilaginous or marginal incisions
- Excessive tip narrowing procedures weakening lateral crural support
- Recurvature of the lateral crura - the lateral crus curves inward rather than lying flat, paradoxically directing it toward the airway
- Trauma - fracture or disruption of the LLC
- Aging - loss of connective tissue support and skin elasticity
- Facial paralysis - loss of dilator naris muscle tone (a significant contributor)
- Previous septal surgery - destabilization of the nasal base
Clinical Features
Symptoms
- Nasal obstruction - typically unilateral or bilateral; worse with exercise/deep breathing
- Inspiratory collapse - patient or examiner can see the ala "sucking in" on deep inspiration
- Exaggerated supra-alar crease - visible groove above the alar rim
- Mouth breathing, snoring, sleep-disordered breathing
- Reduced exercise tolerance due to nasal airway limitation
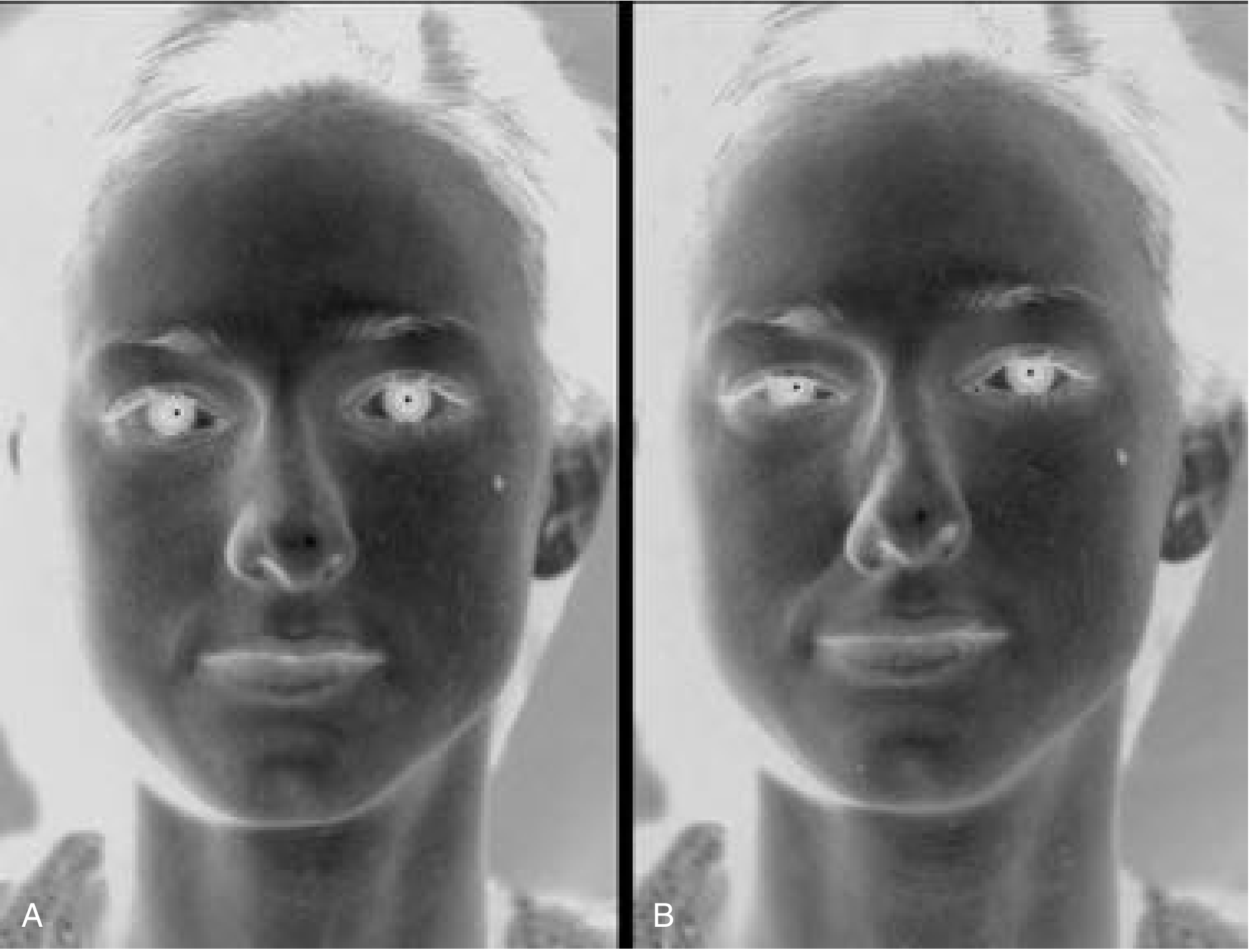
- Often associated with alar-columellar disharmony: excess columellar show (>4 mm on lateral view) and alar notching
Signs on Examination
- Visible alar collapse on deep nasal inspiration
- Exaggerated supra-alar crease
- Thin, underprojected alae
- Cephalic LLC malposition (>35-45° off midline on frontal view)
- "Parenthesis deformity" on frontal view (when combined with bulbous, cephalically oriented lateral crura)
- Alar retraction with excess columellar show (>4 mm)
- Alar notching at the apex of the alar margin
Diagnosis and Assessment
Clinical Tests
1. Modified Cottle Maneuver
- Gentle lateralization of the lateral nasal wall using a cotton-tipped applicator, cerumen curette, or similar instrument
- Specifically opens the internal nasal valve angle
- Positive result: Relief of nasal obstruction on lateralization = nasal valve compromise confirmed
- More specific than the classic Cottle maneuver (which moves too much tissue and gives many false positives)
"Gentle lateralization of the ULC with a cotton-tipped applicator, a cerumen curette, or similar instrument is a more specific maneuver to increase the internal nasal valve angle and, in those with a narrow angle, to improve airflow." - Cummings Otolaryngology
2. Breathe Right Strip Test
- Application of an external nasal dilator strip (Breathe Right) across the nasal dorsum
- If it significantly relieves obstruction → external nasal valve/lateral wall insufficiency
3. Dynamic Nasal Inspection
- Ask patient to breathe in forcefully through nose - observe alar collapse in real time
- Quantify degree of collapse (mild/moderate/severe)
4. Nasal Endoscopy
- Assess internal nasal valve angle, septal deviation, turbinate hypertrophy, and scarring
- Rule out concurrent causes of obstruction (polyps, adenoids, mass)
5. Objective Assessment (Research/Specialist)
- Rhinomanometry - measures nasal airflow resistance; documents functional impairment and surgical outcomes
- Acoustic rhinometry - maps cross-sectional area at each nasal level; identifies site of minimum cross-sectional area
- NOSE scale (Nasal Obstruction Symptom Evaluation) and SNOT-22 - validated patient-reported outcome measures
Treatment
Non-Surgical
| Option | Mechanism | Best For |
|---|---|---|
| External nasal dilator strips (Breathe Right) | Mechanical lateralization of alar wall | Mild collapse; trial before surgery; athletes; sleep |
| Nasal stents/splints | Internal support of nasal valve | Temporary; post-surgical support |
| Nasal dilators (internal clips) | Expand nasal vestibule mechanically | Mild-moderate; non-surgical candidates |
| Facial physiotherapy | Strengthen dilator naris | Facial paralysis-related collapse |
Surgical
- Cummings Otolaryngology
1. Alar Batten Grafts
- Most commonly used graft for external nasal valve/alar collapse
- Cartilage graft (usually septal or auricular conchal cartilage) placed in a precise pocket at the area of maximal lateral wall weakness
- Overlaps slightly with the lateral crus of the LLC
- Stiffens the lateral wall, preventing inspiratory collapse
- Can correct both internal and external nasal valve collapse
- Placed via marginal or intercartilaginous incision
- Works for primary and post-rhinoplasty alar collapse
2. Lateral Crural Strut Grafts (LCSGs)
- Cartilage graft sutured to the dissected undersurface of the lateral crus, extending to the dome
- Three functions:
- Flatten recurvature of the lateral crus
- Reorient the caudal margin above the cephalic margin
- Provide structural support to the lateral nasal wall
- Creates a strong, well-positioned strut of the lateral crus
- Powerful technique for recurved or malpositioned lateral crura
- Can correct alar retraction by repositioning the LLC into a pocket just below the supra-alar groove (cantilever effect that lowers the nostril margin)
3. Spreader Grafts
- Cartilage grafts placed between the nasal septum and the upper lateral cartilages
- Primary indication: Internal nasal valve stenosis/narrowing
- Also used when ULC-septal junction is narrowed, contributing to upstream obstruction
- Patients with positive cotton-tip applicator lateralization test often benefit from spreader grafts
4. LLC Repositioning (Cephalic Malposition Correction)
- When the LLC is cephalically malpositioned (>35-45° off midline):
- The LLC is detached and repositioned in a more favorable orientation
- Simultaneously improves cosmesis (reduces parenthesis deformity) and restores functional support
- Affects nasal length, projection, and rotation in addition to function
5. Alar Extension Graft
- A newer technique specifically for external nasal valve collapse
- Graft extends the lateral crus caudally to bolster the alar rim
- A 2025 prospective study (PMID 38992252, Aesthetic Plast Surg) of 51 patients showed:
- 90% subjective satisfaction with nasal breathing improvement
- Significant improvement in NOSE and SNOT-20 scores
- Rhinomanometry showed significantly increased nasal flow post-operatively
6. Composite Auricular Grafts
- Used when significant scar contracture exists at marginal/intercartilaginous incisions (common in alar retraction)
- Auricular skin-cartilage composite graft creates tension-free closure while providing structural support
7. Caudal LLC Extension Graft
- Extends the caudal margin of the lateral crus
- Addresses alar retraction and provides lateral wall support simultaneously
Surgical Approach
| Approach | Indication |
|---|---|
| Open rhinoplasty | Severe collapse, LLC repositioning, LCSG, complex revision |
| Endonasal/closed | Isolated alar batten graft, spreader grafts, mild-moderate collapse |
Graft Donor Sites (in order of preference)
| Site | Advantages | Disadvantages |
|---|---|---|
| Septal cartilage | Rigid, flat, easy to carve, no extra incision | Limited supply (especially in revision cases) |
| Auricular conchal cartilage | Plentiful, good flexibility | Curved; less rigid |
| Costal (rib) cartilage | Abundant, very rigid | Extra incision, warping risk |
Alar Collapse vs. Alar Retraction - Key Distinction
| Feature | Alar Collapse | Alar Retraction |
|---|---|---|
| Problem | Dynamic inward collapse on inspiration | Static superior displacement of alar margin |
| Cause | LLC weakness, cephalic malposition | Over-resection of LLC, scar contracture |
| Symptom | Nasal obstruction on inspiration | Excess columellar show (>4 mm), nostril show on frontal view |
| Treatment | Alar batten graft, LCSG, LLC repositioning | LCSG into caudal pocket (cantilever), composite graft, LLC repositioning |
Summary
Alar collapse = Dynamic inspiratory inward collapse of ala
due to inadequate LLC structural support
Mechanism: Bernoulli negative pressure overwhelms weakened lateral crura
Causes: Congenital LLC weakness, cephalic malposition,
post-rhinoplasty (over-resection), aging, facial paralysis, trauma
Diagnosis: Modified Cottle/cotton-tip lateralization test (most specific)
Observe dynamic collapse on forced inspiration
Rhinomanometry for objective quantification
Treatment:
- Non-surgical: External nasal dilator strips, internal splints
- Surgical:
• Alar batten graft (most common) - lateral wall support
• Lateral crural strut graft - strut + recurvature correction
• Spreader graft - internal nasal valve (upstream)
• LLC repositioning - cephalic malposition
• Alar extension graft - newer; effective (90% satisfaction)
Key principle: Restore structural rigidity to resist inspiratory
negative pressure
Bondys atticotomy
Bondy modified radical mastoidectomy atticotomy cholesteatoma
atticotomy attic cholesteatoma canal wall down mastoidectomy hearing preservation
Bondy atticotomy modified radical mastoidectomy technique indications cholesteatoma attic
https://www.theentresident.com/ent-notes-lectures/modified-r…
Bondy's Atticotomy (Bondy's Modified Radical Mastoidectomy)
Historical Background
Position in Surgical Classification
| Category | Procedures | Principle |
|---|---|---|
| Resection & Reconstruction (Canal-Wall-Up) | Simple mastoidectomy, CWU tympanomastoidectomy, cortical mastoidectomy | Cholesteatoma excised; ear canal wall preserved; middle ear reconstructed |
| Exteriorization (Canal-Wall-Down) | Radical mastoidectomy, Modified radical mastoidectomy, Bondy procedure | Anatomy altered so cholesteatoma no longer in a confined space; creates open cavity |
"Surgeries that rely on exteriorization include radical mastoidectomy, modified radical mastoidectomy, and the Bondy procedure."
- Cummings Otolaryngology Head and Neck Surgery
The Three Key Operations - Compared
| Feature | Classic Radical Mastoidectomy | Modified Radical Mastoidectomy (MRM) | Bondy's Operation |
|---|---|---|---|
| Posterior canal wall | Removed | Removed | Removed (attic + antrum only) |
| Tympanic membrane | Removed | Preserved (remnant) | Intact/preserved |
| Ossicular chain | Removed | Preserved if possible | Preserved - left untouched |
| Mesotympanum | Obliterated | Accessible; disease cleared | Left intact and sealed off |
| Eustachian tube | Obliterated | Preserved | Preserved and functional |
| Middle ear mucosa | Stripped | Preserved where possible | Preserved |
| Hearing | Abolished | Preserved or improved | Preserved (pre-existing level) |
| Scope of disease | Extensive, unresectable | Cholesteatoma involving middle ear | Attic + mastoid only; mesotympanum normal |
| Common cavity | Yes | Yes | Yes (but smaller) |
Definition of Bondy's Operation
- Exenterates the mastoid air cells, antrum, and attic (epitympanum) - removing all disease and the posterior/lateral canal wall to create an open cavity
- Preserves the mesotympanum - the tympanic membrane, ossicular chain (malleus, incus, stapes), middle ear mucosa, and Eustachian tube are left completely undisturbed
- Creates a common cavity between the mastoid, attic, and external auditory canal
- Seals the mesotympanum from the open cavity - the tympanic membrane and lateral attic wall remnant act as a barrier, preventing the open mastoid cavity from communicating with the functioning middle ear
The Critical Prerequisite
- Cholesteatoma is strictly confined to the attic, antrum, and mastoid
- The mesotympanum is normal (healthy TM, intact and functional ossicular chain, good middle ear mucosa)
- There is no cholesteatoma extension into the mesotympanum, Eustachian tube, or sinus tympani
Pathological Basis
How Attic Cholesteatoma Develops
- The pars flaccida (Shrapnell's membrane) - the upper, unsupported part of the TM - is prone to retraction due to chronic negative middle ear pressure (Eustachian tube dysfunction)
- The retraction pocket gradually invaginates medially into the attic (epitympanum)
- Accumulating desquamated keratin debris forms the cholesteatoma sac
- Disease expands laterally (eroding the scutum - the bony lateral wall of the attic), then posteriorly into the antrum and mastoid
- The mesotympanum may remain entirely uninvolved in early cases - this is the window of opportunity for Bondy's operation
- An attic or pars flaccida perforation always signifies cholesteatoma
Why Disease Confined to Attic?
- The scutum (lateral wall of epitympanum) and the necks of the malleus and incus form a partial anatomical barrier that can, in some cases, contain disease to the attic and mastoid without mesotympanic involvement
- Early or limited cholesteatoma respects these boundaries
Indications
Absolute Indication
- Attic cholesteatoma strictly limited to the epitympanum, aditus ad antrum, and mastoid, with a completely normal and intact mesotympanum
Additional Considerations
- Patients with good pre-operative hearing in whom middle ear preservation is paramount
- Where CWU (canal-wall-up) tympanomastoidectomy is technically difficult (sclerotic mastoid, limited pneumatization, low-lying tegmen)
- Patients in whom a two-stage procedure is impractical (poor compliance, geographic inaccessibility)
- Occasional or less experienced otologic surgeons for attic cholesteatoma (MRM/Bondy being technically less demanding than staged CWU)
- Only-hearing ear with attic cholesteatoma (hearing preservation of paramount importance)
Contraindications
- Cholesteatoma extending into the mesotympanum (then requires MRM or CWU)
- Cholesteatoma extending to the Eustachian tube orifice or petrous apex
- Extensive labyrinthine fistula (especially if matrix cannot be left safely)
- Medically unfit patients (general anaesthesia risk)
- Patients with limited attic disease who are reliable for follow-up (CWU or simple atticotomy with scutal reconstruction may suffice instead)
Surgical Technique
Pre-operative Setup
- General anaesthesia (with facial nerve monitoring strongly recommended)
- Patient: supine, head turned, operated ear facing upward
- Pre-operative CT temporal bone mandatory: assess extent of disease, mastoid pneumatization, integrity of tegmen and sigmoid sinus plate, semicircular canal status, facial nerve dehiscence, ossicular chain
Step-by-Step Operative Technique
- Postauricular (endaural) incision - postauricular approach gives wider access; endaural may be used for limited disease
- Elevate the skin and periosteum; expose the mastoid cortex and posterior EAC
- Drill the mastoid cortex (Macewen's triangle)
- Exenterate all mastoid air cells
- Identify the sigmoid sinus posteriorly, tegmen superiorly, and posterior semicircular canal
- Open the mastoid antrum - identify the lateral semicircular canal as the key landmark
- Follow cholesteatoma matrix forward through the aditus into the attic
- Remove the posterior and lateral bony wall of the EAC (posterior canal wall takedown)
- Remove the scutum (lateral attic wall) to expose the epitympanum
- The head of the malleus and short process of the incus (occupying the attic) are visualized
- Remove all cholesteatoma matrix from the epitympanum, around the ossicles, and from the antrum and mastoid
- The mesotympanum is NOT entered - the TM and ossicular chain below the level of the neck of the malleus are preserved and left in situ
- The area just inferior to the ossicles forms the natural boundary between the attic and mesotympanum - this is respected
- The attic, antrum, and mastoid are now a single open cavity communicating with the EAC
- The mesotympanum is sealed off by the intact TM and remaining ossicular structures
- This is the defining feature of Bondy's operation vs. full MRM
- The cavity must be smoothly contoured - no overhanging ridges, no "sump" below the floor of the EAC, no high facial ridge
- A low facial ridge is essential: the facial nerve ridge must be drilled down to the level of the fallopian canal to allow epithelialization and self-cleaning
- Round, shallow bowl configuration
- The facial (fallopian) ridge - the bony prominence overlying the facial nerve - is carefully drilled down
- A high facial ridge is the most common cause of a discharging mastoid cavity (prevents self-cleaning)
- Must be lowered to the level of the fallopian canal without injuring the facial nerve
- Mandatory - the external auditory meatus must be widened (enlarged) to allow:
- Adequate access for post-operative cavity inspection and cleaning
- Adequate ventilation of the cavity
- Self-epithelialization
- The conchal cartilage removed during meatoplasty is used to partially obliterate and reduce cavity volume
- Partial obliteration with cartilage, bone pate, or abdominal fat reduces cavity volume
- Smaller cavities are easier to maintain and have better rates of self-cleaning
- Skin flap repositioned; closure in two layers; mastoid dressing applied
Key Anatomical Landmarks
| Landmark | Significance |
|---|---|
| Scutum | Lateral bony wall of attic; eroded by cholesteatoma; removed during atticotomy |
| Lateral semicircular canal | Key landmark in mastoid; must be identified and protected |
| Tegmen plate | Roof of mastoid/middle ear; protects middle cranial fossa dura |
| Sigmoid sinus | Posterior limit of mastoidectomy |
| Fallopian canal (facial nerve) | Must be identified; facial ridge lowered to this level |
| Aditus ad antrum | Passage between mastoid antrum and attic; cholesteatoma tracks through here |
| Fossa incudis | Site of short process of incus; landmark for depth of attic dissection |
Post-operative Care and Follow-up
| Issue | Management |
|---|---|
| Cavity cleaning | Regular outpatient micro-suction every 3-6 months lifelong for most patients |
| Water precautions | Must avoid water entering the cavity (risk of infection); use cotton-wool plug/ear plug when showering; avoid swimming initially |
| Caloric vertigo | Cold water entering cavity can cause vertigo (caloric effect) - patients must be warned |
| Otorrhoea | 20-25% of cavities continue to discharge intermittently; good surgical technique reduces this |
| Recurrent cholesteatoma | Cavity must be inspected regularly; epithelial pearls may form (5-6%), usually managed in-office |
Advantages of Bondy's Operation
| Advantage |
|---|
| Hearing preserved - mesotympanum and ossicular chain left intact |
| Single-stage - no need for second-look operation (disease in open cavity is visible) |
| Lower recurrence rate than CWU (2-10% vs 5-13% for CWU) |
| Residual disease easily identified in open cavity at outpatient follow-up |
| No second-stage operation usually required |
| Technically less demanding than CWU for occasional surgeons |
Disadvantages of Bondy's Operation
| Disadvantage |
|---|
| Lifelong cavity maintenance - regular cleaning required |
| Water restrictions - cannot swim freely; must protect cavity |
| Caloric vertigo from water or temperature changes |
| Altered pinna position - meatoplasty changes external ear contour |
| Middle ear shallow if disease progresses (limits future reconstruction) |
| Hearing not improved - only preserved at pre-operative level (no ossiculoplasty) |
Comparison: Bondy vs. MRM vs. CWU
| Feature | Bondy | MRM | CWU (Canal Wall Up) |
|---|---|---|---|
| Disease extent | Attic/mastoid only | Attic + mesotympanum | Any |
| Hearing preservation | Yes (pre-op level) | Possible | Best potential |
| Recurrence rate | 2-10% | 2-10% | 5-13% residual; 5-13% recurrent |
| Second look needed | Rarely | Rarely | Often (or MRI DWI) |
| Cavity maintenance | Yes, lifelong | Yes, lifelong | No cavity |
| Water precautions | Yes | Yes | No |
| Single stage | Yes | Yes | Usually two-stage |
Results
-
A dry, self-cleaning mastoid cavity can be maintained in ~95% of cases with strict attention to technique (low facial ridge, adequate meatoplasty, well-saucerized cavity)
-
Epithelial pearls occur in 5-6% and are usually managed in-office
-
Hearing results are unchanged from pre-operative levels (preservation, not improvement)
-
Canal-wall-down procedures achieve lower recurrence (2-10%) than CWU (5-13%), with residual cholesteatoma a rarity in experienced hands
-
Shambaugh Surgery of the Ear; Scott-Brown's Otorhinolaryngology
Summary
Bondy's Atticotomy:
= Canal-wall-DOWN procedure for ATTIC-ONLY cholesteatoma
= Mastoid + attic + antrum exteriorized → open cavity
= Mesotympanum, TM, ossicles, Eustachian tube LEFT INTACT
= Hearing PRESERVED at pre-operative level (not improved)
= Single-stage; no second-look required
= Lifelong cavity cleaning + water precautions needed
Key requirement: Cholesteatoma MUST be confined to attic/mastoid
Mesotympanum must be normal
Key steps:
1. Postauricular approach
2. Mastoidectomy → open antrum
3. Atticotomy → remove scutum, remove lateral canal wall
4. Eradicate ALL disease (attic, antrum, mastoid)
5. Preserve mesotympanum (do not enter it)
6. Low facial ridge + smooth saucerization
7. Meatoplasty (mandatory)
Thornwaldt cyst
Tornwaldt cyst nasopharynx diagnosis treatment MRI
Tornwaldt cyst nasopharynx
PMID: 38784350
PMID: 40677866
Thornwaldt Tornwaldt cyst nasopharynx embryology pathology MRI features treatment 2023 2024
PMID: 31091377
PMID: 31760788
https://drsanu.com/articles/tornwaldt-cyst
Thornwaldt (Tornwaldt) Cyst
Nomenclature
- Pharyngeal bursa cyst (Bursa pharyngea)
- Luschka's bursa cyst
- Nasopharyngeal bursa cyst
Definition
Embryology and Pathogenesis
Normal Embryology
- During early embryogenesis, the notochord (axial mesodermal structure that becomes the nucleus pulposus of intervertebral discs) makes transient contact with the endoderm of the pharyngeal roof
- This contact point is the pharyngeal bursa (Bursa pharyngea of Luschka) - a small pit or invagination in the roof of the nasopharynx, located in the midline between the longus capitis muscles
- Normally, this communication regresses completely by birth
Cyst Formation
- If this connection fails to regress, a residual pit or recess persists (the pharyngeal bursa)
- The opening of this bursa may become obstructed due to:
- Infection
- Adenoid hypertrophy
- Trauma or surgery
- Inflammatory scarring
- Obstruction traps secretions from the respiratory epithelial lining → progressive accumulation → cyst formation
- The cyst is lined by respiratory epithelium (pseudostratified ciliated columnar) and accumulates fluid with variable proteinaceous content
- Secondary infection causes inflammation and may change the cyst contents
Classification by Drainage
| Type | Description |
|---|---|
| Cystic type | Obstructed drainage → true cyst formation; more likely to be symptomatic |
| Crusting type | Drains spontaneously into nasopharynx; forms crusts; less likely to enlarge |
Epidemiology
| Parameter | Data |
|---|---|
| Incidence | 1.4-3.3% of the general population (imaging-based series) |
| Age of presentation | Typically 15-30 years (can occur at any age) |
| Sex | No significant gender predilection |
| Presentation | Majority asymptomatic - incidentally discovered on MRI done for other reasons |
| Symptomatic rate | Minority - usually larger or infected cysts (>1-2 cm) |
Anatomy and Location
- Exact location: Posterior nasopharyngeal wall, strictly in the midline, between the two longus capitis muscles
- Sits in the roof (vault) of the nasopharynx, immediately superior to the pharyngeal tonsil (adenoid) region
- Lies immediately deep to the pharyngeal mucosa (submucosal)
- May be slightly off-midline in some cases
- Surrounded by the prevertebral muscles laterally
- Superior relation: basisphenoid and basiocciput (clivus)
- Posterior relation: anterior arch of atlas (C1)
Clinical Features
Asymptomatic (Majority)
- Most cysts are small (2-10 mm) and completely asymptomatic
- Discovered incidentally on MRI obtained for headache, sleep apnea evaluation, or other conditions
- Represent the majority of cases in imaging series
Symptomatic ("Tornwaldt's Disease")
| Symptom | Mechanism |
|---|---|
| Postnasal drip (most common symptomatic complaint) | Mucoid secretions draining from cyst into nasopharynx |
| Nasal obstruction | Mass effect on nasopharyngeal airway |
| Halitosis (foul breath) | Stagnant, infected cyst contents |
| Occipital/nuchal headache | Irritation of prevertebral muscles and upper cervical nerves |
| Neck stiffness | Involvement of longus capitis and prevertebral musculature |
| Pharyngitis / nasopharyngeal discomfort | Mucosal irritation |
| Eustachian tube dysfunction | Large cyst obstructing Eustachian tube orifice |
| Otitis media with effusion (OME) | Secondary to Eustachian tube obstruction; conductive hearing loss |
| Nasal airway complete obstruction | Rare - huge cysts (reported in literature, PMID 31760788) |
| Auditory symptoms | As an incidental finding during OSA workup in a patient with auditory symptoms (PMID 40677866) |
"Symptomatic cysts may cause nasal obstruction, postnasal drip, halitosis, occipital headache, or Eustachian tube dysfunction."
- PMID 40677866 (Radiol Case Rep 2025)
"Smaller cysts are usually asymptomatic; cysts exceeding a diameter of 1 to 2 cm may be symptomatic."
- PMID 31760788 (Ear Nose Throat J)
Diagnosis
1. Nasal Endoscopy
- First-line investigation when clinical suspicion exists
- Reveals a smooth, submucosal, well-encapsulated midline mass on the roof/posterior wall of the nasopharynx
- Surface covered by intact normal nasopharyngeal mucosa (unless infected/ulcerated)
- The pharyngeal orifice of the bursa may be visible as a small pit, but is often difficult to see even when unobstructed
- Cannot assess depth, intracranial extension, or cyst content
2. MRI - Gold Standard Imaging
| Sequence | Typical Appearance | Explanation |
|---|---|---|
| T1-weighted | Intermediate to high signal | Proteinaceous fluid content; may be variable |
| T2-weighted | High signal (bright) | Simple fluid; most cysts are hyperintense |
| T1 post-gadolinium | No enhancement (wall may show thin rim) | Benign cyst - no solid enhancing component |
| Location | Midline, posterior nasopharyngeal wall, between longus capitis muscles | Pathognomonic location |
| Morphology | Well-circumscribed, round/oval, thin-walled | Typical benign cyst appearance |
- Better soft tissue characterization (confirms cystic nature vs. solid mass)
- Can detect intracranial extension
- Differentiates from other nasopharyngeal pathology
- No radiation
- Low-attenuation (hypodense) soft tissue mass on the posterior nasopharyngeal wall
- Sharply defined margins
- No bony erosion or surrounding soft tissue reaction
- Helpful in differentiating from bony lesions
3. Histopathology
- Confirms diagnosis after surgical removal
- Cyst wall lined by respiratory epithelium (pseudostratified ciliated columnar) ± squamous metaplastic areas
- Variable content: clear/mucoid/proteinaceous fluid
- Inflammatory infiltrate if secondarily infected
- No malignant features
Differential Diagnosis
| Differential | Distinguishing Features |
|---|---|
| Adenoid hypertrophy | Solid soft tissue, not cystic; enhances on MRI; in children |
| Mucous retention cyst | Usually off-midline, lateral nasopharyngeal wall; not between longus capitis muscles |
| Nasopharyngeal carcinoma (NPC) | Solid, irregular, enhancing mass; lateral wall involvement; cervical lymphadenopathy; NOT between longus capitis |
| Neurenteric cyst | Similar location; may have connection to spinal canal; bony defect on CT |
| Meningocele / encephalocele | Critical differential before surgery - connection to intracranial contents; CSF on MRI; DO NOT excise without excluding this first |
| Minor salivary gland tumor | Solid or mixed; may enhance |
| Rathke's cleft cyst | Sellar/suprasellar; different location |
| Chordoma | Bony destruction of clivus; solid enhancing mass |
| Branchial cleft cyst | Lateral neck; may extend to nasopharynx but typically not midline posterior wall |
CRITICAL: Thornwaldt cysts must be differentiated from nasopharyngeal encephaloceles before any surgical excision. Inadvertent excision of an encephalocele can cause catastrophic CSF leak and meningitis.
Treatment
Asymptomatic Cysts
- No treatment required - conservative management with clinical observation
- Annual or biannual endoscopic follow-up if large
- Reassure patient of benign nature
Symptomatic Cysts - Surgical Options
1. Endoscopic Transnasal Marsupialization (Preferred)
- Treatment of choice for symptomatic Thornwaldt cysts
- Performed under general anaesthesia with a rigid nasal endoscope
- The cyst is opened widely (unroofed/marsupialised) so its contents drain freely into the nasopharynx
- The posterior wall of the cyst is excised, creating a wide opening
- Allows drainage and prevents re-accumulation
- Excellent outcomes - complete symptom resolution in the vast majority
- Low recurrence rate
- Successful treatment confirmed in both recent case series (PMID 38784350, Cureus 2024)
2. Complete Surgical Excision
- Complete cyst removal with its wall
- More technically demanding; risk of damage to prevertebral musculature
- Performed when marsupialization is insufficient or recurrence occurs
- Transnasal endoscopic approach
3. Aspiration/Drainage Alone
- Generally not recommended - high recurrence rate as the cyst wall remains intact
Post-operative
- Symptom resolution usually complete
- Low recurrence rate with adequate marsupialization
- Follow-up endoscopy at 3-6 months
Key Clinical Points
| Point | Detail |
|---|---|
| Most important feature | Strictly midline, posterior nasopharyngeal wall, between longus capitis muscles |
| Most common presentation | Incidental MRI finding |
| Hallmark MRI | T1 intermediate/high, T2 high signal, no enhancement, midline |
| Most dangerous differential | Encephalocele - must be excluded before surgery |
| Treatment of choice | Endoscopic transnasal marsupialization |
| Symptomatic size threshold | Usually >1-2 cm |
| Incidence | 1.4-3.3% of population |
| Complication if missed | Eustachian tube dysfunction → otitis media with effusion |
Summary Table
| Feature | Thornwaldt Cyst |
|---|---|
| Origin | Persistent notochord-pharyngeal connection (pharyngeal bursa) |
| Location | Midline, posterior nasopharyngeal wall, between longus capitis muscles |
| Lining | Respiratory epithelium (pseudostratified ciliated columnar) |
| Content | Serous/mucoid/proteinaceous fluid |
| Epidemiology | 1.4-3.3%; no sex predilection; ages 15-30 common |
| Presentation | Usually asymptomatic (incidental MRI); symptomatic if infected/large |
| Symptoms | Postnasal drip, nasal obstruction, halitosis, occipital headache, OME |
| MRI | T1 intermediate/high, T2 bright, no gadolinium enhancement |
| Treatment | Observation (asymptomatic); endoscopic marsupialization (symptomatic) |
| Prognosis | Excellent; very low recurrence after adequate surgery |
| Critical DDx | Encephalocele (exclude before surgery); NPC |
Undifferentiated sinonasal ma
Undifferentiated sinonasal malignancy
sinonasal undifferentiated carcinoma SNUC treatment outcomes
PMID: 39162231
PMID: 37859617
PMID: 34958321
Sinonasal Undifferentiated Carcinoma (SNUC)
Definition
"SNUCs are rare tumors arising from Schneiderian epithelium and were only recognized as a distinct entity in 1986 [by Frierson et al.]"
- Cummings Otolaryngology Head and Neck Surgery
Historical Context
- First formally described as a distinct entity by Frierson et al. in 1986
- Also known as anaplastic carcinoma of the sinonasal tract
- Before 1986, many of these tumors were misclassified as olfactory neuroblastoma (ONB/esthesioneuroblastoma), lymphoma, or poorly differentiated squamous cell carcinoma
- Recent molecular/genomic studies (post-2015) have further subdivided the SNUC category into distinct molecular entities with different biology, prognosis, and treatment implications
Epidemiology
| Parameter | Data |
|---|---|
| Incidence | Extremely rare; accounts for <1% of all head and neck malignancies |
| Age | Most commonly 5th-7th decade; rare pediatric cases reported |
| Sex | Male predominance (M:F ~2:1) |
| Ethnicity | No clear predilection |
| Stage at presentation | ~80% present at T4 (advanced, locally extensive disease) |
Molecular Subtypes - The Modern Classification
"Several additional tumor types with distinct pathologic and genomic features have been identified, including IDH2-mutant SNUCs, INI-1-deficient sinonasal carcinomas, and NUT-midline carcinomas."
- Cummings Otolaryngology
| Subtype | Molecular Feature | Clinical Notes |
|---|---|---|
| Classic SNUC | No specific driver mutation | Aggressive; poor prognosis |
| IDH2-mutant SNUC | IDH2 R172 point mutation | Distinct entity; may overlap with olfactory carcinoma; potentially targetable with IDH2 inhibitors (enasidenib) |
| SMARCB1 (INI-1)-deficient sinonasal carcinoma | Loss of SMARCB1/INI-1 expression | Highly aggressive; EZH2 inhibition being explored |
| NUT carcinoma (NUT midline carcinoma) | NUTM1 gene rearrangement (t(15;19)) | Extremely aggressive; occurs in midline structures; BET bromodomain inhibitors under investigation |
| SMARCA4-deficient undifferentiated tumor | Loss of SMARCA4 (BRG1) | Newly characterized; very poor prognosis |
Molecular subtyping is now mandatory in pathological workup, as it has treatment and prognostic implications, and because clinical series that predate molecular classification may have mixed multiple distinct entities.
Pathology
Gross Appearance
- Large, bulky, polypoid or infiltrative mass
- Often fills the nasal cavity/sinus and extends beyond
- Areas of necrosis and hemorrhage common
- Paradoxically, often produces few symptoms despite extensive nature - patients may ignore early symptoms
Histology
- Sheets, nests, trabeculae, or ribbons of undifferentiated cells
- Small to medium-sized cells with high nuclear:cytoplasmic ratio
- Prominent nucleoli
- Abundant mitoses and geographic necrosis (characteristic feature)
- No squamous differentiation (no keratin pearls, intercellular bridges)
- No glandular differentiation (no mucin, no acinar structures)
- No neuroendocrine differentiation by light microscopy (though focal IHC staining may be present)
- Vascular and perineural invasion common
Immunohistochemistry (IHC) - Critical for Diagnosis
| Marker | SNUC Result | Significance |
|---|---|---|
| Pan-cytokeratin (AE1/AE3, CK7) | Positive | Confirms epithelial origin |
| p63 / p40 | Negative | Distinguishes from SCC |
| Synaptophysin, chromogranin, CD56 | Negative or focal | Distinguishes from neuroendocrine carcinoma |
| S100, HMB-45 | Negative | Distinguishes from melanoma |
| CD45 (LCA) | Negative | Distinguishes from lymphoma |
| EBV (EBER in situ hybridization) | Negative | Distinguishes from WHO Type 3 NPC (undifferentiated carcinoma) |
| IDH2 R172 | Positive (in IDH2 subtype) | Molecular subtyping |
| INI-1 (SMARCB1) | Lost (in INI-1-deficient type) | Molecular subtyping |
| NUT (C15orf55) | Positive (in NUT carcinoma) | Molecular subtyping |
Key distinguishing feature: SNUC is typically EBV-negative, which separates it from undifferentiated nasopharyngeal carcinoma (WHO Type 3/lymphoepithelioma) - one of the most important and clinically critical distinctions.
Clinical Features
Symptoms
| Symptom | Frequency/Notes |
|---|---|
| Nasal obstruction | Most common presenting symptom |
| Epistaxis | Unilateral, recurrent; often first noticed symptom |
| Facial pain / facial swelling | Orbital and maxillary extension |
| Proptosis / diplopia | Orbital invasion (common at presentation) |
| Epiphora | Nasolacrimal duct obstruction |
| Cranial nerve deficits | Skull base invasion (CN II, III, IV, V, VI) |
| Trismus | Pterygoid / infratemporal fossa extension |
| Cervical lymphadenopathy | N1-N2 disease at presentation in ~20-30% |
| Anosmia | Cribriform plate involvement |
| Headache | Intracranial extension |
"It is a highly aggressive and invasive tumour commonly containing areas of necrosis but, paradoxically, often produces few symptoms despite its extensive nature."
- Scott-Brown's Otorhinolaryngology
Sites of Origin
- Nasal cavity (most common primary site)
- Ethmoid sinuses
- Maxillary sinus
- May involve multiple compartments simultaneously at diagnosis
- Skull base, cribriform plate, orbit, and anterior cranial fossa involvement common at presentation
Differential Diagnosis
| Tumor | Key Distinguishing Feature |
|---|---|
| Olfactory neuroblastoma (ONB) | Positive synaptophysin/chromogranin; Homer-Wright pseudorosettes; Hyam's grading; S100+ sustentacular cells; EBV- |
| Sinonasal neuroendocrine carcinoma (SNEC) | Prominent neuroendocrine IHC (synaptophysin, chromogranin, CD56 diffuse+) |
| Undifferentiated NPC (WHO Type 3) | EBV-positive (EBER+); nasopharyngeal origin; lymphocytic stroma |
| High-grade sinonasal adenocarcinoma | Glandular IHC markers (CK20, CDX2 for ITAC) |
| Mucosal melanoma | S100+, HMB-45+, Melan-A+; may be amelanotic |
| Lymphoma (NK/T-cell, DLBCL) | CD45+; T/B-cell markers positive; angiocentric |
| Rhabdomyosarcoma | Desmin+, myogenin+; younger patients |
| NUT carcinoma | NUT IHC positive; NUTM1 FISH; distinct entity within undifferentiated tumors |
| SMARCB1-deficient carcinoma | Loss of INI-1 by IHC; distinct behavior |
| Poorly differentiated SCC | p63/p40 positive; focal keratinization |
Staging
| Stage | T Category | Description |
|---|---|---|
| T1 | Tumor limited to one subsite of a single region with or without bony invasion | |
| T2 | Two subsites of a single region or extends to involve an adjacent region within the nasoethmoidal complex | |
| T3 | Extends to invade medial wall/floor of orbit, maxillary sinus, palate, or cribriform plate | |
| T4a | Invades anterior orbital contents, skin of nose/cheek, minimal pterygoid plates, hard palate, frontal or sphenoid sinus | |
| T4b | Invades orbital apex, dura, brain, middle cranial fossa, CN except V2, nasopharynx, or clivus |
80% of SNUCs are T4 at presentation - the most locally advanced stage. This is the fundamental driver of its poor prognosis.
Investigations
Imaging
| Modality | Role |
|---|---|
| MRI with gadolinium | Gold standard for soft tissue extent, intracranial/orbital involvement, perineural spread, dural and brain invasion |
| CT sinuses | Bony destruction, extent of sinonasal involvement, surgical planning |
| PET-CT | Systemic staging, lymph node involvement, distant metastases |
Tissue Diagnosis
- Biopsy (endoscopic or open) - essential
- Full IHC panel including cytokeratins, neuroendocrine markers, S100, p40/p63, EBV, NUT, INI-1
- Molecular testing: IDH2, SMARCB1, NUTM1 FISH
Treatment
Principles
- Multimodality treatment is essential - single-modality treatment is strongly associated with worse survival
- Treatment must be individualized based on resectability, stage, molecular subtype, and patient fitness
Treatment Modalities
Surgery
- Radical surgical resection (craniofacial resection/anterior skull base surgery) when feasible
- Endoscopic skull base surgery increasingly used for selected cases
- Aims for R0 (clear margins) resection
- Combined open and endoscopic approaches for extensive disease
- 5-year local control of 74% with gross total resection vs. only 24% with subtotal resection (UCSF series)
- Elective or therapeutic neck dissection - considered given high regional failure rate (27% at 2 years)
Radiation Therapy
- IMRT (Intensity-Modulated Radiotherapy) is standard adjuvant/definitive modality
- Doses typically 60-70 Gy to primary site
- Particle therapy (proton beam, carbon ion) increasingly used for skull base proximity - better dose distribution, sparing of critical neural structures
- Elective nodal irradiation recommended given risk of regional recurrence
Chemotherapy
- Platinum-based regimens (cisplatin + 5-FU, or cisplatin + paclitaxel) are most commonly used
- Two roles:
- Induction (neoadjuvant) chemotherapy - given before surgery/RT to downstage tumor and test chemo-sensitivity
- Concurrent chemotherapy with radiation (chemoRT) - radiosensitization
Emerging Role of Induction Chemotherapy
Induction chemotherapy (IC) has recently gained major importance in SNUC management.
- 5-year OS with IC: 72.6% vs. 44.5% without IC
- "IC should be considered in every patient diagnosed with SNUC"
- Tests tumor chemo-sensitivity (good responders are selected for further aggressive local treatment)
- Potential to downstage unresectable disease to resectable
- Treats occult micrometastatic disease early
- Avoids unnecessary radical surgery in chemoresistant (poor prognosis) tumors
Evidence-Based Treatment Strategies
| Approach | Evidence | Outcomes |
|---|---|---|
| Trimodality (Surgery + RT + Chemo) | Meta-analysis by Morand et al. (390 pts) | Single-modality = 3x increased risk of death vs. dual or triple therapy (HR 2.97 vs. 2.80) |
| Induction chemo → CRT (non-surgical) | Rischin et al. (10 pts) | 2-year OS 64% |
| Surgery + adjuvant CRT | MD Anderson series (18 pts) | 5-year OS 64.2% |
| Chemoradiotherapy alone (definitive) | Meta-analysis (PMID 37859617) | Highest cumulative survival (42% at 40 months); comparable to trimodality |
| Surgery alone or RT alone | Multiple series | 5-year OS ~0-22%; should not be used alone |
Key caveat: Direct comparisons are confounded by selection bias - unresectable tumors are treated with non-operative approaches, artificially worsening those outcomes.
Treatment Algorithm (General)
SNUC Diagnosis
↓
Molecular subtyping (IDH2, INI-1, NUT, SMARCA4)
↓
Staging (CT + MRI + PET-CT)
↓
Multidisciplinary tumor board
↓
Resectable disease: Unresectable / borderline disease:
↓ ↓
Induction chemotherapy Induction chemotherapy
(cisplatin-based) (cisplatin-based)
↓ ↓
Responders → Surgery + Good response → consider
adjuvant IMRT ± chemo surgery or definitive CRT
↓
Non-responders → Definitive CRT
Molecular-Targeted Therapy (Emerging)
- IDH2-mutant SNUC: Enasidenib (IDH2 inhibitor) - case reports of response
- NUT carcinoma: BET bromodomain inhibitors (e.g., OTX015) - under investigation
- SMARCB1-deficient: EZH2 inhibitors (tazemetostat) - under investigation
- Immune checkpoint inhibitors - role being explored given tumor microenvironment data
Prognosis
| Parameter | Data |
|---|---|
| Overall 5-year OS (untreated/single modality) | 0-22% |
| 5-year OS (multimodality, surgery + RT) | ~40-65% |
| 5-year OS with induction chemotherapy | ~72.6% (PMID 39162231) |
| Cumulative OS at 95 months (all comers) | ~30% (PMID 37859617) |
| Regional failure rate | ~27% at 2 years |
| Distant metastasis rate | Significant; liver, lung, bone |
- T stage (T4b worst)
- Extent of surgical resection (R0 vs R1/R2)
- Chemotherapy response (induction chemo responders do significantly better)
- Molecular subtype (IDH2-mutant may behave differently)
- Intracranial extension
Comparison with Related Entities
| Feature | SNUC | Olfactory Neuroblastoma (ONB) | Undifferentiated NPC |
|---|---|---|---|
| EBV | Negative | Negative | Positive |
| Neuroendocrine markers | Negative/focal | Positive | Negative |
| p63/p40 | Negative | Negative | Negative |
| Lymphocytic stroma | No | No | Yes |
| Origin | Schneiderian epithelium | Olfactory neuroepithelium | Nasopharyngeal epithelium |
| Cribriform plate | Often involved | Classic origin site | Uncommon |
| Prognosis | Very poor | Moderate (Kadish-dependent) | Better (EBV-related, chemo-sensitive) |
| Treatment | Multimodality | Surgery + RT ± chemo | Chemoradiation (excellent response) |
Summary
SNUC - Key Facts:
• Rare, aggressive, high-grade carcinoma; Schneiderian epithelium origin
• First described 1986; now subdivided by molecular markers
(IDH2, INI-1/SMARCB1, NUT, SMARCA4)
• 80% present at T4; often paradoxically few symptoms despite large mass
• EBV-NEGATIVE (key feature distinguishing from undifferentiated NPC)
• Diagnosis of exclusion after ruling out SCC, NEC, melanoma, lymphoma, ONB
Treatment:
• NEVER single-modality
• Induction chemotherapy → dramatically improves OS (72.6% vs 44.5%)
• Surgery + adjuvant IMRT = best local control (74% if gross total resection)
• Definitive CRT for unresectable disease
• Elective neck treatment mandatory (27% regional failure at 2 years)
• Particle therapy (proton/carbon) for skull base proximity
Prognosis:
• 5-year OS ~40-65% with optimal multimodality treatment
• Significantly better with induction chemotherapy
• Distant metastases and locoregional recurrence are principal failure modes
Cernea classification
Cernea classification external branch superior laryngeal nerve thyroid surgery
PMID: 38075061
Cernea classification EBSLN external branch superior laryngeal nerve types 1 2a 2b anatomy thyroid surgery
PMID: 33521945
Cernea 1992 original classification EBSLN superior laryngeal nerve thyroid superior pole vessels cricothyroid muscle palsy voice
Cernea Classification of the External Branch of the Superior Laryngeal Nerve (EBSLN)
Background
"In 1992, we proposed the following surgical anatomic classification of the EBSLN, based on the relationships among the nerve, the superior thyroid vessels, and the upper border of the superior thyroid pole."
- Cernea et al. (original description, via Entokey)
"The course of the external branch is variable and meticulous dissection close to the superior pole is necessary to prevent iatrogenic injury during thyroidectomy."
- Mulholland and Greenfield's Surgery: Scientific Principles and Practice, 7e
Anatomy Relevant to the Classification
The Superior Laryngeal Nerve (SLN)
- Arises from the inferior ganglion of the vagus nerve (CN X)
- Divides into two branches at the level of the hyoid bone:
- Internal branch (IBSLN): Sensory to the supraglottis and laryngeal mucosa above the vocal cords; enters the larynx through the thyrohyoid membrane
- External branch (EBSLN): Motor to the cricothyroid muscle (CTM); the branch classified by Cernea
The EBSLN
- Descends along the inferior pharyngeal constrictor muscle
- Runs in close proximity to the superior thyroid artery (STA) and superior thyroid vein (STV)
- Enters the cricothyroid muscle from its posteromedial surface
- The cricothyroid muscle is the only intrinsic laryngeal muscle innervated outside the larynx
- CTM function: tenses and elongates the vocal cord → raises vocal pitch, increases vocal projection and fundamental frequency
Why It Matters Surgically
- Cricothyroid muscle paralysis
- Loss of ability to produce high-pitched tones
- Lowered fundamental voice frequency
- Reduced vocal projection and endurance
- Vocal fatigue, especially during prolonged speaking or singing
- Often missed on routine laryngoscopy (cords look normal; only acoustic analysis or EMG detects the deficit)
- Particularly devastating for professional singers, teachers, lawyers, public speakers
The Cernea Classification
Type 1 (Safe Zone)
| Feature | Detail |
|---|---|
| Level | Crosses vessels high in the neck, well above the thyroid pole |
| Risk of injury | LOW - nerve is remote from the surgical dissection field |
| Frequency (small goiter) | ~60-68% |
| Frequency (large goiter) | ~23% |
| Frequency (prospective IONM series) | ~41% |
The nerve crosses safely above the level where the superior pole vessels are ligated. With careful high-vessel ligation at the thyroid capsule (hugging technique), injury is unlikely.
Type 2a (Intermediate Risk)
| Feature | Detail |
|---|---|
| Level | Crosses close to the superior pole, but still above it |
| Risk of injury | MODERATE - within the dissection zone; care required |
| Frequency (small goiter) | ~11-17% |
| Frequency (large goiter) | ~15% |
| Frequency (prospective IONM series) | ~41-46% |
The nerve is close enough to be inadvertently clamped or ligated with the superior thyroid vessels if mass ligation is performed. Individual vessel ligation at the thyroid capsule reduces (but does not eliminate) risk.
Type 2b (Highest Risk)
| Feature | Detail |
|---|---|
| Level | Nerve passes BEHIND or BELOW the superior thyroid vessels, deep to the upper pole |
| Risk of injury | HIGHEST - nerve is within or posterior to the dissection plane |
| Frequency (small goiter) | ~14-20% |
| Frequency (large goiter) | ~54% (significantly more common in large goiters) |
| Frequency (prospective IONM series) | ~11% |
The nerve is essentially hidden behind the superior pole, easily mistaken for a vascular structure, and at maximal risk during routine superior pole dissection and vessel ligation. A large goiter dramatically increases the likelihood of this configuration.
Type NI (Non-Identifiable)
- The nerve runs so deeply or under the pharyngeal constrictor that it cannot be visualized
- Some authors consider this a separate category; others fold it into Type 2b or attribute it to the Type 4 of the Kierner classification (nerve running dorsally)
Summary Table
| Type | Relationship to Superior Pole Plane | Risk | Frequency (Small Goiter) | Frequency (Large Goiter) |
|---|---|---|---|---|
| 1 | Crosses STV ≥1 cm ABOVE superior pole | Low | 60-68% | 23% |
| 2a | Crosses STV <1 cm ABOVE superior pole | Moderate | 11-17% | 15% |
| 2b | Crosses STV BELOW superior pole | Highest | 14-20% | 54% |
| NI | Non-identifiable | High | ~3% | Variable |
Key insight: Large goiter shifts the classification distribution dramatically toward Type 2b (54% in large goiters vs. 14-20% in small goiters), because the enlarged gland physically displaces the EBSLN downward and medially relative to the superior pole vessels.
Comparison with Other Classifications
Kierner Classification (1998)
| Type | Criteria |
|---|---|
| 1 | Crosses STV >1 cm above upper pole (=Cernea 1) |
| 2 | Crosses STV <1 cm above upper pole (=Cernea 2a) |
| 3 | Crosses STV below upper pole (=Cernea 2b) |
| 4 | Descends dorsally to artery and crosses STA branches immediately above upper pole (=Cernea NI - explains the non-identifiable variant) |
Friedman Classification
| Type | Criteria | Significance |
|---|---|---|
| 1 | Runs superficial to the inferior constrictor (~20%) | Easily identifiable, low risk |
| 2 | Penetrates the inferior constrictor in its lower portion (~67%) | Partially buried, moderate risk |
| 3 | Runs entirely deep to the inferior constrictor ("buried nerve") (~13%) | Invisible without dissection, highest risk |
A 2023 prospective study (PMID 38075061) found the Friedman classification has higher accuracy (69.8% vs 44.3%) for predicting EBSLN injury risk than Cernea, though with a higher false-negative rate. All three classifications (Cernea 2a/2b, Kierner 2/3/4, Friedman 2) identify the same high-risk anatomical configurations.
Surgical Implications
The "Hugging" or "Capsular Dissection" Technique
- Ligate the superior thyroid vessels individually at the thyroid capsule rather than en masse high in the neck
- Minimizes the zone of dissection near the EBSLN regardless of its classification type
- Considered the single most important technical maneuver to protect the EBSLN
Identification Strategy Based on Classification
| Risk Level | Approach |
|---|---|
| Type 1 (low risk) | Careful capsular vessel ligation; nerve identification not always mandatory |
| Types 2a/2b (high risk) | Active identification of EBSLN recommended before vessel ligation |
| Large goiter (high risk for 2b) | Always attempt EBSLN identification |
| All types | Intraoperative neuromonitoring (IONM) with CTM electrodes increasingly recommended |
Intraoperative Neuromonitoring (IONM) for EBSLN
- EBSLN signal attenuation >50% after superior pole dissection correlates with significantly worse voice outcomes (PMID 33521945, Laryngoscope 2021)
- CTM needle electrodes provide finer amplitude measurement than standard ETT electrodes for detecting subtle EBSLN injury
- Cricothyroid muscle twitch on stimulation is visible in ~92.5% of cases; EMG signal obtained in ~54%
Clinical Consequences of EBSLN Injury
| Feature | Detail |
|---|---|
| Mechanism | Cricothyroid muscle denervation |
| CTM function lost | Vocal cord tension/elongation for high-pitch |
| Laryngoscopy appearance | Often NORMAL (cords adduct normally - RLN intact) |
| Symptoms | Lowered fundamental frequency, loss of high notes, vocal fatigue, reduced projection |
| Detection | Acoustic voice analysis, videostroboscopy (reduced mucosal wave), LEMG |
| Incidence | Up to 58% in some series; most cases subclinical; ~1-2% clinically significant |
| High-risk patients | Professional singers, teachers, public speakers, voice performers |
Key Points Summary
Cernea Classification - EBSLN (1992)
Type 1: Crosses STV ≥1 cm ABOVE superior pole → LOW risk (~60% small goiter)
Type 2a: Crosses STV <1 cm ABOVE superior pole → MODERATE risk (~17%)
Type 2b: Crosses STV BELOW superior pole → HIGHEST risk (~20% small, ~54% large goiter)
NI: Non-identifiable → ~3%
The "2" types (2a + 2b) are HIGH-RISK requiring active nerve identification
Large goiter → dramatically shifts distribution to Type 2b (54%)
Surgical principle: Individual capsular vessel ligation (hugging technique)
± IONM to detect subtle injury
Active identification mandatory in Types 2a/2b and large goiters
EBSLN injury → cricothyroid palsy → loss of high pitch, vocal fatigue
→ Often MISSED on routine laryngoscopy
Ebstein Barr virus and its implications in ENT
Epstein-Barr virus ENT head neck nasopharyngeal carcinoma lymphoma
Epstein-Barr virus nasopharyngeal carcinoma pathogenesis treatment
PMID: 39505801
Epstein Barr virus ENT implications infectious mononucleosis NPC lymphoma Burkitt sinonasal 2024
PMID: 38254110
EBV infectious mononucleosis complications airway tonsil treatment
EBV infectious mononucleosis ENT complications airway obstruction corticosteroids tonsillectomy indications peritonsillar abscess
Epstein-Barr Virus (EBV) and Its Implications in ENT
The Virus - Overview
Key Virological Features
| Feature | Detail |
|---|---|
| Classification | dsDNA virus; Gammaherpesvirinae; HHV-4 |
| Size | ~172 kb genome; enveloped icosahedral capsid |
| Primary target cells | B lymphocytes (via CD21/CR2 = complement receptor = EBV receptor) |
| Secondary target | Nasopharyngeal and oropharyngeal epithelium |
| Seroprevalence | >90% of adults worldwide are EBV-seropositive |
| Transmission | Saliva (hence "the kissing disease"); also blood transfusion, organ transplant |
| Latency | Establishes lifelong latency in B lymphocytes; intermittent reactivation |
Lifecycle Phases
- Primary infection - EBV enters via oropharyngeal epithelium, replicates, then infects B lymphocytes via CD21
- B-cell immortalization - EBV drives polyclonal B-cell proliferation via latent gene expression (LMP1, LMP2, EBNAs)
- Immune control - massive CTL (CD8+) response → atypical lymphocytes → controls acute infection
- Latency - virus persists in resting memory B cells with minimal gene expression
- Reactivation - during immunosuppression, stress; lytic replication resumes
EBV Latency Programs
| Latency Program | Genes Expressed | Associated Disease |
|---|---|---|
| Latency 0 | None (resting memory B cell) | Healthy latent carrier |
| Latency I | EBNA1 only | Burkitt lymphoma |
| Latency II | EBNA1, LMP1, LMP2 | NPC, Hodgkin lymphoma |
| Latency III | All EBNAs + LMPs | Post-transplant lymphoproliferative disorder (PTLD), immunoblastic lymphoma |
EBV in ENT - Organ-by-Organ Overview
1. Infectious Mononucleosis (IM) - "Glandular Fever"
Pathogenesis
- Primary EBV infection in adolescents and young adults (15-24 years peak)
- In childhood infection: typically asymptomatic or mild
- In adolescence/adulthood: symptomatic IM in ~50% of primary infections
- Massive polyclonal B-cell proliferation → vigorous CTL response → atypical lymphocytes (Downey cells)
- The profound pharyngo-tonsillar inflammation is partly immunopathological (T-cell mediated)
Classic ENT/Clinical Triad
- Exudative pharyngotonsillitis - severe, confluent white/grey exudate; can be membranous and simulate diphtheria
- Cervical lymphadenopathy - posterior cervical chain predominance (vs. anterior in bacterial tonsillitis); bilateral; tender
- Fever - high-grade, prolonged (1-3 weeks)
Additional Features
| Feature | Detail |
|---|---|
| Palatal petechiae | At the junction of hard and soft palate; relatively specific for IM |
| Periorbital/facial oedema | Especially around eyes |
| Splenomegaly | ~50%; risk of rupture with contact sports |
| Hepatomegaly/hepatitis | Transaminase elevation in 80% |
| Skin rash | ~5% spontaneous; >90% if given ampicillin/amoxicillin (not true allergy; immune complex reaction) - this is the classic Ix pitfall |
| Atypical lymphocytes | Activated CD8+ T cells - >10% of peripheral lymphocytes |
ENT-Specific Complications
1a. Airway Obstruction - The Most Critical ENT Emergency
- Occurs in up to 25% of hospitalized IM patients
- Mechanism: massive lymphoid hyperplasia throughout Waldeyer's ring (tonsils + adenoids + lymphoid tissue) + mucosal oedema
- Can be life-threatening
- Management:
- Corticosteroids (dexamethasone/prednisolone) - first-line; reduces tonsillar oedema within hours
- Humidified oxygen, nebulised adrenaline for severe cases
- Acute tonsillectomy/adenotonsillectomy - when steroids fail; controversial but life-saving in extremis
- Emergency tracheostomy - last resort for complete obstruction
1b. Peritonsillar Abscess (PTA)
- More common in IM than previously thought; some studies report >10% of IM cases develop PTA
- Bilateral PTA more prevalent in IM than in bacterial tonsillitis (EBV causes bilateral tonsillar hypertrophy + immune suppression → bacterial superinfection with Group A Strep, Fusobacterium, S. aureus)
- Mechanism: decreased mucosal antibody production → bacterial attachment to tonsillar epithelium
- Management: aspiration/incision & drainage + antibiotics (avoid amoxicillin - rash risk)
- CT neck mandatory if bilateral PTA or deep neck space infection suspected
1c. Deep Neck Space Infection
- Secondary to tonsillar/PTA spread
- Parapharyngeal / retropharyngeal abscess
- Risk of Lemierre's syndrome (septic thrombophlebitis of internal jugular vein), though more typically caused by Fusobacterium
1d. Otitis Media with Effusion (OME)
- Adenoid hypertrophy in IM → Eustachian tube obstruction → OME
- Usually resolves as IM resolves
Diagnosis of EBV-IM
| Test | Details |
|---|---|
| Monospot test (Heterophile antibody test) | Rapid, cheap; positive in 85-90% of adults; false-negative in <10-year-olds and early IM (<1 week) |
| Paul-Bunnell test | Formal heterophile antibody test; historical predecessor of monospot |
| EBV-specific serology | Most accurate: Anti-VCA IgM (acute), Anti-VCA IgG (past), Anti-EA (active), Anti-EBNA (late seroconversion, indicates past/resolved infection) |
| FBC/Differential | Lymphocytosis; >10% atypical lymphocytes (Downey cells) |
| LFTs | Transaminase elevation in 80% |
| Throat swab | To exclude Group A Strep co-infection (15% co-infection rate) |
EBV Serology Pattern
| Disease Phase | Anti-VCA IgM | Anti-VCA IgG | Anti-EA | Anti-EBNA |
|---|---|---|---|---|
| Acute IM | + | + | +/- | - |
| Past infection | - | + | - | + |
| NPC | - | +++ (high titre) | +/- | + |
| Burkitt lymphoma | - | +++ | +/- | + |
Treatment of IM
- Supportive - rest, analgesics (paracetamol, NSAIDs - avoid aspirin under 16 years), adequate hydration
- Avoid amoxicillin/ampicillin - causes maculopapular rash in ~90%
- Corticosteroids - indicated for: severe airway compromise, thrombocytopenia, haemolytic anaemia, severe hepatitis; NOT routine
- Antivirals (aciclovir) - minimal clinical benefit in uncomplicated IM; may be used in severe/immunocompromised
- Contact sports restriction - 3-4 weeks minimum due to splenic rupture risk
- Antiviral prophylaxis against secondary streptococcal infection - sometimes used
2. Nasopharyngeal Carcinoma (NPC)
Epidemiology and EBV Link
- EBV is found in virtually 100% of undifferentiated (WHO Type III) NPC cases
- Consistently associated by serology, EBER in situ hybridization, and EBV genome detection
- Endemic regions: Southern China (30-50 per 100,000/year; 20x higher than non-endemic populations), Southeast Asia, North Africa, Arctic Inuit populations
- Rare in the West (<1% of all cancers in the US)
- Bimodal age distribution: Peak in teenagers/young adults AND again in 50-60 year age group
- Male:Female ratio = 3:1
"Genetic susceptibility, tobacco smoking, early infection by EBV and consumption of traditional diets, particularly salted fish, are known to contribute."
- Bailey and Love's Short Practice of Surgery, 28th ed.
Aetiological Factors for NPC
| Factor | Contribution |
|---|---|
| EBV infection | Most important; essentially universal in Type III NPC |
| Genetic susceptibility | HLA haplotypes (HLA-A2, HLA-B46 in Cantonese); EBV variant lineages (high-risk variants in Southern Chinese - meta-analysis 2024) |
| Salted fish (nitrosamines) | Major dietary carcinogen; particularly in childhood |
| Tobacco smoking | Modest additional risk |
| Other preserved foods | Nitrosamine-rich fermented/salted foods |
EBV Oncogenic Mechanism in NPC
- LMP1 (Latent Membrane Protein 1) - acts as a constitutively active CD40 receptor mimic → activates NF-κB pathway → anti-apoptotic, pro-proliferative signals → oncogenesis
- LMP2 - PI3K/Akt pathway activation
- EBNA1 - maintains EBV episome in dividing cells
- EBERs (EBV-encoded RNAs) - non-coding RNAs; used for diagnostic EBER ISH staining
- miRBARTs - EBV-encoded microRNAs; target tumour suppressor genes
"The tumour cells contain EBV genomes and express several EBV proteins, including LMP1, which generates oncogenic signals that activate the NF-κB pathway."
- Robbins & Kumar Basic Pathology
WHO Histological Classification of NPC
| Type | Description | EBV Association |
|---|---|---|
| Type I | Keratinizing squamous cell carcinoma | Weak/absent |
| Type II | Non-keratinizing squamous cell carcinoma | Moderate |
| Type III (undifferentiated) | Lymphoepithelioma; large epithelial cells with "syncytial" growth, prominent nucleoli, dense T-lymphocyte infiltrate | Near 100% |
Type III constitutes >90% of NPC in endemic areas; T-cell infiltrate is the immune response to EBV antigens.
Clinical Features of NPC
| Symptom/Sign | Mechanism |
|---|---|
| Neck mass (most common; ~50% at presentation) | Cervical node metastasis (Rouvière's node/retropharyngeal LN → level II/III) |
| Nasal obstruction | Tumour mass in nasopharynx |
| Nosebleed (epistaxis) | Mucosal invasion |
| Nasal voice / hyponasality | Nasopharyngeal obstruction |
| Neural signs (cranial nerve palsies) | Skull base invasion: CN VI (abducens - lateral rectus palsy = most common), CN V (trigeminal - facial numbness), CN III/IV |
| No hearing / OME / conductive hearing loss | Eustachian tube obstruction → OME (very characteristic - unilateral OME in an adult mandates nasopharyngeal examination) |
| Neck nodes (bilateral or unilateral, often matted) | Extensive nodal spread; retropharyngeal nodes first, then levels II/III/V |
"In about 5% of patients, the nasopharynx may look normal or minimally asymmetrical but contains submucosal NPC." - Bailey & Love
Diagnosis
- Nasal endoscopy + biopsy - direct visualization; biopsy from lateral pharyngeal recess (fossa of Rosenmuller) most productive
- MRI - gold standard for extent, perineural spread, skull base, intracranial extension
- CT chest/abdomen - distant metastases
- PET-CT - nodal and distant staging
- EBV DNA (plasma) - highly sensitive/specific; used for screening, monitoring treatment response, predicting relapse
- EBER ISH - definitive histological confirmation of EBV in tumour cells
- EBV serology (VCA IgA, EA IgA) - elevated in NPC; used for population screening in endemic areas
Staging and Treatment
| Stage | Treatment |
|---|---|
| Stage I (T1N0M0) | Definitive RT alone (IMRT, 70 Gy) |
| Stage II (T2N0/T1-2N1) | Controversial; CRT increasingly used |
| Stage III-IVA (locally advanced) | Concurrent CRT (cisplatin + IMRT) ± induction or adjuvant chemotherapy |
| Stage IVB (metastatic) | Chemotherapy (cisplatin + 5-FU or gemcitabine + cisplatin) ± immunotherapy |
- IMRT local/locoregional progression-free rates: 95-98% (UCSF series)
- RTOG 02-25: excellent 2-year locoregional control of 90% in multi-institutional setting
- Induction TPF (docetaxel + cisplatin + 5-FU) before CRT: improved 3-year failure-free survival (80% vs 72%), OS (92% vs 86%)
- 5-year OS: 36-58% overall; stage I/II approaches 90%+; distant metastasis remains dominant failure mode (up to 30%)
- Circulating EBV DNA post-RT: indicates high relapse risk; guides adjuvant therapy decisions (NRG HN001 trial)
- Bevacizumab + CRT: feasibility demonstrated (RTOG 06-15)
- Immune checkpoint inhibitors (pembrolizumab, nivolumab): active in recurrent/metastatic NPC; EBV-specific T-cell responses make NPC potentially immunotherapy-sensitive
"Circulating EBV DNA after completion of RT appears to indicate a high risk of relapse."
- Cummings Otolaryngology
3. EBV-Associated Lymphomas with ENT Manifestations
3a. Burkitt Lymphoma
- EBV association: ~100% of African (endemic) Burkitt; ~20% of sporadic Burkitt
- Most common childhood malignancy in sub-Saharan Africa; often presents with jaw/facial bone involvement (classic "African" Burkitt)
- The jaw tumour - rapidly expanding lytic bone lesion of the mandible or maxilla - is the hallmark ENT manifestation
- Histology: "starry sky" appearance (macrophages engulfing apoptotic tumour cells)
- EBV latency I (EBNA1 only)
- t(8;14) translocation: MYC oncogene juxtaposed to IgH gene → constitutive MYC overexpression
- Treatment: intensive cyclophosphamide-based chemotherapy; excellent response
3b. Hodgkin Lymphoma
- EBV association: ~40-60% of mixed cellularity subtype; ~20% of nodular sclerosis subtype
- Reed-Sternberg cells contain EBV (Latency II: LMP1/LMP2 + EBNA1)
- Presents with cervical lymphadenopathy in ~70% - highly relevant to ENT
- Level II/III neck nodes most commonly involved
- "B symptoms": fever, night sweats, weight loss
- Requires excision biopsy for diagnosis (FNA insufficient)
- Treatment: ABVD chemotherapy ± RT
3c. NK/T-Cell Lymphoma (Lethal Midline Granuloma)
- EBV-positive in nearly 100% of cases (Latency II)
- Originates from NK cells or cytotoxic T cells
- Classic ENT presentation: Destructive midline facial/nasal lesion - ulceration and necrosis of the nasal septum, hard palate, midface
- Often mistaken for Wegener's granulomatosis (GPA) or fungal infection
- Diagnosis: biopsy (EBER ISH confirms EBV); CXCL9, CD56, granzyme B, TIA-1 positive
- Predominantly in Asia and Central/South America
- Treatment: non-anthracycline-based (L-ASPA regimens: SMILE protocol) + involved-field RT; poor prognosis if disseminated
3d. Post-Transplant Lymphoproliferative Disorder (PTLD)
- EBV latency III (all EBNAs + LMPs expressed due to absent T-cell immune control)
- Occurs in immunocompromised patients: solid organ transplant, haematopoietic stem cell transplant, HIV/AIDS
- In solid organ transplant: can manifest as tonsillar/Waldeyer's ring lymphoma or cervical lymphadenopathy
- Spectrum: early polyclonal hyperplasia → monomorphic DLBCL-like
- Treatment: reduce immunosuppression + rituximab ± chemotherapy
4. EBV and Other ENT-Relevant Conditions
4a. Chronic Active EBV Infection (CAEBV)
- Rare; defined as persistent EBV infection >3 months with tissue damage
- Elevated EBV DNA in blood + tissue
- Manifestations: chronic pharyngitis, lymphadenopathy, fever, hepatosplenomegaly, skin lesions (hydroa vacciniforme), hearing loss
- Can progress to NK/T-cell lymphoma
- Treatment: haematopoietic stem cell transplantation
4b. Oral Hairy Leukoplakia
- EBV lytic replication in lateral tongue epithelium
- White, corrugated, non-removable plaques on lateral border of tongue
- Classic marker of HIV infection/immunosuppression
- Also occurs in other immunosuppressed states
- Benign; does not transform malignantly
- Treatment: aciclovir/valaciclovir if symptomatic; resolves with antiretroviral therapy
4c. EBV and Sinonasal Disease
- SNUC (Sinonasal Undifferentiated Carcinoma): characteristically EBV-negative (important distinguishing feature from NPC)
- EBV positivity in sinonasal undifferentiated tumours should prompt re-classification as nasopharyngeal carcinoma or NK/T-cell lymphoma
- Sinonasal lymphomas: EBV-associated NK/T-cell lymphoma affects nasal cavity primarily
4d. Salivary Gland Lymphoepithelial Lesions
- Lymphoepithelial cysts and lesions of parotid gland can occur in EBV/HIV co-infection
- Benign lymphoepithelial lesion (BLEL) of parotid: bilateral parotid enlargement in HIV; EBV associated
- Differential from Sjögren's syndrome, lymphoma
5. EBV-Specific Diagnostic Tests Summary
| Test | Sensitivity | Specificity | Use |
|---|---|---|---|
| Monospot (Heterophile) | 85-90% adults | ~99% | Rapid IM screening; poor <10 yrs |
| Anti-VCA IgM | ~97% | High | Acute primary EBV infection |
| Anti-VCA IgG | >95% | Moderate | Confirms past infection |
| Anti-EBNA | High (late) | High | Confirms resolved infection; absent in acute IM |
| Anti-EA IgA, VCA IgA | ~70-90% | High for NPC | NPC screening in endemic areas |
| Plasma EBV DNA (quantitative PCR) | ~96% | ~95% | NPC staging, treatment monitoring, relapse detection |
| EBER ISH (in situ hybridization) | Near 100% | Near 100% | Tissue confirmation of EBV; gold standard histological test |
6. ENT-Specific Implications Summary Table
| Condition | EBV Type/Role | ENT Manifestation | Key Points |
|---|---|---|---|
| Infectious Mononucleosis | Primary lytic + CTL | Exudative tonsillitis, cervical LN, airway obstruction, PTA | Avoid amoxicillin; steroids for airway |
| Nasopharyngeal Carcinoma (Type III) | Latency II; LMP1 (NF-κB) | Nasopharyngeal mass, OME, cranial nerve palsies, neck nodes | EBV DNA = monitoring tool; IMRT + cisplatin |
| Burkitt Lymphoma | Latency I; EBNA1 | Jaw/facial bone destruction in endemic form | t(8;14); MYC; starry sky histology |
| Hodgkin Lymphoma | Latency II; RS cells | Cervical adenopathy | ~50% EBV+; excision biopsy needed |
| NK/T-Cell Lymphoma | Latency II; near 100% | Midline nasal destruction, palate ulceration | "Lethal midline granuloma"; SMILE protocol |
| PTLD | Latency III | Tonsillar/Waldeyer's ring mass | Post-transplant; reduce immunosuppression |
| Oral Hairy Leukoplakia | Lytic | Lateral tongue white corrugated plaques | HIV marker; benign |
| CAEBV | Persistent infection | Chronic pharyngitis, LN, hearing loss | Risk of lymphoma transformation |
Nasal myiasis
Nasal myiais
nasal myiasis treatment diagnosis Cochliomyia Lucilia
nasal myiasis ENT management larvae
nasal myiasis fly larvae ENT infestation pathology treatment ivermectin turpentine 2023 2024
PMID: 41003567
PMID: 42110092
nasal myiasis causative flies Cochliomyia Lucilia Calliphora Chrysomya clinical features maggots nasal cavity endoscopy diagnosis India Africa
https://pmc.ncbi.nlm.nih.gov/articles/PMC6848309
PMID: 40065968
Nasal Myiasis (Rhinomyiasis)
Definition
Classification of Myiasis (by Parasite Biology)
| Type | Definition | Causative Flies |
|---|---|---|
| Obligatory myiasis | Larvae can ONLY develop in living host tissue | Cochliomyia hominivorax (New World screwworm), Chrysomya bezziana (Old World screwworm), Wohlfahrtia magnifica, Oestrus ovis |
| Facultative myiasis | Larvae normally develop in carrion but can invade living/necrotic tissue | Calliphora, Lucilia (greenbottle), Phormia, Musca domestica |
| Accidental myiasis | Larvae accidentally ingested or deposited; not adapted to host | Various species |
Classification by Anatomical Site
| Site | Name |
|---|---|
| Nasal cavity / sinuses | Nasal / Rhinomyiasis |
| Ear canal | Aural myiasis |
| Eye / orbit | Ophthalmomyiasis |
| Oral cavity | Oral myiasis |
| Skin (furuncle-like) | Furuncular myiasis |
| Wound | Wound myiasis |
| Gastrointestinal | Intestinal myiasis |
| Urogenital | Urogenital myiasis |
Causative Organisms
Obligate Parasites (Most Destructive)
| Organism | Common Name | Geography | Key Feature |
|---|---|---|---|
| Cochliomyia hominivorax | New World screwworm | Americas (Central/South America, Caribbean) | Most destructive; invades healthy tissue; mandatory reporting in some countries |
| Chrysomya bezziana | Old World screwworm | Africa, Asia, Middle East | Equally destructive to C. hominivorax in Old World |
| Wohlfahrtia magnifica | Flesh fly | Europe, Middle East, North Africa | Obligate; deposits larvae (viviparous) directly into body orifices |
| Oestrus ovis | Sheep nasal botfly | Worldwide (sheep-rearing regions); Mediterranean, North Africa, Middle East | Most common cause of nasal myiasis in immunocompetent humans in Mediterranean/North Africa; zoonotic; normally infests sheep |
Facultative Parasites (Wound-Based)
| Organism | Common Name | Geography |
|---|---|---|
| Lucilia sericata / cuprina | Greenbottle fly | Worldwide; common in India, UK |
| Calliphora spp. | Bluebottle fly | Worldwide |
| Chrysomya spp. | Various | Africa, Asia |
| Musca domestica | Common housefly | Worldwide |
| Sarcophaga spp. | Flesh fly | Worldwide |
Oestrus ovis is notable as the most common cause of human nasal myiasis in immunocompetent patients - it is a zoonosis from sheep that can accidentally deposit larvae in humans, presenting as a syndrome mimicking allergic rhinitis (PMID 41003567, Trop Med Infect Dis 2025).
Epidemiology
| Parameter | Data |
|---|---|
| Geography | Tropical and subtropical regions predominantly; Sub-Saharan Africa, Indian subcontinent, Middle East, Central/South America, Mediterranean |
| Seasonality | More common in hot, dry months (increased fly activity) |
| Age/Sex | Any age; older neglected patients most common in severe cases |
| Socioeconomic | Strongly associated with poverty, poor sanitation, rural areas |
| Setting | More common in resource-limited settings; hospital-acquired cases reported in ICUs (especially in endemic areas) |
Predisposing Factors
High-Risk Patient Profile ("Classic" Case)
| Factor | Mechanism |
|---|---|
| Pre-existing nasal disease | Atrophic rhinitis (ozaena) - most important; foetid discharge attracts flies |
| Poor nasal hygiene / neglect | Attracts ovipositing flies |
| Chronic rhinosinusitis | Mucopurulent discharge; attracts flies |
| Old age / debility | Reduced awareness, immobility |
| Mental illness / psychiatric disorder | Inability to self-care |
| Alcoholism / drug addiction | Impaired consciousness; poor hygiene |
| Immunosuppression | Diabetes mellitus, HIV, malnutrition, malignancy |
| Open wounds / post-surgical | Exposed necrotic tissue |
| Unconsciousness / ICU patients | Direct access for fly oviposition |
| Nasal foreign body | Fetor attracts flies |
| Homeless / outdoor sleeping | Direct exposure |
Important: Recent series confirm nasal myiasis can occur in fully immunocompetent individuals without any predisposing factors, particularly with Oestrus ovis - always consider the diagnosis in endemic areas regardless of host immune status (PMID 42110092, 40065968).
Life Cycle of the Fly - Relevance to Pathology
Adult fly (gravid female)
↓
Attracted by: odour (fetor, necrosis, blood, discharge), body warmth, moisture
↓
Deposits EGGS (or larvae if viviparous) in/around nasal opening, wounds, body orifices
↓
Eggs hatch in 8-24 hours (temperature/species dependent)
↓
1st stage larvae (L1) → feed on mucosa, blood, secretions → 2nd stage (L2) → 3rd stage (L3)
↓
Larvae equipped with: HOOKED mouthparts (for tissue attachment/feeding)
POSTERIOR SPIRACLES (for breathing)
ROW OF SPINES (for locomotion and anchorage)
↓
Larvae can invade: nasal cavity → maxillary/ethmoidal/sphenoid sinuses
→ orbit → anterior cranial fossa (via cribriform plate)
→ intracranial complications (rare)
↓
Fully grown larvae drop off, pupate in soil
↓
Adult fly emerges after 3-9 weeks
Pathology
Tissue Destruction
- Larvae produce proteolytic enzymes (collagenase, proteases) that actively digest living tissue
- They have chitinous hooks and spines that anchor them and facilitate burrowing
- Create sinus tracts through mucosa into bone and deeper structures
- Each larva individually causes a small lesion; hundreds of larvae collectively cause massive destruction
- Bone erosion is a major concern - turbinates, septum, palate, orbital walls, skull base
Complications
| Complication | Mechanism |
|---|---|
| Turbinate destruction | Direct larval feeding + enzymatic digestion |
| Septal perforation | Cartilage/bone destruction |
| Palate perforation | Inferior spread |
| Orbital cellulitis/invasion | Medial orbital wall breach |
| Orbital myiasis | Larvae migrating through nasolacrimal duct or through ethmoids |
| Meningitis | Cribriform plate erosion → intracranial extension |
| Intracranial abscess | Larval migration with secondary infection |
| Fatal haemorrhage | Vascular erosion |
| Secondary bacterial infection | Mixed oral flora, Staphylococci, Streptococci, anaerobes |
| Sepsis | Secondary bacteraemia |
Clinical Features
Symptoms
| Symptom | Notes |
|---|---|
| Nasal obstruction | Usually unilateral initially |
| Epistaxis (nasal bleeding) | Often the presenting complaint; may be profuse |
| Foul-smelling nasal discharge | Serosanguineous/purulent; particularly repulsive odour |
| Crawling / movement sensation in the nose | Pathognomonic - sensation of "something moving" inside the nose |
| Facial pain / headache | Sinus involvement; can be severe |
| Toothache | Maxillary sinus floor involvement |
| Passage of maggots from the nose | Spontaneous expulsion - the patient may actually see maggots |
| Periorbital / midfacial oedema | Inflammatory spread; sinusitis |
| Pruritus / itching | Larval irritation |
| Fever | Secondary infection / systemic inflammatory response |
In Oestrus ovis infestation: presentation often mimics allergic rhinitis - sneezing, watery rhinorrhoea, pruritus - making early diagnosis challenging. In a series of 14 cases (PMID 41003567), all patients were initially suspected of allergic rhinitis before nasal endoscopy revealed larvae.
Signs
- Maggots visible in nasal cavity - wriggling white/cream-coloured larvae of varying sizes
- Mucosal ulceration, slough, necrosis
- Serosanguineous or mucopurulent discharge
- Turbinate swelling or destruction
- Midfacial oedema
- In advanced cases: exposed cartilage/bone, septal perforation, orbital signs
Diagnosis
1. Clinical Suspicion
- Key: Think of it in any patient from an endemic area with unilateral nasal symptoms + foetid discharge + history of any predisposing factor
- The crawling/movement sensation is highly suggestive
- Do NOT miss it in immunocompetent patients in endemic areas
2. Nasal Endoscopy - Investigation of Choice
- Rigid nasal endoscopy (0° and 30° scopes) is the gold standard diagnostic and therapeutic tool
- Reveals maggots directly - wriggling larvae in the nasal cavity, meatal regions, sinus ostia
- Identifies extent of mucosal damage, tissue necrosis, bone exposure
- Allows guided extraction
- Positive in ~79% of cases at first examination (some larvae may be hiding in sinuses)
- Repeat endoscopy mandatory to confirm complete clearance
3. CT Scan Paranasal Sinuses
- Essential for:
- Extent of sinus involvement (maxillary, ethmoidal, sphenoid, frontal)
- Bony erosion (turbinates, septum, palate, orbital wall, skull base)
- Orbital / intracranial extension
- Surgical planning
- CT findings: mucosal thickening, heterogeneous secretions, bony erosion, soft tissue opacification of sinuses
- May reveal larvae as small hyperdense foci within opacified sinuses
4. Parasitological Identification
- Larvae identification by morphology under microscopy:
- Posterior spiracles - key identification feature (species-specific spiracle pattern)
- Body spines arrangement
- Size and stage (L1/L2/L3)
- Culture: larvae reared to adult fly → definitive species identification
- Important for epidemiological reporting (obligate parasites like C. hominivorax may be notifiable)
5. Blood Tests
- FBC: eosinophilia (variable; more common with Oestrus ovis)
- Inflammatory markers (CRP, ESR): elevated with secondary infection
- Blood cultures: if sepsis suspected
- Serology: EBV/HIV/immunosuppression workup if no obvious predisposing factor
- Blood glucose: exclude diabetes mellitus
Treatment
Step 1: Kill/Immobilise the Larvae
A. Chloroform + Turpentine Oil (1:4 ratio) - Traditional Method
- Instilled into the nasal cavity
- Immobilises and irritates larvae, causing them to surface
- Effective but:
- Longer hospital stay needed
- More repeated procedures required
- More tissue damage from repeat manipulation
- Turpentine is irritating to mucosa
B. Topical Ivermectin (1% solution)
- Applied topically to nasal mucosa
- Kills larvae rapidly by binding glutamate-gated chloride channels → irreversible paralysis
- Can be prepared from oral ivermectin tablets dissolved in normal saline
C. Nasal Saline Irrigation (Oestrus ovis)
- High-volume saline irrigation flushes Oestrus ovis larvae out effectively (larvae are smaller/less adherent)
- Combined with albendazole/ivermectin systemically
Step 2: Mechanical Extraction
- Rigid nasal endoscopy with Tilley's nasal forceps / crocodile forceps / suction
- Remove all larvae systematically - count larvae; must account for all
- Do NOT rupture larvae during extraction - retained larval fragments cause severe foreign body granulomatous reaction and abscess formation
- Irrigation with saline to flush out smaller larvae
- Session repeated at 24 hours and 48 hours until complete clearance confirmed
- All extracted larvae should be examined and counted
Step 3: Systemic Medical Therapy
Ivermectin (Cornerstone of Modern Treatment)
- Mechanism: Semi-synthetic macrocyclic lactone derived from Streptomyces avermitilis; binds glutamate-gated Cl⁻ channels in invertebrate nerve/muscle → irreversible hyperpolarisation → paralysis and death of larvae
- Oral dose: 200 mcg/kg single dose (typically 2 × 6 mg tablets, 24 hours apart in a 60-70 kg adult)
- Effect: Larvae killed and expelled within 4-5 hours in most patients
- Evidence: In a prospective RCT of 80 patients (Ivermectin group vs. turpentine group):
- 76/80 (95%) patients in ivermectin group had complete resolution of maggots within 4-5 hours
- Ivermectin group: shorter hospital stay, less tissue damage, faster healing, better re-epithelialisation at 1 week
- Turpentine group: required repeated daily manual removal over several days; greater tissue loss
- Also available as topical 1% ivermectin solution
Albendazole
- Antihelminthic with some antilarval activity
- Used particularly for Oestrus ovis nasal myiasis (PMID 41003567, 42110092)
- Oral albendazole + corticosteroids + antihistamines effective in O. ovis series (resolution in ~4 days average)
Step 4: Adjuvant Management
| Component | Detail |
|---|---|
| Antibiotics | Broad-spectrum IV antibiotics (ceftriaxone + metronidazole or clindamycin) for secondary bacterial infection; adjust based on culture |
| Analgesics | Adequate pain relief |
| Nasal irrigation | Saline irrigation 2-3x daily to flush debris, larvae, secretions |
| Corticosteroids | For Oestrus ovis (inflammatory response management) + if orbital oedema |
| Antihistamines | For Oestrus ovis (allergic-type response) |
| Surgical debridement | For necrotic tissue, slough in sinuses; FESS if sinus involvement severe |
| Treatment of predisposing condition | Diabetes control, nutritional support, HIV management, treatment of atrophic rhinitis |
Treatment Algorithm
Nasal Myiasis Confirmed by Endoscopy
↓
CT PNS (assess extent + bone erosion)
↓
Immobilise larvae:
- Chloroform:Turpentine (1:4) instillation
OR
- Topical ivermectin 1% nasal drops
↓
Endoscopic mechanical extraction (Tilley's forceps + suction)
Count and account for ALL larvae
↓
Oral Ivermectin 200 mcg/kg (2 doses 24h apart)
+ Systemic antibiotics
+ Analgesics
+ Saline irrigation
↓
Repeat endoscopy at 24h and 48h
→ Continue until ZERO larvae confirmed
↓
Wound care + debridement of necrotic tissue
± FESS for sinus involvement
↓
Treat underlying predisposing condition
↓
Discharge + outpatient endoscopy follow-up
Complications (if Untreated or Delayed)
| Complication | Severity |
|---|---|
| Turbinate/septal/palate destruction | Severe; permanent |
| Orbital cellulitis / orbital myiasis | Sight-threatening |
| Blindness (optic nerve compression) | Permanent |
| Meningitis / brain abscess | Life-threatening |
| Fatal haemorrhage | Life-threatening |
| Sepsis / multi-organ failure | Life-threatening |
| Oronasal fistula | Significant morbidity |
Prevention
| Strategy | Detail |
|---|---|
| Personal hygiene | Regular nasal irrigation/cleaning; wound care |
| Insect repellents | DEET-based repellents around body orifices in endemic areas |
| Fly control | Screens on windows/doors; insecticide sprays |
| Wound care | Prompt dressing of wounds; covering wounds, especially in outdoor/rural settings |
| Treatment of predisposing conditions | Early management of atrophic rhinitis, diabetes, immunosuppression |
| Sanitation | Proper waste disposal; reduce fly breeding sites |
| Hospital infection control | Fly screens in ICUs and wards in endemic regions (hospital-acquired myiasis is a recognized entity in tropical ICUs) |
| Public health education | Community awareness in endemic areas |
Key Summary Points
Nasal Myiasis - ENT Essentials
Definition: Fly larval infestation of nasal cavity ± paranasal sinuses
Most important organisms:
• Oestrus ovis (most common in immunocompetent; mimics allergic rhinitis)
• Cochliomyia hominivorax (Americas; most destructive)
• Chrysomya bezziana (Asia/Africa; equally destructive)
• Lucilia, Calliphora (facultative; associated with necrotic tissue/atrophic rhinitis)
Classic risk factors: atrophic rhinitis, diabetes, neglect, poor hygiene, ICU
(BUT: immunocompetent cases well-documented - always consider in endemic areas)
Hallmark symptom: CRAWLING SENSATION inside nose
Hallmark sign: Maggots visible on endoscopy
Diagnosis: Nasal endoscopy (gold standard) + CT PNS
Treatment:
1. Immobilise: chloroform:turpentine (1:4) OR topical ivermectin
2. Mechanical extraction: endoscopic, account for ALL larvae
3. Oral ivermectin 200 mcg/kg × 2 doses (significantly better outcomes)
4. Antibiotics + saline irrigation + wound care
5. Treat underlying condition
Key danger: Larvae DO NOT stop - orbital invasion, intracranial extension, death
Key rule: DO NOT rupture larvae during extraction (foreign body granuloma)
Hemifacial spasm