Corneal ulcer
Reading File
Finding Sources
Finding Sources
Searching PubMed
"corneal ulcer" AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full clinical overview of corneal ulcer:
Corneal Ulcer (Infectious Keratitis)
Definition and Pathogenesis
A corneal ulcer is a serious infection involving multiple layers of the cornea. It develops when the epithelial barrier is breached - by trauma, desiccation, desquamation, or direct microbial invasion - allowing organisms to invade the underlying corneal stroma. Some bacteria (N. gonorrhoeae, N. meningitidis, C. diphtheriae, H. influenzae) can penetrate even an intact epithelium. Infections may be polymicrobial (bacterial and fungal co-infection). - Tintinalli's Emergency Medicine, p. 241; Kanski's Clinical Ophthalmology 10e, p. 226
Etiology / Causative Organisms
| Category | Organisms |
|---|---|
| Bacteria | Pseudomonas aeruginosa, Streptococcus pneumoniae, Staphylococcus species, Moraxella species, Serratia species |
| Viruses | Herpes simplex, Varicella zoster |
| Fungi | Candida, Aspergillus, Penicillium, Cephalosporium |
| Protozoa | Acanthamoeba |
- Pseudomonas aeruginosa accounts for >60% of contact lens-related keratitis - aggressive and potentially destructive.
- S. aureus produces a focal, well-defined white or yellow-white infiltrate.
- Streptococcal infections tend to be aggressive.
- Fungi must be considered after trauma with vegetable matter (e.g., tree branch) or in immunosuppressed patients.
- Kanski's Clinical Ophthalmology 10e, p. 226; The Wills Eye Manual, p. 202
Risk Factors
- Contact lens wear - the most important risk factor, especially extended-wear and soft lenses; risk increases dramatically with overnight wear and poor lens hygiene
- Trauma (including LASIK refractive surgery)
- Exposure keratitis / incomplete eyelid closure (Bell's palsy)
- Prior ocular surgery
- Topical or systemic corticosteroids / immunosuppressants
- Diabetes mellitus
- Vitamin A deficiency
- Local or systemic immunosuppression
- Kanski's Clinical Ophthalmology 10e, p. 226; Tintinalli's, p. 241
Clinical tip: Bacterial corneal ulceration should be excluded in any contact lens wearer who presents with painful red eye and blurred vision. - Kanski's 10e
Clinical Features
Symptoms
- Unilateral eye pain (moderate to severe)
- Photophobia
- Blurred / decreased vision (especially if ulcer is central)
- Mucopurulent or purulent discharge
- Foreign body sensation
- Red eye; acute contact lens intolerance
Signs (slit-lamp examination)
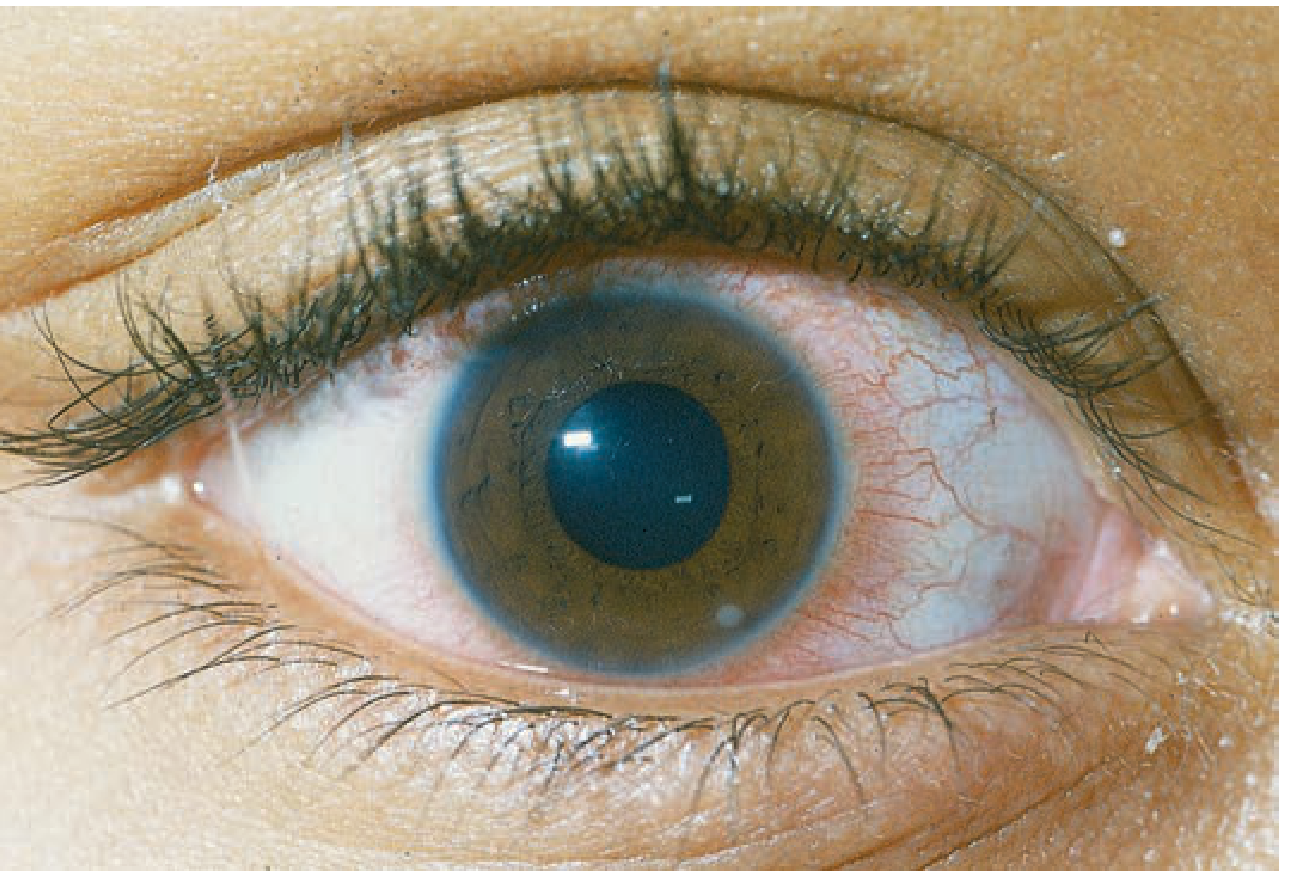
Critical finding: Focal white stromal opacity (infiltrate) associated with an overlying epithelial defect and underlying stromal thinning/tissue loss.
Additional findings in increasing severity:
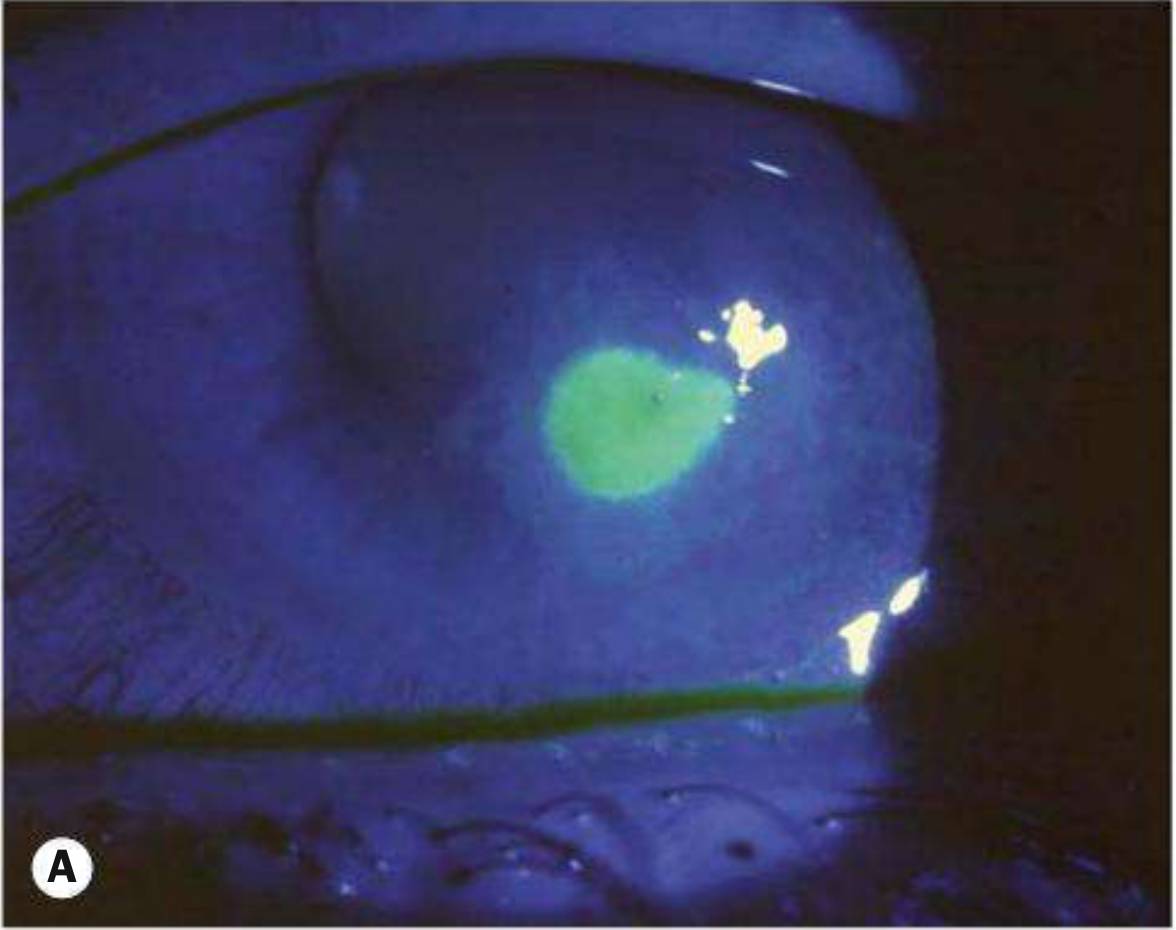
- Epithelial defect (stains with fluorescein)
- Circumcorneal (ciliary) injection
- Stromal edema, Descemet membrane folds
- Anterior chamber reaction (flare + cells) - hypopyon in moderate-severe cases
- Miotic pupil from ciliary spasm (associated iritis)
- Mucopurulent discharge; eyelid and conjunctival edema
- Posterior synechiae, raised IOP in severe cases
- Descemetocele formation and corneal perforation in very severe cases (especially Pseudomonas)
- Scleritis with perilimbal infection
- Endophthalmitis is rare without perforation
- Kanski's Clinical Ophthalmology 10e, p. 227; The Wills Eye Manual, p. 199
Fluorescein-stained bacterial corneal ulcer (Kanski's Fig. 7.7A):
Large corneal ulcer (Pseudomonas) with dense white stromal infiltrate (Kanski's Fig. 7.7D):

Corneal ulcer at 5 o'clock (Tintinalli's Fig. 241-32):
Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Fungal keratitis | Feathery/irregular borders, satellite lesions; after vegetable trauma or contact lens wear |
| Acanthamoeba | Extremely painful; perineural invasion; ring-shaped infiltrate in late stages; soft CL wearer; swimming/hot tub history |
| HSV keratitis | Dendritic epithelial ulcer; recurrent unilateral disease; eyelid vesicles |
| Atypical mycobacteria | Post-LASIK; indolent course; requires Lowenstein-Jensen media (kept 8 weeks) |
| Staphylococcal hypersensitivity | Peripheral, multiple, often bilateral; clear space between infiltrate and limbus; minimal AC reaction |
| Sterile corneal infiltrates | Small, peripheral, subepithelial; minimal staining; no/minimal AC reaction; diagnosis of exclusion |
| Topical anesthetic abuse | Large ring opacity; poor response to treatment; mimics Acanthamoeba/HSV |
- The Wills Eye Manual, pp. 200-201
Investigations
Corneal Scraping and Culture
- Scrape the center and edges of the ulcer under slit-lamp
- Specimens inoculated directly onto culture media at the bedside (C-streaks)
- Scraping may be delayed up to 12 hours if antibiotics have already been started
Culture media:
| Medium | Organisms Detected |
|---|---|
| Blood agar | Most bacteria and fungi (except Neisseria, Haemophilus, Moraxella) |
| Chocolate agar | Fastidious organisms: H. influenzae, Neisseria, Moraxella |
| Sabouraud dextrose agar | Fungi |
| Non-nutrient agar + E. coli | Acanthamoeba |
| Brain-heart infusion | Streptococci, meningococci, fastidious organisms |
| Lowenstein-Jensen | Mycobacteria, Nocardia (keep 8 weeks) |
- Gram stain and KOH preparation for rapid presumptive identification
- PCR/nanopore sequencing for exact species ID and antibiotic resistance profiling
- Culture contact lens cases and solution bottles as well (patient must NOT clean case first)
- Conjunctival swabs may supplement corneal scraping, especially in severe cases
- Kanski's Clinical Ophthalmology 10e, pp. 228-229
Treatment
General Principles
- Treat empirically while awaiting culture results
- Corneal infections are assumed bacterial until proven otherwise
- Contact lens wear must be discontinued immediately
- Do NOT patch the eye (especially in contact lens wearers - rapid infection spread risk)
- Emergent ophthalmology consultation for any significant ulcer
Antibiotic Selection by Risk Level (Wills Eye Manual protocol)
Low risk - Small (<1 mm), peripheral, minimal discharge, no/trace AC reaction, non-CL wearer:
- Fluoroquinolone drops (moxifloxacin, gatifloxacin, besifloxacin, levofloxacin) q1-2h while awake
- OR polymyxin B/trimethoprim q1-2h while awake
Borderline risk - 1-1.5 mm peripheral, or any smaller infiltrate with epithelial defect, AC reaction, or moderate discharge:
- Fluoroquinolone q1h around the clock ± polymyxin B/trimethoprim q1h
- Consider loading dose: q5min x 5 doses, then q30min until midnight, then q1h
Vision-threatening - >1.5-2 mm, in visual axis, or unresponsive to initial therapy:
- Fortified antibiotics (from formulating pharmacy):
- Fortified tobramycin or gentamicin (15 mg/mL) q1h, alternating with
- Fortified cefazolin (50 mg/mL) or vancomycin (25 mg/mL) q1h
- Net: one drop every 30 minutes around the clock
- If Pseudomonas suspected (contact lens wearer): fortified tobramycin q30min + fortified ceftazidime q1h + fluoroquinolone q1h
- Vancomycin reserved for resistant organisms or MRSA risk
Note: Moxifloxacin/besifloxacin have slightly better gram-positive coverage; gatifloxacin/ciprofloxacin have slightly better Pseudomonas/Serratia coverage.
Adjunctive / Special Circumstances
- Cycloplegic (cyclopentolate 1-2%, atropine 1%) for iritis-related spasm and pain
- Oral fluoroquinolones (ciprofloxacin 500 mg bid or moxifloxacin 400 mg daily) for scleral extension or impending perforation
- Neisseria infections: ceftriaxone 1 g IV q12-24h if corneal involvement (systemic spread risk)
- Haemophilus infections: oral amoxicillin/clavulanate (systemic complications possible)
- Atypical mycobacteria: prolonged topical moxifloxacin/gatifloxacin ± fortified amikacin (15 mg/mL) ± oral clarithromycin 500 mg bid
When to Admit
- Sight-threatening infection or impending perforation
- Difficulty self-administering drops at required frequency
- High noncompliance risk
- Suspected topical anesthetic abuse
- IV antibiotics needed (Neisseria with corneal involvement)
- Corneal perforation or scleral extension
- The Wills Eye Manual, pp. 203-207; Tintinalli's Emergency Medicine, p. 241
Follow-Up
Daily evaluation initially. Key parameters to track:
- Pain level
- Epithelial defect size (may initially increase after scraping)
- Infiltrate size and depth
- Anterior chamber reaction
- IOP (can rise; treat if elevated)
Signs of improvement: reduced lid edema/chemosis, shrinking epithelial defect, decreasing infiltrate density, reduced anterior chamber inflammation. - Kanski's 10e, p. 228; Wills Eye Manual, p. 208
Complications
- Corneal scarring and permanent visual loss
- Descemetocele (Descemet membrane bulging through thinned stroma)
- Corneal perforation (especially Pseudomonas)
- Hypopyon
- Endophthalmitis (rare without perforation)
- Elevated IOP / secondary glaucoma
- Posterior synechiae
- Persistent epithelial defects (may require amniotic membrane grafting - recent systematic review, PMID 39257085)
Summary Table: Organism-Specific Clues
| Organism | Clinical Hint |
|---|---|
| Pseudomonas | Contact lens wearer; aggressive, rapidly progressive; >60% of CL ulcers |
| S. pneumoniae / S. aureus | Common in non-CL wearers; following trauma |
| Fungi (Aspergillus/Fusarium) | Feathery borders, satellite lesions; vegetable/agricultural trauma |
| Acanthamoeba | Extreme pain; swimming/hot tub; ring infiltrate late |
| HSV | Dendrites; recurrent; unilateral |
| Atypical mycobacteria | Post-LASIK; indolent |
| Moraxella | Alcoholism, immunosuppression |
NDPS cfm mbbs 3rd year short notes
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive material from two forensic medicine textbooks. Here are complete short notes on NDPS Act for MBBS 3rd year CFM/Forensic Medicine:
NDPS Act - Short Notes (CFM / Forensic Medicine, MBBS 3rd Year)
Full Form & Introduction
NDPS = Narcotic Drugs and Psychotropic Substances Act, 1985
- Passed by the Parliament of India in 1985
- Extended to the whole of India
- Administered by the Ministry of Finance (Department of Revenue)
Acts Repealed by NDPS Act 1985
NDPS Act repeals three earlier Acts:
- The Opium Act, 1857
- The Opium Act, 1878
- The Dangerous Drugs Act, 1930
Objectives of the NDPS Act
- Consolidate and amend laws relating to narcotic drugs
- Strengthen existing controls over drugs of abuse
- Enhance penalties, especially for illegal trading offences
- Exercise effective control over psychotropic substances
- Implement international conventions (UN Single Convention on Narcotic Drugs, 1961; 1971 Convention on Psychotropic Substances; 1988 UN Convention Against Illicit Traffic)
- The Essentials of Forensic Medicine & Toxicology 36e; PC Dikshit's Textbook of FMT
Important Definitions Under NDPS Act
Narcotic Drug
Means: Coca leaf, Cannabis (Hemp), Opium, Poppy straw and includes all manufactured drugs.
Manufactured Drug
- All coca derivatives, medicinal cannabis, opium derivatives and poppy straw concentrate
- Any other narcotic substance declared as such by the Central Government
Psychotropic Substance
Any substance (natural or synthetic) or any natural material or any salt or preparation of such substance included in the schedule to the Act.
- The schedule lists 77 psychotropic substances
- Examples: LSD, amphetamine, tranquilizers, barbiturates, benzodiazepines, methaqualone, ketamine, psilocybin, phencyclidine, mescaline
Addict
A person addicted to any narcotic drug or psychotropic substance.
Small Quantity
Quantity specified by the Central Government in the Official Gazette. Burden of proof that possession was for personal consumption lies on the person found in possession.
Commercial Quantity
Quantity specified by the Central Government, attracting maximum penalty.
Quantity Schedule and Penalties
| Drug | Small Quantity | Commercial Quantity |
|---|---|---|
| Cocaine | 2 g | 100 g |
| Heroin | 5 g | 250 g |
| Opium | 25 g | 2.5 kg |
| Charas / Hashish | 100 g | 1 kg |
| Ganja | 1 kg | 20 kg |
Punishment Grid
| Quantity | Imprisonment | Fine |
|---|---|---|
| Small quantity | Up to 6 months | Up to ₹10,000 |
| Between small and commercial | Up to 10 years | Up to ₹1 lakh |
| Commercial quantity | 10-20 years (rigorous imprisonment, not less than 10 years) | ₹1-2 lakh (not less than ₹1 lakh; court may exceed ₹2 lakh for reasons recorded) |
| Repeat offence (commercial) | Death sentence |
- PC Dikshit's FMT, p. 448; Essentials of FMT 36e, p. 473
Offences Under NDPS Act (Chapter IV)
Punishable contraventions include:
- Cultivation of poppy, cannabis, coca plants without licence
- Production, manufacture, possession, sale, purchase, transport, import, export of narcotic drugs/psychotropic substances
- Embezzlement of opium by a cultivator
- Illegal import/export/transshipment of narcotic drugs
- External dealings in narcotic drugs in contravention of Section 12
- Allowing premises to be used for commission of an offence (S.26)
Note: Ganja possession for personal use may not attract commercial quantity penalties but is still punishable.
Prevention of Illicit Traffic in Narcotic Drugs and Psychotropic Substances Act, 1988 (PITNDPS Act)
- A companion Act to NDPS 1985
- If a person produces, possesses, transports, imports, exports, sells, purchases, or uses any narcotic drug or psychotropic substance (except ganja) - punishable with imprisonment
- Death sentence for repeat offenders
- Provides for preventive detention of persons engaged in illicit drug trafficking
Licensing Requirement
Cultivation of the following requires a licence:
- Poppy plant
- Cannabis plant
- Coca plant
Related Companion Legislation (Important for MCQs)
| Act | Key Point |
|---|---|
| Opium Act, 1857 | Repealed by NDPS; cultivation/possession of opium |
| Opium Act, 1878 | Repealed by NDPS; import/export/transport of opium |
| Dangerous Drugs Act, 1930 | Repealed by NDPS; controlled manufactured drugs |
| Drugs and Cosmetics Act, 1940 | Import, manufacture, distribution, sale of drugs; S. 18 - prohibited acts |
| Drugs & Magic Remedies Act, 1954 | Prohibits advertisements of magic remedies for abortion, contraception, aphrodisiacs, VD |
| Medicinal & Toilet Preparations (Excise Duties) Act, 1956 | Excise duties on preparations containing alcohol and narcotic drugs |
| Prevention of Food Adulteration Act, 1954 | Adulterated food and drugs |
Relevant IPC / BNS Sections on Poisoning
| Section | Provision | Punishment |
|---|---|---|
| Sec. 284 IPC (S. 286 BNS 2023) | Negligent conduct with poisonous substance | Up to 6 months + fine |
| Sec. 299 IPC | Culpable homicide by poisoning | Variable (depending on intent/knowledge) |
| Sec. 300 IPC | Murder by poisoning | Death or life imprisonment |
| Sec. 304A IPC | Causing death by negligence (rash/negligent act) | Up to 2 years + fine |
| Sec. 328 IPC (S. 123 BNS 2023) | Administering stupefying/intoxicating drug to cause hurt or facilitate offence | Up to 10 years + fine |
| Sec. 272-276 IPC (S. 272-280 BNS 2023) | Adulteration of food/drugs | Fine + imprisonment |
Key legal principle: The law does not require an exact definition of "poison" - administration of any substance with intent to cause injury/death is sufficient for conviction. Intent is the key element.
High-Yield Points for Exams (MCQ + Short Notes)
- Year of NDPS Act - 1985 ✔
- Three Acts repealed - Opium 1857, Opium 1878, Dangerous Drugs 1930 ✔
- Narcotic drug definition mnemonic - CCOP → Coca leaf, Cannabis, Opium, Poppy straw + manufactured drugs ✔
- 77 psychotropic substances in the schedule ✔
- Heroin small quantity - 5 g; commercial - 250 g ✔
- Cocaine small quantity - 2 g; commercial - 100 g ✔
- Ganja commercial quantity - 20 kg (highest threshold) ✔
- Commercial quantity punishment - minimum 10 years, maximum 20 years RI + ₹1-2 lakh fine ✔
- Death sentence - for repeat commercial-quantity offenders ✔
- Burden of proof - on the accused to prove personal consumption for small quantity possession ✔
- Cultivation of poppy/cannabis/coca requires licence ✔
- PITNDPS Act 1988 = companion Act for preventive detention and trafficking ✔
Sources: PC Dikshit's Textbook of Forensic Medicine and Toxicology, p. 448-449; The Essentials of Forensic Medicine and Toxicology 36e (2026), p. 473
This is a shared conversation. Sign in to Orris to start your own chat.