Glomerular filtration barrier
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Glomerular Filtration Barrier
The glomerular filtration barrier (GFB) is the specialized, three-layered structure in the renal corpuscle that filters blood from the glomerular capillaries into Bowman's space, producing the primary urine ultrafiltrate (~180 L/day). It filters by size, shape, and electrical charge. Only about 0.01% of plasma protein passes through under normal conditions.
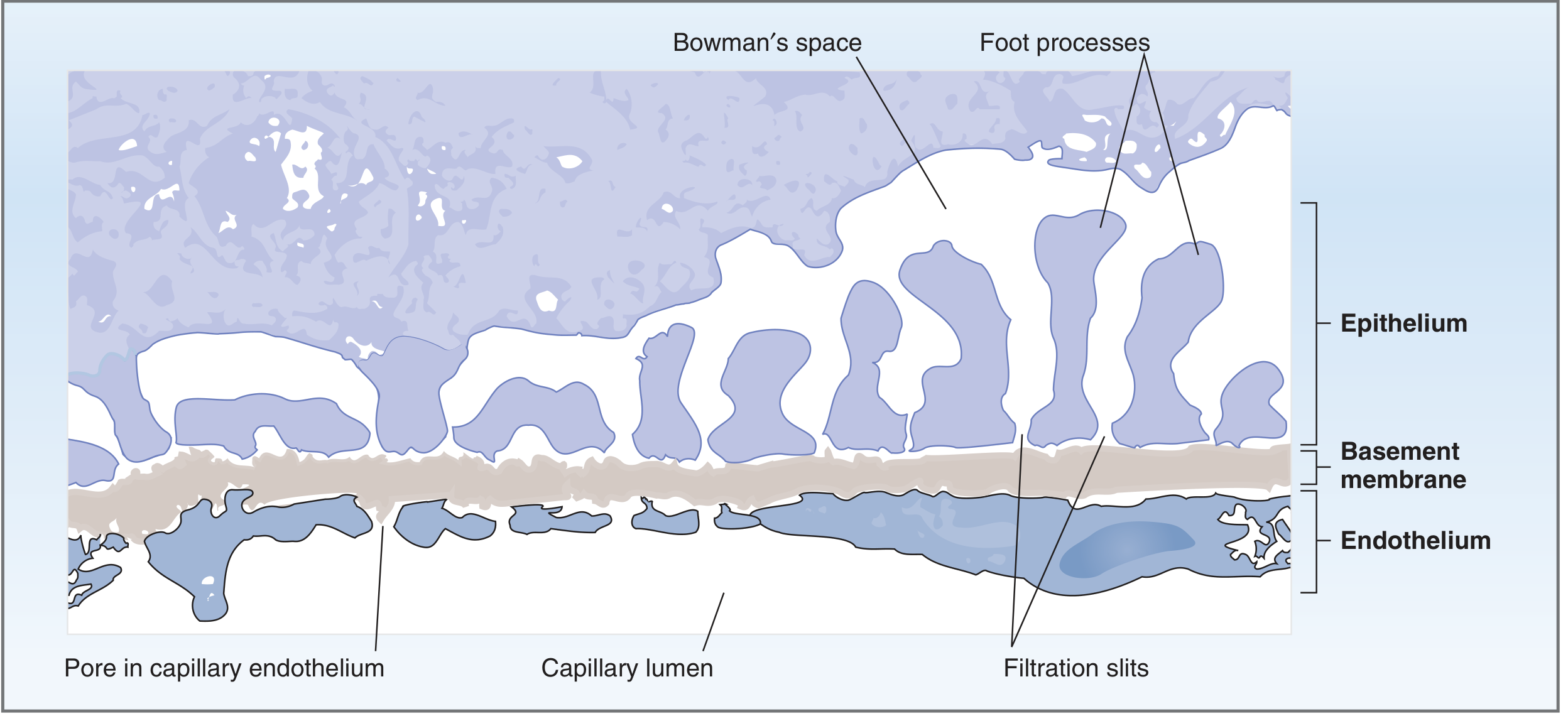
Fig. 6.9 - Structure of the glomerular capillary wall (Costanzo Physiology)
Components of the Barrier
The filtration barrier, moving from the capillary lumen outward toward Bowman's space, consists of:
1. Fenestrated Glomerular Endothelium
- Glomerular capillary endothelial cells are perforated by fenestrations 70-100 nm in diameter (larger, more numerous, and more irregular than fenestrations in other capillaries).
- Unlike fenestrae elsewhere, these lack a bridging diaphragm, allowing free passage of fluid and all plasma solutes.
- Blood cells (too large) are retained; plasma proteins pass through.
- Endothelial cells express large numbers of aquaporin-1 (AQP-1) water channels, enabling rapid water flux.
- The luminal surface is covered by a glycocalyx - a meshwork of glycosaminoglycans (including heparan sulfate proteoglycans) that bridges the fenestrations and acts as the initial coarse barrier to macromolecules.
- Endothelial products (nitric oxide, prostaglandin E2) are implicated in thrombotic glomerular diseases.
2. Glomerular Basement Membrane (GBM)
The GBM is a thick (300-370 nm) basal lamina - the thickest in the body - and is the joint product of both the endothelium and the podocytes. It has three sub-layers:
| Layer | Location | Role |
|---|---|---|
| Lamina rara interna | Fused to endothelium | Charged, initial exclusion |
| Lamina densa | Central | Main physical barrier |
| Lamina rara externa | Fused to podocytes | Charged exclusion |
Composition:
- Type IV collagen (primarily α3, α4, α5 chains) - the structural scaffold
- Laminin, nidogen/entactin
- Heparan sulfate proteoglycans (agrin, perlecan) - provide strong negative charge
- Multiadhesive glycoproteins
The GBM accounts for approximately 50% of total hydraulic resistance across the barrier. It is also the most significant barrier to plasma proteins.
Clinical relevance:
- Alport syndrome - mutations in genes encoding the α3, α4, α5 chains of type IV collagen → irregularly thickened, laminated GBM → hematuria, proteinuria, progressive renal failure
- Goodpasture syndrome - autoantibodies against the NCI domain of α3-chain of type IV collagen → rapidly progressive glomerulonephritis
3. Podocytes and Slit Diaphragms (Visceral Epithelial Layer)
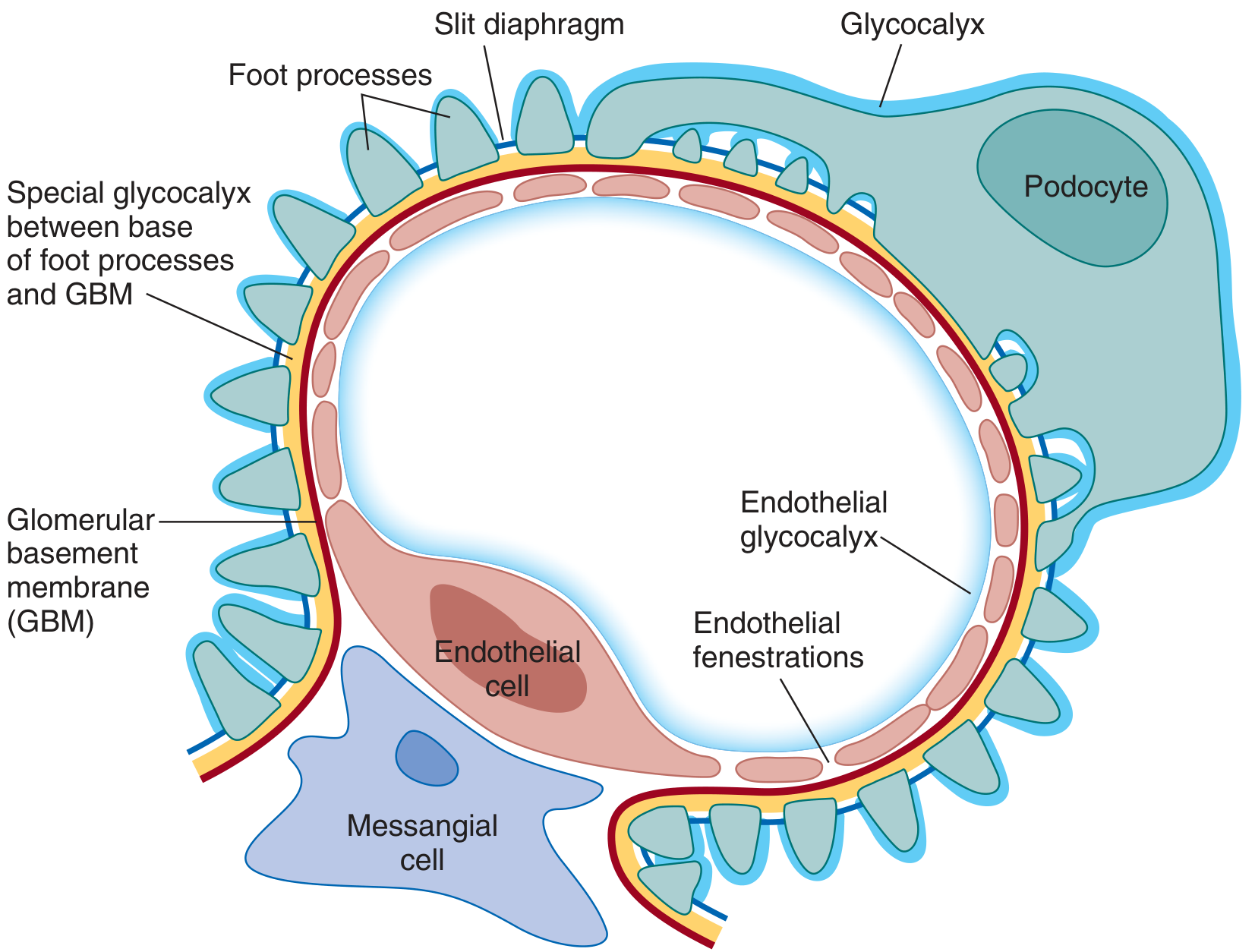
Fig. 3.12 - Full filtration barrier components including glycocalyx, GBM, foot processes, and slit diaphragm (Brenner and Rector's The Kidney)
Podocytes are highly differentiated, mesenchymal-derived visceral epithelial cells that reside in the urinary space and embrace the capillaries with an elaborate cytoskeletal architecture:
- Cell body extends long major processes
- Major processes give rise to secondary foot processes, which interdigitate in a "zipper-like" fashion with those of adjacent podocytes
- Foot processes attach to the GBM via integrins, syndecans, dystroglycan, and other adhesion receptors
- The apical surface is coated with podocalyxin (a sialomucin with strong negative charge) that keeps adjacent foot processes separated, maintaining the open filtration barrier
The Slit Diaphragm:
The gaps between interdigitating foot processes are 25-60 nm wide (filtration slits) and are bridged by the slit diaphragm - the ultimate barrier to macromolecules. It is not simply a thin membrane but a multi-layered, flexible structure combining features of tight junctions, adherens junctions, and gap junctions.
Key molecular components:
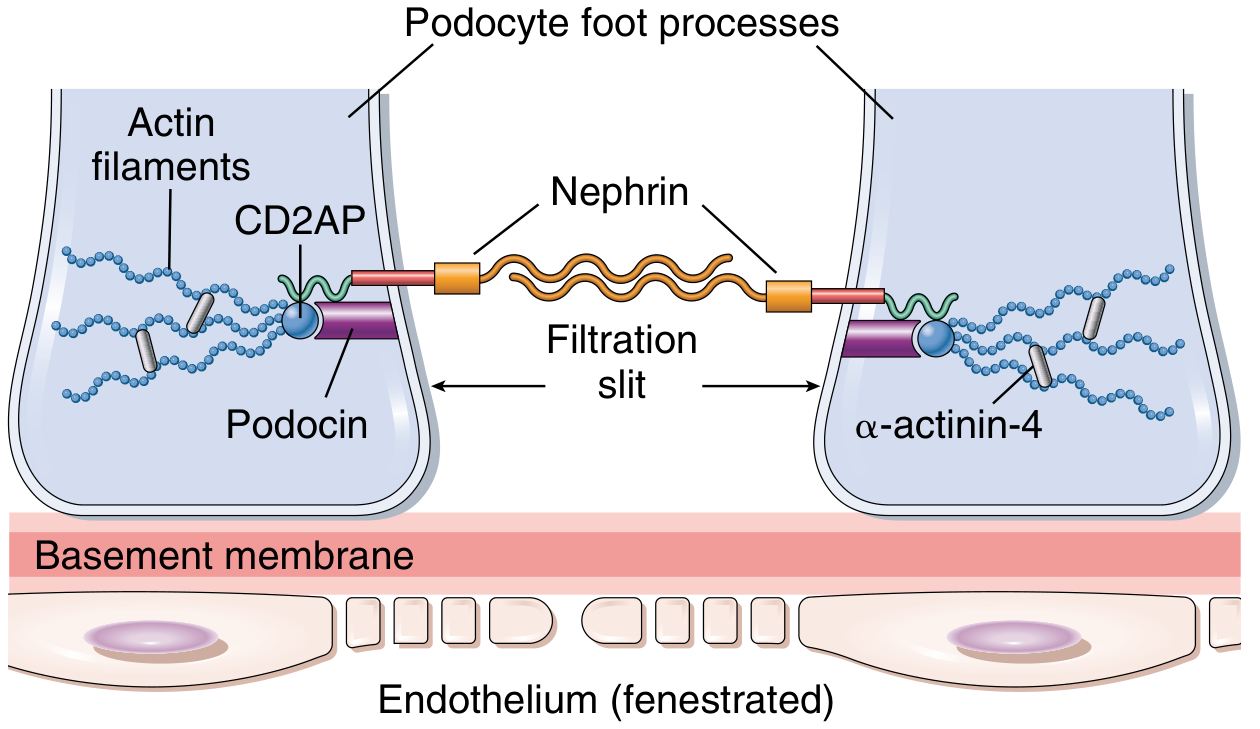
Fig. 20.4 - Molecular structure of the slit diaphragm
| Protein | Gene | Role |
|---|---|---|
| Nephrin | NPHS1 | Core structural protein spanning the slit; immunoglobulin superfamily |
| Neph1 | NEPH1 | Bipartite assembly with nephrin; spans lower part of slit near GBM |
| Podocin | NPHS2 | Anchors nephrin to membrane via lipid rafts; signaling hub; interacts with CD2AP |
| CD2AP | CD2AP | Adaptor linking slit diaphragm to actin cytoskeleton |
| α-actinin-4 | ACTN4 | Links to actin cytoskeleton |
| ZO-1, JAM4 | - | Tight junction components |
| P-cadherin, FAT1 | - | Adherens junction components |
The foot process actin cytoskeleton (actin + α-actinin-4 + myosin) forms a contractile system that is regulated by synaptopodin and rho GTPases, allowing plasticity of the filtration network.
Clinical relevance of slit diaphragm proteins:
- Congenital nephrotic syndrome of the Finnish type - mutations in NPHS1 (nephrin) → massive proteinuria from birth
- Steroid-resistant nephrotic syndrome (SRNS) - mutations in NPHS2 (podocin)
- Focal segmental glomerulosclerosis (FSGS) - mutations in ACTN4 (α-actinin-4) or TRPC6
Functional Properties - Size and Charge Selectivity
Size Selectivity
| Molecule radius | Filterability |
|---|---|
| < 20 Å (water, glucose, electrolytes, amino acids) | Freely filtered |
| ~35 Å (inulin) | Freely filtered |
| ~36 Å (neutral dextran) | Partially restricted |
| ~50 Å and above (albumin) | Almost completely excluded |
Mathematical modeling shows that macromolecular sieving is determined largely by the combination of slit diaphragms and GBM; the endothelium provides only ~2% of hydraulic resistance.
Charge Selectivity
Fixed negative charges are present throughout the barrier:
- Glycocalyx on endothelium
- Lamina rara interna and externa (heparan sulfate)
- Podocalyxin on podocytes
- Slit diaphragm region
Consequences:
- At physiologic pH, plasma proteins (including albumin) carry a net negative charge - they are repelled, reducing filtration beyond what size alone would predict
- Positively charged solutes are attracted and more readily filtered
- Negatively charged solutes are repelled and less readily filtered
- For small ions (Na+, K+, Cl-, HCO3-), charge has no practical effect - they pass freely regardless of charge
In minimal change disease (MCD), the leading mechanism is loss of anionic charges from the GFB (not physical disruption of the barrier), causing selective proteinuria - mainly albumin (which is normally charge-repelled) - while the GBM and podocyte architecture remain grossly intact on light microscopy.
Filtration Driving Forces (Starling Equation)
GFR is governed by:
GFR = K_f × [(P_GC - P_BS) - π_GC]
Where:
- K_f = filtration coefficient (hydraulic conductivity × surface area)
- P_GC = glomerular capillary hydrostatic pressure (~55 mmHg) → favors filtration
- P_BS = Bowman's space hydrostatic pressure (~15 mmHg) → opposes filtration
- π_GC = glomerular capillary oncotic pressure (~30 mmHg) → opposes filtration
- π_BS ≈ 0 (negligible protein in filtrate)
Net filtration pressure ≈ 55 - 15 - 30 = ~10 mmHg
Summary of Layers
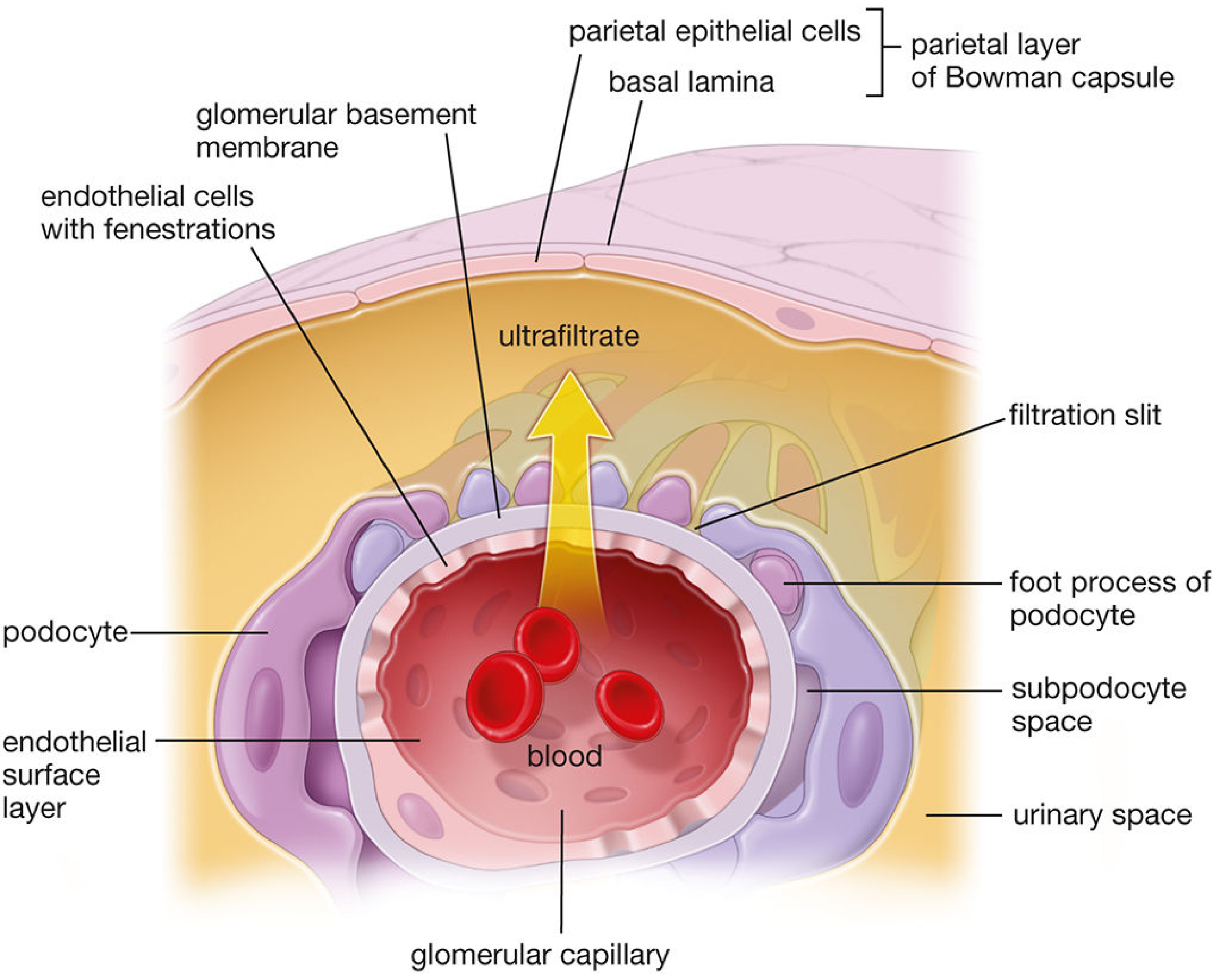
Schematic of filtration barrier showing movement of ultrafiltrate from capillary lumen through fenestrated endothelium, GBM, and podocyte foot processes into the urinary space
| Layer | Pore/Slit Size | Primary Function |
|---|---|---|
| Endothelial glycocalyx | Mesh ~20 nm | Initial coarse barrier; charge |
| Fenestrated endothelium | 70-100 nm | Retains blood cells; allows all plasma components |
| GBM (3 sub-layers) | ~50 Å effective | Main size and charge barrier for proteins; ~50% hydraulic resistance |
| Slit diaphragm | 25-60 nm slit | Ultimate barrier; primary determinant of protein permeability |
Sources:
- Costanzo Physiology, 7th ed., pp. 267-268
- Brenner and Rector's The Kidney, pp. 144-145, 4552-4554
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, pp. 1867-1870
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Fig. 20.4
- Medical Physiology (Boron & Boulpaep), p. 1104
This is a shared conversation. Sign in to Orris to start your own chat.