Teach me carple tunnel syndrome
Reading File
Finding Sources
Searching PubMed
"carpal tunnel syndrome"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full teaching response.
Carpal Tunnel Syndrome (CTS)
What Is It?
Carpal tunnel syndrome is the most common entrapment neuropathy in the upper extremity, first described by Paget in 1854. It results from compression of the median nerve as it passes through the carpal tunnel at the wrist. It affects up to 10% of the U.S. population and is twice as common in women as men, with peak incidence between ages 40-60.
Anatomy of the Carpal Tunnel
The carpal tunnel is a tight, rigid space:
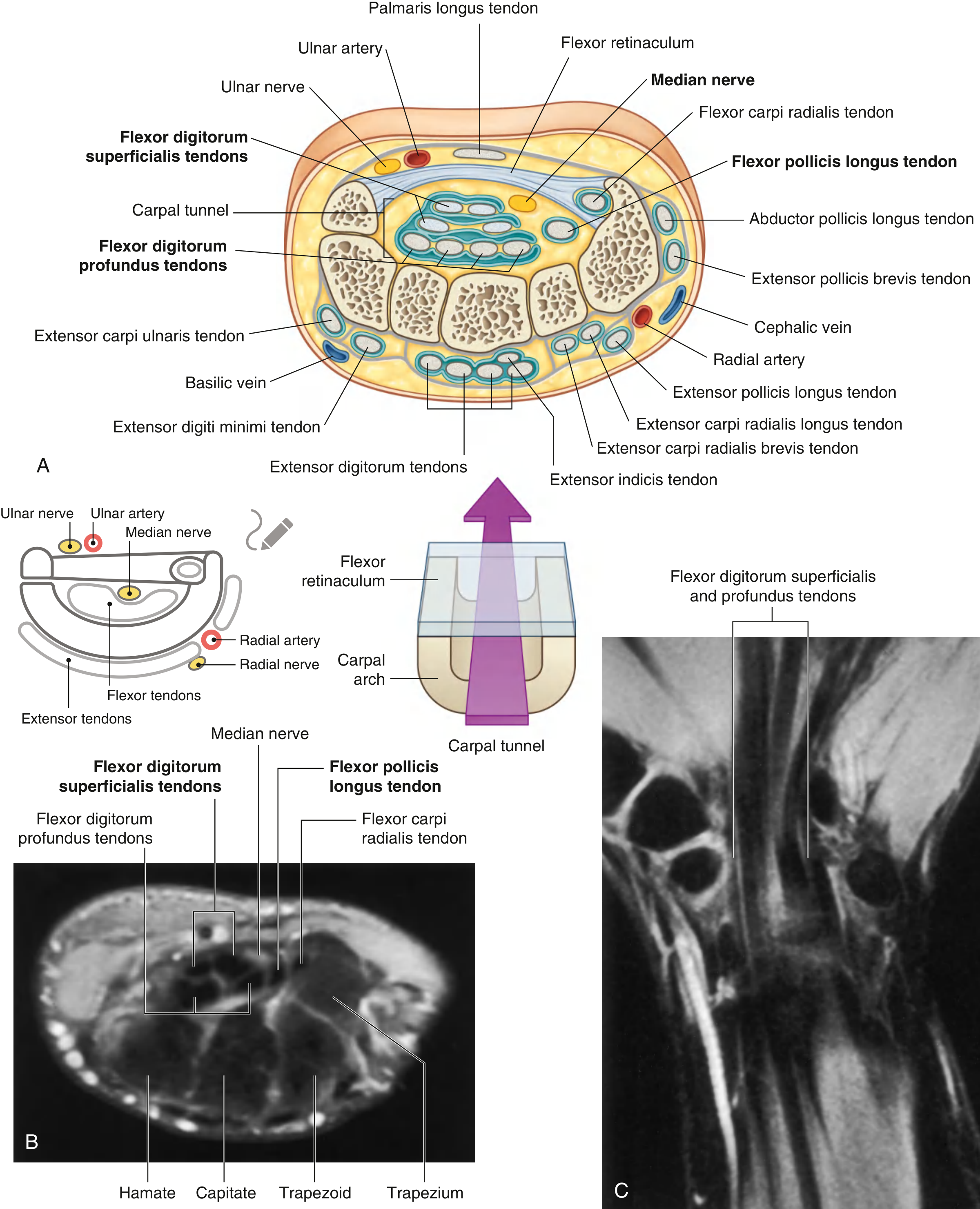
Fig. 7.98 - Gray's Anatomy for Students: Cross-section (A), Axial MRI (B), and Coronal MRI (C) of the carpal tunnel.
Boundaries:
- Floor/sides: Arching carpal bones (hamate, pisiform medially; scaphoid tubercle, trapezial ridge laterally)
- Roof: Flexor retinaculum (transverse carpal ligament, TCL)
Contents (10 structures total):
- The median nerve - the most palmar (superficial) structure in the tunnel
- Nine flexor tendons lying dorsal to the nerve: 4x flexor digitorum superficialis, 4x flexor digitorum profundus, 1x flexor pollicis longus
Key anatomical point: The palmar cutaneous branch of the median nerve exits proximal to the flexor retinaculum, so CTS causes numbness in the distal thumb, index, and middle fingers but NOT over the thenar eminence itself - a useful diagnostic clue.
- Goldman-Cecil Medicine, p. 4088
- Gray's Anatomy for Students, p. 920
Pathophysiology
Elevated carpal tunnel pressure (>20-30 mmHg) impedes epineurial blood flow. This causes:
- Venous congestion
- Nerve edema
- Anoxic damage to capillary endothelium of the median nerve
- Progressive demyelination and, in severe cases, axonal loss
- Gray's Anatomy for Students, p. 920
- Campbell's Operative Orthopaedics 15e, p. 4502
Causes and Risk Factors
| Category | Examples |
|---|---|
| Patient factors | Female sex, obesity, physical inactivity, smoking |
| Decrease in tunnel size | Bony abnormalities, acromegaly, wrist flexion/extension |
| Increase in tunnel contents | Colles fracture, lunate dislocation, osteophytes, hypertrophic synovium, hematoma |
| Inflammatory conditions | Rheumatoid arthritis, gout, nonspecific tenosynovitis, infection |
| Fluid balance alterations | Pregnancy, menopause, hypothyroidism, renal failure, hemodialysis, eclampsia |
| Neuropathic conditions | Diabetes mellitus, double-crush syndrome, alcoholism, industrial solvents |
| Occupational | Repetitive stress (e.g., typing) |
| Systemic diseases | Congestive heart failure, multiple myeloma, TB, sarcoidosis, amyloidosis |
The cause is idiopathic in most cases. Work association is difficult to substantiate, and non-dominant hand involvement is frequent.
- Campbell's Operative Orthopaedics 15e, p. 4503
- Firestein & Kelley's Textbook of Rheumatology, p. XXX
Clinical Features
Symptoms
- Paresthesia (tingling/numbness) in the thumb, index, and middle fingers (+/- radial half of ring finger) - classic median nerve distribution
- Nocturnal symptoms are hallmark - waking the patient at night
- Relief by shaking or elevating the hand ("flick sign")
- Diffuse aching or throbbing pain radiating up the forearm
- Occasionally proximal symptoms including shoulder pain
- In severe/late cases: thenar muscle atrophy and weakness (abductor pollicis brevis, opponens pollicis)
- Subjective numbness can spread to the whole hand (even ulnar distribution) - this does not exclude CTS
Signs
| Finding | Details |
|---|---|
| Thenar atrophy | Abductor pollicis brevis - late sign, indicates advanced compression |
| Sensory loss | Distal thumb, index, middle finger; thenar eminence is SPARED |
| Weakness | Thumb abduction and opposition (opponens weakness can be masked by recruitment of long flexors) |
- Bradley and Daroff's Neurology in Clinical Practice, p. 549
- Firestein & Kelley's Rheumatology, p. XXX
Provocative Tests
| Test | Method | Sensitivity | Specificity |
|---|---|---|---|
| Phalen test | Sustained wrist flexion for 1-2 minutes; reproduction of symptoms is positive | ~74% | Moderate (~25% false positive rate) |
| Tinel sign | Gentle percussion over the volar wrist (median nerve); radiating paresthesia is positive | Lower | Higher (most specific) |
| Durkan (carpal compression) test | Direct compression of median nerve with thumbs for 30 seconds | 87% | 90% - best overall |
| CTS-6 score | Clinical scoring tool using 6 history/exam items; score ≥12 has 95% sensitivity, 91% specificity | 95% | 91% |
The CTS-6 is as sensitive and specific as EMG/nerve conduction studies (NCS) and is free, non-invasive, and immediate.
- Campbell's Operative Orthopaedics 15e, p. 4502
Investigations
Nerve Conduction Studies (NCS) + EMG
- Gold standard for confirmation
- Abnormal values: distal motor latency >4.5 ms, sensory latency >3.5 ms
- EMG may show: increased insertional activity, positive sharp waves, fibrillations at rest, decreased motor recruitment
- NCS: 90% sensitive, 60% specific
- Important caveat: Studies can be normal in symptomatic patients and abnormal in asymptomatic patients. They are not predictors of functional recovery post-surgery.
- Useful for ruling out cervical radiculopathy, thoracic outlet syndrome, and proximal nerve compression
Ultrasound
- Increasingly used; can show median nerve enlargement (cross-sectional area) at the wrist
- High sensitivity/specificity comparable to NCS in many studies
Blood tests to screen for secondary causes
All patients should be checked for: diabetes, hypothyroidism, rheumatoid arthritis, acromegaly, sarcoidosis, gout, amyloidosis
- Campbell's Operative Orthopaedics 15e, p. 4503
- Bradley and Daroff's Neurology, p. 549
Differential Diagnosis
- Cervical disc disease / radiculopathy (C6/C7)
- Thoracic outlet syndrome
- Diabetic or other peripheral neuropathy
- Pronator teres syndrome (median nerve compression at elbow)
- Autoimmune/inflammatory conditions
Treatment
Conservative (First-line)
1. Wrist splinting (neutral position)
- Best used at night to prevent provocative wrist positioning
- Should hold wrist at neutral to 10 degrees extension - NOT hyperextension
- Use sparingly during the day to avoid secondary muscle weakness
- Effective for mild cases; long-term benefit is limited
2. NSAIDs - for pain control
3. Corticosteroid injection
- Methylprednisolone injection into the carpal tunnel
- Highly effective short-term; long-term efficacy is mixed
- Risk of median nerve injury if performed incorrectly
- Best reserved for: pregnancy-related CTS, or when surgery must be temporarily deferred
4. 5% dextrose injection - evidence of benefit comparable to steroid injections (per Goldman-Cecil)
5. Vitamin B6 (100-200 mg/day) - some clinical benefit reported but not confirmed in RCTs
6. Activity modification - reduce repetitive wrist movements, ergonomic adjustments
7. Ultrasound-guided nerve hydrodissection - emerging technique with growing evidence (2025 systematic review, PMID 39894044)
Surgical (Definitive)
Indications for surgery:
- Failed conservative treatment
- Objective sensory loss (late finding) - prompt early referral
- Thenar atrophy (late finding) - prompt early referral
- Severe electrodiagnostic abnormalities
Types of carpal tunnel release:
| Approach | Description |
|---|---|
| Open release | Incision ≤3 cm paralleling palm skin creases; direct visualization of TCL |
| Endoscopic release | 1-2 small portal incisions; generally preferred (faster recovery, less scar tenderness) |
| Ultrasound-guided percutaneous release | Newer minimally-invasive technique |
-
Surgery is highly effective, with most patients obtaining relief
-
Endoscopic approach is generally preferred over open
-
Revision surgery is occasionally needed for recurrent symptoms
-
Firestein & Kelley's Rheumatology, p. XXX
-
Goldman-Cecil Medicine, p. 4088
-
Campbell's Operative Orthopaedics 15e, p. 4502
Special Populations
Pregnancy
- CTS is common in pregnancy (fluid retention increases tunnel pressure)
- Usually resolves spontaneously after delivery
- Corticosteroid injection is reasonable if symptoms are severe
- Goldman-Cecil Medicine, p. 4088
Children
- CTS is unusual in children
- Associated with: congenital bone abnormalities, hypothyroidism, lysosomal storage disease, myopathic contractures, or strong family history
- Symptoms differ: decreased dexterity, diffuse pain, absent Phalen/Tinel in late stages
Summary: Clinical Approach
SUSPECT CTS:
Nocturnal hand tingling + median nerve distribution + flick sign
↓
EXAMINE:
Phalen / Tinel / Durkan test + thenar atrophy + CTS-6 score
↓
SCREEN BLOODS:
TFTs, fasting glucose, FBC, CRP, RF (exclude secondary causes)
↓
CONFIRM (if needed):
NCS/EMG or wrist ultrasound
↓
TREAT:
Mild-Moderate: Night splint ± NSAIDs → corticosteroid injection if inadequate
Severe/refractory/atrophy: Surgical release (endoscopic preferred)
Recent Evidence (2025)
Two recent systematic reviews and a network meta-analysis confirm the current approach:
- Conservative treatments comparison (splints, injections, physiotherapy, hydrodissection): PMID 40315975
- Ultrasound-guided nerve hydrodissection outperforms some conservative options: PMID 39894044
- Neurodynamic tests (Phalen, Tinel) have moderate diagnostic accuracy: PMID 40156954
Sources: Goldman-Cecil Medicine (International Ed.), Bradley and Daroff's Neurology in Clinical Practice, Gray's Anatomy for Students, Firestein & Kelley's Textbook of Rheumatology, Campbell's Operative Orthopaedics 15e (2026), Creasy & Resnik's Maternal-Fetal Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.