
Screenshot_20260621-135340.png
Explain adernal insufficiency
Reading File
Finding Sources
Searching PubMed
"adrenal insufficiency"[MeSH Terms] AND diagnosis
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all I need to write a comprehensive answer. Here it is:
Adrenal Insufficiency (PA 31.8)
Overview
Adrenal insufficiency (AI) is the failure of the adrenal glands to produce adequate amounts of glucocorticoids, with or without mineralocorticoid or androgen deficiency. It is potentially life-threatening. Prevalence of non-iatrogenic AI is approximately 100 per million population. - Goldman-Cecil Medicine
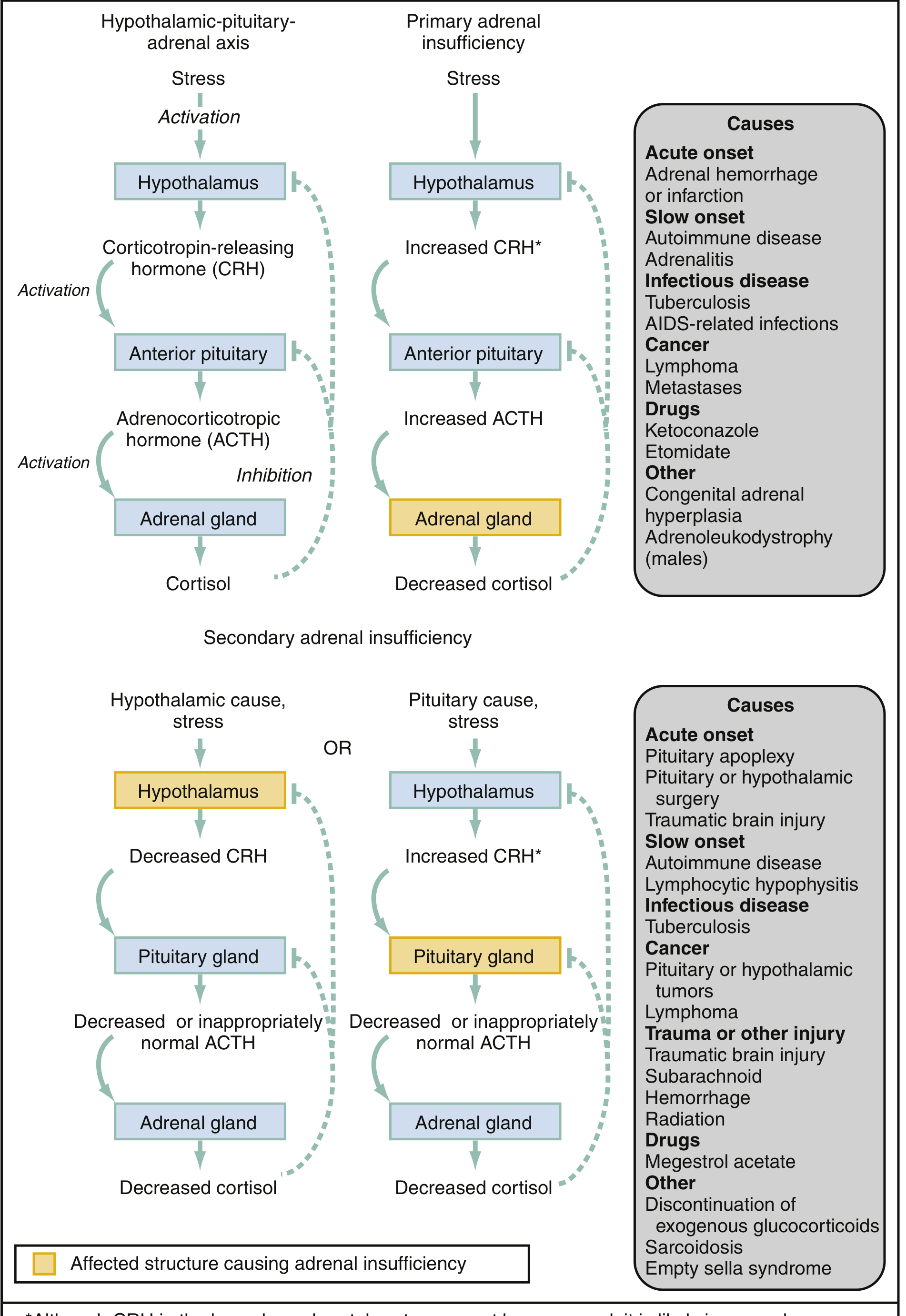
Types: Primary, Secondary, and Tertiary
The distinction is based on where in the HPA axis the problem lies:
| Type | Site of Lesion | ACTH | Cortisol | Aldosterone |
|---|---|---|---|---|
| Primary (Addison's disease) | Adrenal gland | High (no negative feedback) | Low | Low |
| Secondary | Anterior pituitary (low ACTH) | Low/inappropriately normal | Low | Near normal |
| Tertiary | Hypothalamus (low CRH) | Low | Low | Normal |
Etiology
Primary Adrenal Insufficiency
Chronic causes:
- Autoimmune adrenalitis - most common in industrialized countries; may occur in isolation or as part of Autoimmune Polyglandular Syndrome type 1 (with hypoparathyroidism + mucocutaneous candidiasis) or type 2 (with type 1 DM, autoimmune thyroid disease, vitiligo)
- Infections - tuberculosis is classic; also histoplasmosis, coccidioidomycosis, blastomycosis; CMV or MAI in AIDS
- Bilateral metastases - lung, breast, kidney, gut primaries; primary lymphoma
- Adrenoleukodystrophy - X-linked; deficiency of peroxisomal membrane protein leads to accumulation of very long chain fatty acids (VLCFA), which impair ACTH signal transduction in the adrenal cortex
- Congenital adrenal hyperplasia (CAH) - enzyme deficiency (CYP21A2, CYP11B1) prevents cortisol synthesis
- Drugs - ketoconazole, etomidate, rifampicin
- Sarcoidosis, amyloidosis, hemochromatosis (infiltrative)
Acute causes:
- Adrenal hemorrhage (Waterhouse-Friderichsen syndrome in meningococcemia; also anticoagulation, antiphospholipid syndrome, trauma)
Secondary Adrenal Insufficiency
- Pituitary tumor, surgery, or irradiation
- Sheehan syndrome (postpartum pituitary necrosis)
- Pituitary apoplexy
- Lymphocytic hypophysitis
- Most common overall cause: exogenous glucocorticoid use - suppresses the HPA axis (tertiary mechanism)
- Traumatic brain injury, empty sella syndrome, sarcoidosis
Pathogenesis
Normal HPA axis: Hypothalamus releases CRH -> anterior pituitary releases ACTH -> adrenal cortex produces:
- Cortisol (zona fasciculata) - glucocorticoid; regulates carbohydrate, protein, and lipid metabolism
- Aldosterone (zona glomerulosa) - mineralocorticoid; regulates Na/K and fluid balance
- DHEA (zona reticularis) - androgen
In primary AI, destruction of the entire adrenal cortex causes low cortisol + low aldosterone + low DHEA. The loss of cortisol negative feedback leads to markedly elevated CRH and ACTH. The elevated ACTH also stimulates melanocyte-stimulating hormone (MSH) production (both derived from POMC), causing hyperpigmentation.
In secondary AI, low ACTH fails to stimulate the adrenal gland. Aldosterone is relatively spared (mainly regulated by the renin-angiotensin system, not ACTH). No excess ACTH/MSH, so no hyperpigmentation; in fact, skin may appear pale ("alabaster skin").
Clinical Manifestations
Chronic Adrenal Insufficiency
From glucocorticoid deficiency (both primary and secondary):
- Fatigue, weakness, lack of energy
- Weight loss, anorexia
- Nausea, vomiting, abdominal pain
- Myalgia, arthralgia
- Hypoglycemia (especially in children)
- Low blood pressure, postural hypotension
- Hyponatremia (loss of cortisol inhibition of AVP -> water retention)
- Mild fever
- Normochromic anemia, lymphocytosis, eosinophilia
From mineralocorticoid deficiency (PRIMARY only):
- Salt craving
- Orthostatic hypotension, syncope
- Hyperkalemia
- Hyperchloremia and metabolic acidosis
- Elevated serum creatinine (volume depletion)
From androgen deficiency:
- Loss of axillary and pubic hair (especially in women)
- Loss of libido (in women)
- Dry, itchy skin (in women)
Specific to Primary AI:
- Hyperpigmentation - sun-exposed areas, areas of friction/pressure, buccal mucosa (due to excess POMC-derived MSH)
- Vitiligo (autoimmune association)
Specific to Secondary AI:
- Pale "alabaster" skin (low POMC peptides)
- Amenorrhea
- Decreased libido, impotence
- Loss of axillary and pubic hair
Acute Adrenal Crisis
- Refractory hypotension and shock - hallmark; does not respond to fluids or vasopressors
- Fever
- Abdominal pain (can mimic acute abdomen)
- Severe nausea, vomiting
- Hypoglycemia
Laboratory Features
| Test | Primary AI | Secondary AI |
|---|---|---|
| Serum cortisol | Low | Low |
| Plasma ACTH | High (>2x normal) | Low or inappropriately normal |
| Aldosterone | Low | Normal |
| Plasma renin | High | Normal |
| Sodium | Low (hyponatremia) | Low (hyponatremia) |
| Potassium | High (hyperkalemia) | Normal |
| Blood glucose | Low | Low |
Confirmatory test: ACTH stimulation test (cosyntropin/Synacthen test) - administer 250 mcg ACTH IV and measure cortisol at 30 and 60 minutes. A peak cortisol <500 nmol/L (18 mcg/dL) is diagnostic of AI. The insulin tolerance test (ITT) is the gold standard for secondary AI but is more invasive.
Additional workup in primary AI:
- Anti-21-hydroxylase antibodies - positive in most autoimmune cases
- Plasma VLCFA (C26:0) in males with negative antibodies - to exclude adrenoleukodystrophy
- Adrenal CT - to look for hemorrhage, granulomas, metastases, or masses
- Screen for other autoimmune endocrinopathies (thyroid, diabetes)
Morphologic Features
- Autoimmune AI: Atrophic adrenal glands with lymphocytic infiltration; normal architecture replaced by fibrosis
- TB/granulomatous: Caseating granulomas replacing adrenal tissue; often calcified on imaging
- Hemorrhagic: Blood-filled or necrotic adrenal glands (bilateral); classic Waterhouse-Friderichsen syndrome shows massive bilateral hemorrhage
- Metastatic: Bilateral adrenal enlargement with tumor replacement
- Adrenoleukodystrophy: VLCFA accumulation in adrenal cortex cells; also demyelination in CNS
Complications
- Adrenal crisis - life-threatening acute decompensation; triggers include infection, surgery, trauma, vomiting/diarrhea (inability to take oral steroids)
- Cardiovascular collapse and death if untreated
- Chronic morbidity: reduced quality of life, fatigue, impaired stress response
- Hypoglycemia (especially in children)
- Increased susceptibility to infections
Treatment
Acute Adrenal Crisis (Emergency)
- Hydrocortisone 100 mg IV immediately (has both glucocorticoid and mineralocorticoid activity)
- IV normal saline for volume expansion
- IV dextrose for hypoglycemia
- Vasopressors if needed
- Alternative: Dexamethasone 4 mg IV (does not interfere with serum cortisol assays - useful if diagnosis not yet confirmed)
Chronic Replacement
- Glucocorticoid: Hydrocortisone 10-12 mg/m²/day orally in 1-3 divided doses (mimicking diurnal cortisol rhythm - two-thirds in morning, one-third in afternoon). Prednisone 4-7 mg/day is an alternative
- Mineralocorticoid (primary AI only): Fludrocortisone 50-300 mcg/day; dose adjusted to normalize plasma renin activity; encourage salt intake
- Sick-day rules: Double or triple the glucocorticoid dose during fever, illness, or minor procedures; 100 mg hydrocortisone IV for surgery or major stress
Key Distinguishing Points
| Feature | Primary AI | Secondary AI |
|---|---|---|
| Hyperpigmentation | Yes (excess ACTH/MSH) | No (pale skin) |
| Mineralocorticoid deficiency | Yes | No |
| Hyperkalemia | Yes | No |
| ACTH | High | Low |
| Renin | High | Normal |
| Cause | Adrenal gland disease | Pituitary/hypothalamic disease |
Recent evidence (2026): A systematic review on glucocorticoid-induced AI (PMID 41521083) confirmed that systemic glucocorticoid therapy is a major cause of adrenal insufficiency. A 2025 meta-analysis (PMID 40587340) specifically addressed evaluation and management of glucocorticoid-induced AI in IBD patients. These do not alter the classic framework above but reinforce the importance of iatrogenic AI in clinical practice.
Sources: Goldman-Cecil Medicine, Harrison's Principles of Internal Medicine 22E, Rosen's Emergency Medicine, Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.